The database details criminality over 157 years until 1936, as well as chronicling the lives of some of the justice system’s more notorious enforcers
If death is the final taboo, it might not be for much longer. There has, in recent years, been increasing effort to promote conversations about death and dying, both in the home and in more public settings. For example, death cafes, first launched in Switzerland in 2004, have spread around the world, enabling people to speak about their fears over cake and coffee.
Our reluctance to talk about death is often taken as evidence that we are afraid, and therefore suppress thoughts about it. However, there is little direct evidence to support that we are. So what is a “normal” amount of death anxiety? And how does it manifest itself?
Experimenting with death
Judging by studies using questionnaires, we seem more bothered by the prospect of losing our loved ones than we do about dying ourselves. Such studies also show that we worry more about the dying process – the pain and loneliness involved, for example – than about the end of life itself. In general, when we are asked if we are afraid to die, most of us deny it, and report only mild levels of anxiety. The minority who report high levels of death anxiety are even considered psychologically abnormal – thanatophobic – and recommended for treatment.
On the other hand, our tendency to report only low levels of death anxiety might be a result of our reluctance to admit to our fear, to others and ourselves. Based on this hypothesis, social psychologists have, for almost 30 years now, examined the social and psychological effects of being confronted with our own mortality. In well over 200 experiments, individuals have been instructed to imagine themselves dying.
What’s worse: the death of a loved one or facing our own death?
The first study of this kind was conducted on US municipal court judges, who were asked to set bond for an alleged prostitute in a hypothetical scenario. On average, judges who were confronted with their mortality beforehand set a much higher bail than those who were were not confronted – $455 versus $50. Since then, many other effects have been found among groups including the general population in many different countries.
Besides making us more punitive, thinking about death also increases our nationalistic bias, makes us more prejudiced against other racial, religious and age groups, and leads to other such parochial attitudes. Taken together, these dozens of studies show that being reminded of death strengthens our ties to the groups we belong to, to the detriment of those who are different from us.
Reminders of death also affect our political andreligious beliefs in interesting ways. On the one hand, they polarise us: political liberals become more liberal while conservatives become more conservative. Similarly, religious people tend to assert their beliefs more fervently while nonreligious people disavow more.
On the other hand, these studies have also found that thinking about death tempts us all – religious or otherwise – towards more religious belief in subtle, perhaps unconscious ways. And when the reminder of death is sufficiently powerful and when participants are not mindful of their prior political commitments, liberals as well as conservatives tend to endorse conservative ideas and candidates. Some researchersclaim that this could explain the US political shift to the right after 9/11.
What do the results mean?
But why does the prospect of death make us more punitive, conservative and religious? According to many theorists,reminders of death compel us to seek immortality. Many religions offer literal immortality, but our secular affiliations – such as our nation states and ethnic groups – can provide symbolic immortality. These groups and their traditions are a part of who we are, and they outlive us. Defending our cultural norms can boost our sense of belonging and being more punitive against individuals who violate cultural norms – such as prostitutes – is symptom of this.
Consistent with this interpretation, researchers have also found that reminders of death increase our desire for fame and for children, both of which are commonly associated with symbolic immortality. It turns out that we do want to be immortalised through our work and our DNA.
Thinking about death makes us dream of being famous.
When asked, we do not seem, perhaps not even to ourselves, to fear death. Nor would we guess that thinking about death has such widespread effects on our social attitudes. But there are limits to our introspective powers. We are notoriously bad at predicting how we will feel or behave in some future scenario, and we are similarly bad at working out why we feel the way we do, or evenwhy we have behaved a certain way. So, whether we realise it or not, it seems that to bring death to the surface of our minds is to open Pandora’s box.
So what should we make of these new efforts to demystify death and dying through conversation? It is hard to say. Increasing death’s profile in our imaginations, private and public, might make us all more punitive and prejudiced, as the research found. But then perhaps we get these negative effects precisely because we are unaccustomed to thinking and talking about death.
In exposure therapy, carefully exposing patients to the source of their anxiety – an object, an animal, or even a memory – reduces their fear. In the same way, perhaps this most recent taboo-breaking trend will inoculate us psychologically, and make us more robust in the face of death.
An important process in the physiology of the human body after death, rigor mortis is one of the most reliable subjects of study to determine the time of death of a living being. In this article, we will learn more about this term, its causes, and its various stages.
What is Rigor Mortis and How is it Caused?
Within a few hours of death, the body of a person or animal gets stiff and locked in place. This phenomenon is called rigor mortis or postmortem rigidity. Medically, the term is defined as the temporary rigidity of body muscles occurring soon after death.
Rigor mortis occurs due to biochemical changes in muscle tissue, when the formation of an enzyme called ATP (Adenosine triphosphate) stops after death due to a lack of oxygen in the body. Since ATP provides energy for the muscles to move, this stoppage results in proteins such as myosin molecules sticking to actin filaments, causing contraction and stiffening the tissue. Depending on factors such as temperature, the condition can last for as long as 72 hours. The process is a valuable tool to death investigations, as studying the stage of rigor mortis of the body greatly narrows down the time frame of death.
Timeline and Stages
There are a lot of things to consider when examining rigor mortis to make any conclusive statements about a death. Under normal conditions, the process should follow a fixed timeline.
0 – 8 Hours After Death: Till around 10 minutes after death, the muscles in the body are relaxed. This state is called primary flaccidity, and any stiffening is absent. However, after this period, rigor mortis begins to set in gradually; the skin pales, and the body starts cooling (two degrees Celsius in the first hour; one degree each hour thereafter). Muscle stiffening is minimal during these hours, and the hair stands on end because the muscles start to push on the follicles. After 4 – 6 hours, the stiffening of the muscles becomes moderate, and spreads all around the body. At the end of this period, one may observe sporadic twitches in the muscles. At the end of eight hours, the body should have cooled completely.
8 – 12 Hours After Death: During this period, the stiffening of the muscles goes from a moderate to an advanced stage, and by the time 12 hours have passed, there is absolutely no flexibility in the muscles, and the skin gets discolored due to the collection of blood.
12 – 24 Hours After Death: The rigor mortis is now complete, and at its peak, and the body remains fully stiff for around 12 hours more. It is nearly impossible to move or manipulate any body part without applying a lot of force.
24 – 36 Hours After Death: The stiffness gradually begins to dissipate due to the degradation of proteins in the body, and by the end of the 36th hour, the muscles should have become pliable again. This is the time when undertakers in mortuaries begin the process of embalming dead bodies, and making them presentable for funerals by adjusting the body position appropriately, before putrefaction begins.
Factors Affecting Rigor Mortis
This timeline is appropriate only under regular conditions. However, there are a few factors which alter the timeline, and speed up or slow down the process:
Exercise Before Death: If a person is involved in strenuous activity just before death, rigor mortis sets in immediately. This is because, at the time of death, the working muscles were depleted of ATP and oxygen.
Surrounding Ambient Temperatures: If death occurs under warm conditions, the conditions for decay and multiplication of bacteria are hospitable, increasing the pace of rigor mortis. However, if the person died in a cold environment, or of hypothermia, rigor mortis can last for many days. In these cases, one cannot use it to determine the time of death.
Fat Distribution: More fat in the body adds extra insulation, which causes the process of postmortem rigidity to slow down.
Disease and Age: People with low muscle mass, such as children, the elderly, or people suffering from diseases go through the process faster than those with high muscle mass. This is also true when comparing the rate of rigidity between humans and different animals, i.e., rigor mortis in a cat will set in faster than humans, while that of an elephant will be slower.
As you can see, this condition has great medico-legal importance, and gives investigative agencies a lot of information while looking at cases of suicides and murder.
Jon Henley with his father, mother and son in 2003
My father spent 10 days dying.
He was 84 and he had lost his wife – my mother, whom he adored, and without whom he felt life was a lot less worth living – three years earlier. He died of old age, and it was entirely natural.
The process, though, did not feel that way at all, at least not to me. Dad had been bedridden for months and was in a nursing home. He stopped eating one day, then started slipping in and out of consciousness. Soon he stopped drinking.
For 10 days my sister and I sat by his bedside, holding his hand, moistening his lips. Slowly his breathing changed, became more ragged. During the last few days, the tips of his fingers turned blue. His skin smelled different. His breath gradually became a rasp, then a rattle.
It sounded awful. We were sure he was in pain. The doctor reassured us he wasn’t; this was a human body dying naturally, shutting down, one bit at a time. We had not, of course, talked about any of this with Dad beforehand; we had no plans for this, no idea of what he might have wanted. It would have been a very difficult conversation.
The doctor said he could give him something that would make him at least sound better, but it would really be more for us than for my father. “My job,” the doctor said, “is about prolonging people’s lives. Anything I give to your father now would simply be prolonging his death.”
So we waited. When it finally came, death was quite sudden, and absolutely unmistakable. But those 10 days were hard.
Death is foreign to us now; most of us do not know what it looks, sounds and smells like. We certainly don’t like talking about it. In the early years of the 20th century, says Simon Chapman, director of policy and external affairs at the National Council for Palliative Care, 85% of people still died in their home, with their family.
By the early years of this century, fewer than 20% did. A big majority, 60%, died in hospital; 20% in care homes, like my father; 6% in hospices, like my mother. “Death became medicalised; a whole lot of taboos grew up around it,” Chapman says. “We’re trying now to break them down.”
The reports all, in fact, conclude pretty much the same thing: the need for end-of-life care that is coordinated among all the services, focused on the dying person’s needs and wishes, and delivered by competent, specially trained staff in (where possible) the place chosen by the patient – which for most people is, generally, home.
“It’s not just about the place, though that’s important and things are moving,” says Chapman: the number of people dying in hospital has now dropped below 50%.
“The quality of individual care has to be right, every time, because we only have one chance. It’s about recognising that every patient and situation is different; that communication is crucial; that both the patient and their family have to be involved. It can’t become a box-ticking exercise.”
Dying, death and bereavement need to be seen not as purely medical events, Chapman says: “It’s a truism, obviously, but the one certainty in life is that we’ll die. Everything else about our death, though, is uncertain. So we have to identify what’s important to people, and make sure it happens. Have proper conversations, and make proper plans.”
All this, he recognises, will require “a shift of resources, into the community” – and funding. Key will be the government’s response to What’s Important to Me, published last February by a seven-charity coalition and outlining exactly what was needed to provide full national choice in end-of-life care by 2020. It came with a price tag of £130m; the government is expected to respond before summer.
In the meantime, though, a lot of people – about half the roughly 480,000 who die in Britain each year – still die in hospital. And as an organisation that has long focused on curing patients, the NHS does not always have a framework for caring for the dying, Chapman says.
But in NHS hospitals too, much is changing. There has been a specialist palliative care service – as distinct from end-of-life care, which is in a sense “everyone’s business”, involving GPs, district nurses and other primary care services – at Southampton general hospital and its NHS-run hospice, Countess Mountbatten House, since 1995, says Carol Davis, lead consultant in palliative medicine and clinical end-of-life care lead.
People die in hospital essentially in five wards: emergency, respiratory, cancer, care of elderly people and intensive care, she says: “Our job is about alleviating patients’ suffering, while enabling patients and their families to make the right choices for them – working out what’s really important.”
Palliative care entails not just controlling symptoms, but looking after patients and their families and, often, difficult decisions: how likely is this patient get better? Is another operation appropriate? What would the patient want to happen now (assuming they can’t express themselves)? Has there been any kind of end-of-life planning?
Of course many patients in acute hospital care will not be able to go home to die, and some will not want to, Davis says: “Some simply can’t be cared for at home. If you need two care workers 24/7, it’s going to be hard. Others have been ill for so long, or in and out of hospital so often, they feel hospital is almost their second home. So yes, choice is good – but informed choice. The care has to be feasible.”
In 2014, the report One Chance to Get it Right [pdf] identified five priorities in end-of-life care: recognise, communicate, involve, support, and plan and do. (“Which could pretty much,” says Davis, “serve as a blueprint for all healthcare.”) The first – recognise, or diagnose – is rarely easy. How does a doctor know when a patient is starting to die?
“There are physical signs, of course,” says Davis. “Once the patient can’t move their limbs, or can no longer swallow.” But, she says, “we have patients who look well but are very ill, and others who look sick but are not. In frail elderly people – or frail young people – it can be hard to predict. Likewise, in patients with conditions like congenital heart disease, where something could happen almost at any moment.”
Quite often, Davis and her team face real doubts. “Right now,” she says, “I have a patient in intensive care, really very ill. They probably won’t pull through, but they might. I have another doing well, making excellent progress – but they’ve been in hospital for three months now. They’re very, very weak, and any sudden infection … You just can’t predict.”
Which is why communication, and planning, and involving the family – all those difficult and painful conversations that we naturally shy away from – are so very important.
It could well be, for example, that my father would actually have wanted his death to be prolonged: he certainly clung on to life with a tenacity that startled my sister and me. We will never know, though, because we didn’t talk about any of it.
“It is our responsibility – all of our responsibility – to find the person behind the patient in the bed,” Davis says. “One way or another, we have to have those conversations.”
In the year since I first wrote about cliché-free memorial tattoos for Modern Loss, I’ve encountered people’s ink tributes in bathroom lines at concerts, at book readings and all over the Internet. I’ve heard about a wedding party who got a mass tattoo for a late groom and from a reader who inked the title of my memoir on her forearm to honor her late brother.
I confess that I’m still contemplating tattoo designs for my late husband and brother, but not for lack of exposure to meaningful, aesthetically stunning tributes. The memorial tattoos included below reach beyond rose-wrapped crosses and words like “R.I.P.,” and into the realm of the remarkably personal. Some take a high-design approach and some are unassumingly simple, but all use unexpected symbolism to honor the deceased.
Redford Reid
Name: Redford Reid Age: 34 Current City: Brooklyn, N.Y. Date of Loss: Feb. 8, 2014 Tattoo Artist: Thomas Hooper of Rock of Ages in Austin, Texas
Who does your tattoo memorialize? My father, Gary R. Parker.
How did you lose him? In a tragic skiing accident.
Did you get the tattoo on a significant date? No, the timing was based on the artist’s availability.
Tell us about the tattoo’s design: My dad often wore ties, so I chose several from his closet that had design potential for a tattoo. Then I asked the artist to create a mandala inspired by those ties.
Meghan Schuttler
Name: Meghan Schuttler Age: 25 Current City: Santa Rosa, Calif. Date of Loss: June 3, 2011 Tattoo Artist: Brandon Bartholomew of The Hole Thing in Santa Rosa, Calif.
Who does your tattoo memorialize? My father, Scott Schuttler.
How did you lose him? Sudden heart attack.
Did you get the tattoo on a significant date? Following my college graduation, and almost exactly one year after he passed.
Tell us about the tattoo’s design: My dad was a musician and loved music. The design is his first name, “Scott,” represented in musical symbols. The numbers indicate his birthday (June 5) and death day (June 3). I chose to place the tattoo on my left ribcage so it would be close to my heart.
Angela Lee Bellefeuille
Name: Angela Lee Bellefeuille Age: 35 Current City: Washington, D.C. Date of Loss: February 2, 2014 Tattoo Artist: Alessandro Contu of Tattoo House Perugia in Perugia, Italy
Who does your tattoo memorialize? My husband, Riccardo Romani.
How did you lose him? Metastatic brain tumors. He fought for 14 months and endured five brain surgeries before losing the battle.
Did you get the tattoo on a significant date? On March 31, 2014, after a bout of depression left me contemplating suicide.
Tell us about the tattoo’s design: In order to feel the pain of slitting my wrists — so I’d never do it — I decided to get a tattoo there. The act of tattooing represents curbing my desire to end my life (and the pain) after losing my husband. Literally, the three birds represent the three souls lost: his, mine, and our 19-year old cat who died two weeks before Riccardo did. But it also symbolizes the hope of flying away and finding a beautiful life after tragedy.
Who does your tattoo memorialize? My husband, Riccardo Romani.
How did you lose him? Metastatic brain tumors. He fought for 14 months and endured five brain surgeries before losing the battle.
Did you get the tattoo on a significant date? On March 31, 2014, after a bout of depression left me contemplating suicide.
Tell us about the tattoo’s design: In order to feel the pain of slitting my wrists — so I’d never do it — I decided to get a tattoo there. The act of tattooing represents curbing my desire to end my life (and the pain) after losing my husband. Literally, the three birds represent the three souls lost: his, mine, and our 19-year old cat who died two weeks before Riccardo did. But it also symbolizes the hope of flying away and finding a beautiful life after tragedy.
Katie Irish
Name: Katie Irish Age: 35 Current City: Brooklyn, N.Y. Date of Loss: Nov. 14, 2012 Tattoo Artist: Sue Jeiven of East River Tattoo in Brooklyn, N.Y.
Who does your tattoo memorialize? My daughter, Roxane Persephone Chinn.
How did you lose her? I was 40-weeks pregnant, and it was our due date. Late in the afternoon, I became aware that Roxy wasn’t moving as much as she normally did. I attributed it the fact that she was full term and had pretty much run out of room. We called the doctor, and she had us come in for an ultrasound. We arrived at the hospital, but they could not find a heartbeat. After I delivered her the next morning, we saw that there was a true knot in her umbilical cord that had probably formed very early in the pregnancy.
Did you get the tattoo on a significant date? It took time to decide that I wanted a tattoo (this is my only one) and once I did, to figure out what I wanted. After that all became clear to me, though, I wanted it as soon as I could get an appointment with Sue. The date itself wasn’t significant, but the act definitely was.
Tell us about the tattoo’s design: Once I decided that I wanted to commemorate Roxy in this way, I began researching ideas. I knew that I wanted something beautiful that wasn’t immediately recognizable as a memorial tattoo. I began looking at Victorian mourning jewelry (no one has done mourning like the Victorians) and found a beautiful brooch with an outstretched hand holding some foliage. This symbolizes remembrance. I changed the foliage to Cyprus branches, which is what we had carried at Roxy’s memorial. When I met with Sue, she was thrilled by the idea of using Victorian mourning symbols for this and suggested the addition of the hair jewelry piece at the bottom. The Victorians would cut the hair of their dead and weave it into incredibly intricate pieces: bracelets, brooches, rings, and even tiaras. We decided on a bracelet that attaches to the cuff of the hand and disappears into the Cyprus. This is another symbol for remembrance but it also reminds me that Roxy was born with a full head of beautiful, dark hair.
Rita Schell
Name: Rita Schell
Age: 50
Current City: Colorado Springs, Colo.
Date of Loss: Nov. 18, 2011 Tattoo Artist: Ron Dolocek of Lucky Devil Tattoo in Colorado Springs, Colo.
Who does your tattoo memorialize? My only brother, Johnny Schell.
How did you lose him? Suicide.
Did you get the tattoo on a significant date? I chose the month of February since that’s the beginning of our astrological sign’s timeline.
Tell us about the tattoo’s design: My brother and I had a bond that allowed us to communicate with a look and through humor that only we understood. When I lost him, I was devastated and went through a period of drug and alcohol use. I couldn’t stop thinking about what I could have done to change things. I didn’t want to stop thinking about Johnny because I thought if I did, he would disappear and I’d have nothing. But after I read the book [by the author of this column] “Splitting the Difference,” I realized that keeping my brother’s memory alive didn’t mean living my life for him and it didn’t need to come at the expense of my health. I could still love him, miss him and talk to him without destroying myself in the process. So the tattoo’s phrase refers to my choice to “split the difference” between losing him and losing myself. Johnny was a Pisces like I am, so I chose the two fish that symbolize our astrological sign. He was born on St. Patrick’s Day so the fish representing him is green; my fish is purple because my February birthstone is amethyst. The color of my fish also ties back to a pair of amethyst earrings that Johnny gave me when I was a little girl and he was a cadet at the U.S. Military Academy at West Point.
Jesika Doty
Name: Jesika Doty Age: 40 Current City: Kansas City, Mo. Date of Loss: Sept. 20, 2009 Tattoo Artist: Chris Orr of Mercy Seat Tattoo in Kansas City, Mo.
Who does your tattoo memorialize? My husband, Doug Doty.
How did you lose him? Helicopter crash.
Did you get the tattoo on a significant date? It was close to what would have been our seventh wedding anniversary.
Tell us about the tattoo’s design: On our wedding day, Oct. 1, 2005, my soon-to-be-husband gave me this handwritten card before we walked down the aisle together: ‘You are the love of my soul, and the soul of my life. I love you, Always, Douglas.’ He had a way of capturing the feelings that we experienced together, and these particular words from him remind me of the undying connection we have and the beautiful love we shared. It reminds me that a connection like that is real, can be real again and not to settle for anything less. It’s a daily message in his handwriting about the possibilities of love…a permanent love note directly from him.
Homeless in his last days, Joerg Brylla did not leave assets to pay for a lavish funeral and eternal place of rest.
But, today, Mr. Brylla’s ashes are behind a brass plate labelled with his name and lifespan – 1945-2014 – in a brick wall at a North Vancouver cemetery. There’s a forest setting and a nearby pond. The cost to inter Mr. Brylla, who died of natural causes in a protest camp over affordable housing in Vancouver’s Downtown Eastside, was covered by the B.C. government as a part of a program that addresses the fate of the homeless when they die.
The Vancouver funeral home that handles many government-funded funerals happened to have space in the North Vancouver cemetery where it sent the remains of 69-year-old Mr. Brylla, also known as Bunny George – the focus of a recent Globe and Mail investigation into his eventful life and tragic death.
The situation reflects the reality of attending to the remains of the homeless in British Columbia – not only funeral costs, but also the rites and traditions of gathering to pay tribute to people who die without addresses, and often without salient facts of their lives being known.
In Mr. Brylla’s case, the North Vancouver cemetery fit within the budget set by the Ministry of Social Development, said Corey Dixon, assistant manager of the Glenhaven Memorial Chapel on East Hastings. Mr. Dixon said he did not have a specific cost figure at hand. He said Glenhaven handles 270 to 300 such funerals each year.
The social-development ministry said it spent $3.2-million in the last fiscal year on 2,000 services as part of its funeral supplement program, which can involve the deaths of homeless people, as well as others lacking funds to cover costs.
In a written response to questions from The Globe, Charlotte Poncelet, the executive director of the British Columbia Funeral Association, said funding has not increased since 2008, so its members “frequently financially subsidize these services because they believe that a person’s financial means does not diminish the significance of their life.”
Many people buried under the program are sent to the Surrey Centre Cemetery, which is more affordable than elsewhere in the Vancouver region, although families can make their own recommendations. Outside the Lower Mainland, people are buried wherever space is available.
At the Surrey cemetery, labourer Matthew Scozzafava said there is no paperwork to designate the homeless over others being interred. Sometimes, he and his crew are the only people on hand to bid farewell to the deceased.
“The only time we would know if they are homeless or not is if a loved one or a friend of the family or their friends have shown up and they tell us that sort of thing,” he said. He recalls one occasion where about 40 people from the Downtown Eastside came out to the service by vans and buses – “however they needed to get out here.” Sometimes, family of the homeless turn up after the fact.
But the final rest is only a prelude to tribute and commemoration, which is handled differently by various agencies. No one has ever died at Insite, the safe-injection site in the Downtown Eastside, but memorials for those who die homeless are especially important to the neighbourhood, said spokesperson Darwin Fisher. There are no newspaper obituaries for such individuals, Mr. Fisher said in an e-mail exchange. “But their life and the love and loss felt by the community needs to be acknowledged.”
At Insite, memorials are held in a nearby community garden or a coffee lounge on site. They can feature singing, drumming, speeches or a simple prayer with informal stories. Often, there’s a memorial poster with a photo of the deceased.
“I was so shocked when I overheard a person say, ‘I can’t wait to die so I can get a poster like that …’ It’s so sad that the person who uttered that felt so little loving acknowledgement in their life,” Mr. Dixon wrote.
Pastor Bob Swann of the First Baptist Church in downtown Vancouver, who presided over Mr. Brylla’s memorial service, said he does about one such tribute a year.
“Every story is quite unique,” Mr. Swann said, adding there is a service whenever word comes in that someone associated with his church’s shelter program has died – in dumpsters and elsewhere on the unforgiving streets, without addresses.
“The memorial service is more about those who remain, to teach them that, ‘Yes. This person has passed away, but they did, this, this and this,’ and they meant something to us and were part of our community.”
He said death equalizes the homeless with those who are better off. “We all leave here with nothing,” he said.
How much do you think it costs to cremate a dead body? It’s a question you probably don’t think about until tragedy strikes and you’re planning the funeral of a loved one.
One of the last things anyone wants to do when they’ve lost a loved one is make a complicated financial decision. Families want to spend that time celebrating a life, not hunting for the best rate on the memorial service. If a funeral home quotes you a price for a cremation, you’ll probably just assume you’re being treated fairly and accept the price.
So it may come as a surprise that the price of basic services like cremation can vary wildly from home to home. Today the average cost of a standalone cremation — no additional services — is $2,057. And yet, in any given city, some funeral homes will charge you two to three times as much for a cremation. Same service, drastically different price.
Even more troubling, in the Internet age funeral parlors tend to make pricing hard to find. In fact, the Federal Trade Commission allows funeral homes to keep their rates hidden until someone actually writes or calls a funeral home representative — leaning on regulations last updated in 1994 — rather than pushing funeral homes to let the customer compare online. In a survey by the nonprofit Funeral Consumers Alliance, only 25 percent of funeral homes fully disclosed prices on their websites, while 16 percent failed to disclose prices after an email and a phone call.
Tough access to comparison shopping seems to affect pricing. At Parting, we’ve painstakingly built a database of how much funeral homes charge for services so that no one ever gets ripped off in their time of need. Let’s walk through the data.
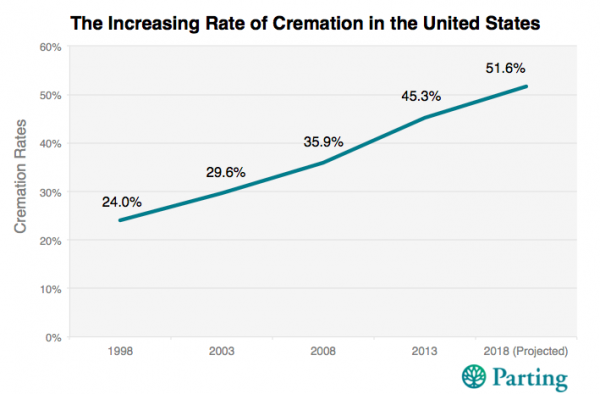
If recent trends continue, cremations will account for over half of all funerals by 2018, up from about a quarter in 1998.
People have been buried in coffins for centuries, so why the rise in cremations?
The Cremation Association took a look at this question. The group found a correlation between high cremation rates in states with a high proportion of people unaffiliated with organized religions, and the number of unaffiliated individuals is on the rise. The group also attributes the growing cremation rate to the simple fact that it’s cheaper than the coffin, which alone can cost thousands of dollars. And having the ashes portable in an urn (which typically cost in the hundreds of dollars) allows families more creative memorial ceremonies, like at a riverside or on a mountain top, where they don’t pay for a burial plot.
The cremation process itself is relatively straightforward. The body is placed in a large chamber and using mid-thousand-degree heat from oil, gas or propane, the body is incinerated. The process may have minor differences, depending the funeral home, but the end product is the same: ashes, in an urn or container.
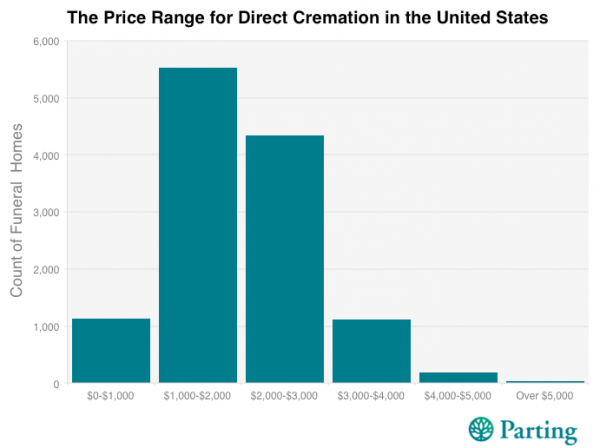
Though families get essentially the same product regardless of where the body is cremated, there is surprising variation in cremation costs. Analyzing our data, we found that while there are many locations at which direct cremation, the most basic cremation service, costs less $1,000, there are are also a large number of funeral homes which offer the service for more than $4,000. There are even those that charge over $9,000 for the service.
Comparing direct cremation costs is not always apples to apples. For instance, some funeral homes have their own crematorium while others use a third party, which can mean an extra fee. Still, these fees don’t explain why direct cremation at some facilities costs five times more than others.
John Jung of California Mortuary in Los Angeles points out that cremations are an administratively intensive process. They have to get approval from a doctor and, depending on the state, the various layers of government.
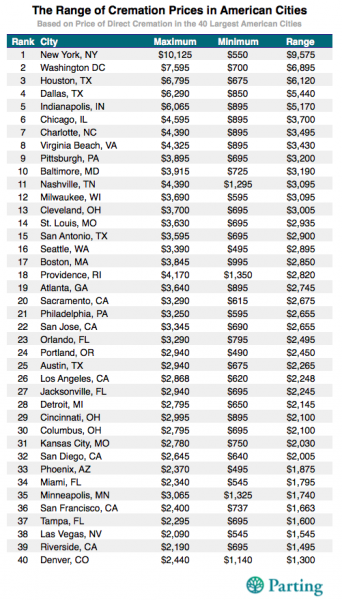
But when we analyzed cremation costs by city, we also found large variations in price within the same location. The following charts shows the range in prices for the forty largest U.S. cities in order of the largest range in price.
The disparity in some cities is glaring. New York tops the list with the highest parlor charging over 18 times the lowest. In Washington DC, the most expensive direct cremation is nearly $7,000 dollars more than the least expensive.
How could there be such a wide range of prices?
Jung believes that any parlor on the very high end of pricing probably doesn’t see the service as essential to their business. They keep cremations on the price list in case someone really wants it and then they turn a hefty profit for the effort. But it’s not core to their revenue.
And the lower range cremation prices are likely to attract additional business. They are loss leaders. “If it’s under $1000, they’re probably losing money. You really don’t make much profit on the direct cremation alone,” Jung says. “They’re just trying to get you into the door.”
The average price for a standalone cremation nation-wide is $2,057 but our data shows a full memorial service costs, on average, $3,650. These bundled services add additional products like the cremation casket, which typically go for around a thousand dollars or just removing and transferring the remains (typically a few hundred), not to mention flowers, embalming services and time spent viewing the body.
Getting a family in the door allows a funeral director to sell these additional services. This can create an awkward situation: It’s hard to say no to an upsell for someone’s last goodbye. Good funeral homes try to keep that balance of selling their own services while respecting the family in a time of need.
“It’s really a service industry,” Jung says of funeral homes. “You have a job to do but at the same time you have to direct them in a gentle manner.”
Not every state is equally shocking in the divergence of cremation prices. California offers some hope that transparency would alleviate such glaring disparities. The state requires that if a funeral parlor has a website, it must post prices.
“California funeral law protects the family a lot,” says Jung, whose family has run their parlor in the Los Angeles area for 17 years. “It’s pretty strict.”
Unfortunately the “death-care” industry, as Bloomberg noted in a 2013 cover story is big business and often ends up preying on grieving families. Publically traded funeral home companies like Service Corporation International (SCI), which run thousands of funeral homes across the country, are worth over $5 billion and — unlike locally-owned homes integrated with a community — answer to Wall Street traders, leading to pressure to upsell consumers.
Cremations are taking the place of casket burials and future generations will expect their prices online for a straightforward albeit serious service. More transparency will go a long way and having cremation costs online puts power into the consumer’s hands when they need it most.
No one wants to shop around for the best prices for a cremation when dealing with a tragic death, and unfortunately some funeral homes take advantage of this fact.
People have smuggled lethal drugs into hospitals so their loved ones can die, Philip Nitschke says.
Three people smuggled lethal drugs into Australian hospitals last year so their loved ones could secretly take their own lives when nobody was watching, euthanasia campaigner Philip Nitschke claims.
The head of Exit International said all three patients were elderly people with serious illnesses when they took a lethal drug in their hospital beds. They were being cared for at the Royal Prince Alfred and Concord hospitals in Sydney and the Austin hospital in Melbourne.
In each case, a partner or adult child took the lethal drug to them in hospital, Mr Nitschke said. The patients had previously acquired the drug in case they wanted to take their own lives one day.
Mr Nitschke, a former medical practitioner, said the three people took their drug overnight while no hospital staff were watching. The next morning, their deaths were recorded with no suspicion about how they died.
“In each one of those three cases, there have been no questions asked. It’s not surprising because they were very sick. The assumption was that they just died,” he said.
The cases are now being used by Mr Nitschke in his workshops on assisted death. He said while many people fear they will not be able to take their own lives in hospitals or other institutions such as nursing homes, these recent stories show it can be done.
However, he warned that if the relatives were caught smuggling a lethal drug into a hospital, they could be charged with criminal offences including assisting a suicide.
Philip Nitschke
Mr Nitschke recently tore up his medical licence after the Medical Board of Australia demanded he stop discussing suicide if he wanted to keep his medical registration. He has since continued his work with Exit International.
Dr Rodney Syme, of Dying with Dignity Victoria, said he had never heard of families assisting people to die in hospitals in such a fashion. However, he said the reports added to the case for assisted dying laws in Australia. If there were more options for people to end their lives when the time was right for them, he said clandestine suicides in hospitals would not happen.
Margaret Tighe, of Right to Life Australia, said it was appalling that Mr Nitschke was promoting these deaths. She said the hospitals should investigate them and boost their security.
While spokespeople for the hospitals said they did not know anything about the deaths, a spokesman for NSW Health Minister Jillian Skinner said: “Any matter of this nature should be referred to the appropriate agency, the police, and accompanied by details and evidence of the illegal activity.”
A spokesperson for federal Health Minister Sussan Ley said she was “disturbed by any serious breach of accepted or ethical medical standards and this certainly falls into that category”.
“Obviously our department will need to obtain more information from the relevant health offices in both states before we could comment in any detail,” her spokesperson said.
A spokeswoman for Victorian Health Minister Jill Hennessy would not comment on the reported deaths, but said the Victorian government was introducing laws this year to give people more choice about the kind of medical care they want or do not want in the event of future illnesses such as cancer or dementia.
The Australian Medical Association would not comment on the report, but Secretary of the Australian Nursing and Midwifery Federation, Lee Thomas, said: “It is unfortunate that any person needs to resort to drastic measures to relieve their pain.”
“Overwhelmingly ANMF members support the right to die with dignity and many have been engaged in the dying with dignity movement,” her statement said.















{kind=link}