How did an act of cannibalism transform into a national day for honoring the dead?
As the legend goes, during China’s Spring and Autumn Period following a civil war, Prince Chong Er was forced into exile for 19-years. With him was his loyal minister, Jie. When the pair had run out of food and were starving, Jie cut the flesh from his own leg and made a leg soup from it to feed the Prince, taking loyalty to a whole new level.
When the hard times were over and the Prince became King, he rewarded all those who had remained loyal to him and totally overlooked the guy who CUT THE FLESH OFF HIS OWN LEG TO FEED HIM. Jie packed up his bags and disappeared into the wilderness, taking his mom with him.
Someone finally confronted the King about his major oversight and feeling ashamed, he went off in search of Jie, but never found him. In result, some idiot suggested setting the entire wilderness on fire to smoke him and his moms out so, that’s just what the king does. Surprise! Still no Jie.
When the fire was extinguished poor, loyal Jie is found dead in the forest , underneath a willow tree, with his mother on his back. Inside the tree is a letter, written in blood from Jie, “Giving meat and heart to my lord, hoping my lord will always be upright. An invisible ghost under a willow tree is better than a loyal minister beside my lord.” Ouch…
In honor of Jie’s death, the King decreed that no fires could be lit on this day and created the Hanshi Festival or “Cold Food Festival,” since food could not be cooked.
Throughout China’s history the Cold Food Festival has been absorbed into the Tomb Sweeping Festival, which occurs on April 4 or 5th each year.
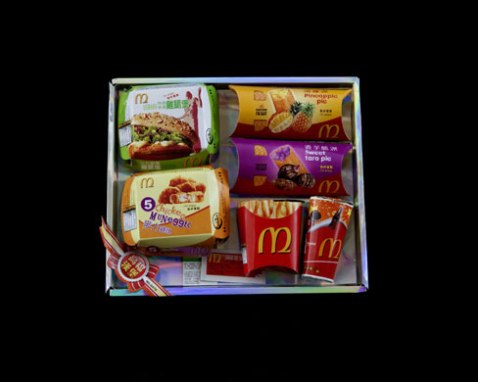
Quingming or Tomb Sweeping Day in China is a day for honoring the dead. The day is reserved for visiting the graves of loved ones. At this time the graves are cleaned and tended to, favorite foods of the deceased are offered and the practice of burning paper goods, “joss paper,” in the form of money and luxury items is practiced. Joss paper has taken many forms in recent years, everything from McDonalds food to IPhones to the more traditional money, ensuring that the deceased is well provided for in the afterlife. It is reassuring to know there is no McDonalds in the afterlife, tho, amirite?
Since the tradition of eating cold food remains a large part of the festival, qing tuan, sweet green rice balls, have been a traditional festival food for some 2,000 years. A “green rice” dish is also common, containing a mixture of rice powder and green mugworts, stuffed with a sweet bean paste. Both dishes are common offerings to the dead.
Modern elements now include the recent crop of websites where busy families and professionals who cannot travel to the gravesite can choose from different “tomb sweeping packages.” Professional mourners will go to your loved ones grave, clean and provide traditional offerings. Sobbing or weeping is extra.
He crossed the marbled lobby of his building, headed for the front door, leaning into his blue walker as if he were facing a gale-force wind. A golden starburst of drying urine ringed the front of his khaki pants. I thought we were meeting in his apartment, but one of us had the time wrong.
As a hospice volunteer for his late wife, I had traveled from my home in Brooklyn to the Upper West Side every Sunday for the last four years to spend time with them, adding more visits when they needed help with household tasks. When she died, I could hardly abandon him. We had, over the course of all our time together, become a kind of family.
Widowers are endangered beings, challenged by grief and its grim companions: loneliness, disorientation and a statistically high mortality rate. A 2012 study by a team at Rochester Institute of Technology showed that widowers are 30 percent more likely to die after the recent death of a spouse, compared to normal risks of mortality. The first six months after widowhood are the most challenging, but the effects of grief can last up to a decade.
At 90, the man I come to visit every week has a host of complicating ailments: He lives with a colostomy bag; his feet are permanently swollen and flaky with gout; he was given a diagnosis of prostate cancer more than a decade ago. It’s a slow growing cancer, and while he had treatment for it, he suspects that some of his current urination problems are a result. These health factors would be challenging enough on their own, but now they are compounded by profound grief.
It had been only eight weeks since he and I had watched his wife take her last breath on the sofa in their apartment upstairs. Her companionship — they had been married for 53 years — had long dictated his daily schedule; for years her illness required him to carry on with the duties of the household. With his wife gone, his routine gave way to a morass of unaccountability and unwelcome quiet.
It would be easy to be rebuffed by his stoical insistence that he’s fine, but his family and I have begun to track his emotional and physical wellness in a number of ways in the hope that we can forestall the typical effects of new widowhood. Which is why, as he and I stood in the lobby, I anxiously checked the time on my watch, vigilant for any indication that he was encountering psychological or physical difficulties.
He seemed a little confused about what day it was. Yet his thin white hair was neat; his sneakered steps deliberate and sure. His eyesight has been quickly fading over the past few years, but he continues to watch TV, and he is in charge of his hygiene and his schedule for all but four hours a day when his aide comes to cook his evening meal. Despite his soiled clothes, he seemed to be managing his activities of daily living (what gerontologists call A.D.L.s) successfully.
Social isolation is a risk many widowers face, compounded by solitary living. A Pew Research study reported in February showed that an increased number of men live alone: 18 percent, up from 15 percent in 1990. According to AARP, 90 percent of those over 65 wish to stay at home as long as possible.
Although his daughters call and visit frequently, they both live far away. Most of his friends are long dead and he is not a member of a synagogue or senior center, organizations that can often provide continuity and support to elder widowers. My weekly visits, and those of his niece and others, are important to ensure that he socializes.
Mobility can also be an inhibiting factor to maintaining social ties and physical health. Although he is still able to take the bus to doctors’ appointments across town, he tires easily. Some taxis can’t accommodate his walker, and his swollen feet and fading eyesight put him at risk for falling. The National Council on Aging notes that falls are the leading cause of fatal and nonfatal hospital admissions among the elderly. A misplaced step could lead to depression, feelings of helplessness and increased isolation during recovery. Still, it’s important to him that he remain independent as long as possible, which means he’s learning to balance mobility with safety.
Unlike many of his peers, my friend owns his home and has adequate finances to last until the end of his life, even if he increases the visiting hours of his home health aide. But in New York City alone, 20 percent of those over 65 live below the poverty line. Because the federal poverty rate is so low — $11,770 a year for a single person — many elderly people don’t qualify for the benefits they need, particularly in urban areas where housing and insurance rates can be higher.
According to a recent study by the University of California, Los Angeles’s Center for Health Policy Research, an increased number of senior citizens in California are experiencing “worse health, more depression and less access to care.” Because widowhood can decrease household income and other resources, those who have recently lost a spouse are particularly susceptible to this trend.
He will turn 91 this month. His older daughter is coming up from Virginia to host a party in his honor. I’ll pick up a cake, ordered by his younger daughter in Colorado, from his favorite bakery on the Upper East Side. We’ll drink champagne to toast his health, and we’ll miss his wife on this first birthday without her.
Marking family and personal occasions in this way has become increasingly important to all of us; these events intersect long, quiet weeks with laughter and company. And here’s the often unacknowledged benefit to keeping watch on a widower: With my grandparents dead and my friends all around my age, he diversifies my social life as much as I do his. He gives me a perspective on the city we live in that my peers simply don’t have. We spend our time together talking about our dissimilar lives and the things that matter to us, reminiscing about his many rich years, and looking up old poems in the vast library that lines the walls of his house. He is my friend and I miss him when I am away. As it turns out, nonagenarians are good company.
A trawl of data in Denmark reveals that recently bereaved people have an elevated risk of heart trouble
Agence France Presse
The risk of an irregular heartbeat was 41% higher among those who had been bereaved, according to the study
The death of a life partner may trigger an irregular heartbeat, itself potentially life-threatening, according to research into the risk of dying from a broken heart.
A trawl of data on nearly one million Danish people showed an elevated risk, lasting about a year, of developing a heart flutter. Those under 60 whose partners died unexpectedly were most in peril.
“One year after the loss, the risk was almost the same as in the non-bereaved population.”
Much research has focused on explaining the observed phenomenon of people dying soon after their life partner.
Several studies have shown that grieving spouses have a higher risk of dying, particularly of heart disease and stroke, but the mechanism is unclear.
The latest study asked specifically whether bereaved partners were more likely than others to develop atrial fibrillation, the most common type of irregular heartbeat and a risk factor for stroke and heart failure.
Researchers in Denmark used population data collected between 1995 and 2014 to search for a pattern.
Of the group, 88,612 people had been newly diagnosed with atrial fibrillation (AF) and 886,120 were healthy.
“(T)he risk of developing an irregular heartbeat for the first time was 41% higher among those who had been bereaved than it was among those who had not experienced such a loss,” said the study led by Simon Graff of Aarhus University.
Younger people, those under 60, were more than twice as likely to develop problems, and those whose partners were relatively healthy in the month before death, thus not expected to die, were 57% more at risk.
The team cautioned that no conclusions can be drawn about cause and effect, as the study was merely an observational one, looking at correlations in data.
Several factors that could throw the findings out of whack, such as the bereaved group’s diet, exercise regime, or predisposal to AF, were not known.
The loss of a partner is considered one of the most stressful life events.
It can lead to mental illness symptoms such as depression, and can cause people to lose sleep and appetite, drink too much and stop exercising – all known health risks.
Rare insight into attitudes to death among the very old
UNIVERSITY OF CAMBRIDGE
Death is a part of life for people over 95 years old, who mainly live day-to-day, concludes a rare study of attitudes to death and dying amongst the very old. The research, from the University of Cambridge and published today in the journal PLOS ONE, finds that this group is willing to discuss dying and their end-of-life care, but is seldom asked.
Improvements in our environment and lifestyles, as well as significant medical and healthcare advances, mean that more and more people are living to a very old age. According to a report published last year by the Office of National Statistics, the number of people aged 90 or more at the time of their death has tripled in the past three decades in the UK.
“Despite the dramatic rise in the number of people living into very old age, there is far too little discussion about what the ‘oldest old’ feel about the end of their lives,” says Dr Jane Fleming from the Department of Public Health and Primary Care at the University of Cambridge, who led the study. “We know very little, too, about the difficult decisions concerning their end of life care.”
In a study part-funded by the National Institute for Health Research, researchers interviewed 33 people over 95 years old from the Cambridge City over-75s Cohort and for 30 of these and for 9 people too frail to be interviewed in person, a ‘proxy’ – a relative or member of care-home staff, for example – about attitudes towards death, dying and end-of-life care. The responses are at times poignant and occasionally humorous, but provide a fascinating perspective on the views of an often overlooked minority.
The age of the older people was so great that most of their contemporaries had died, so death was a regular feature of life and many spoke of living on borrowed time. “As people get older, as their friends die, there’s an element of ticking them off,” said one proxy.
Many of the older people referred to “taking each day as it comes”, expressing thankfulness for where they were in life and content, at this stage, to take life one day at a time, not worrying too much about tomorrow. There was a sense of life ticking along until something drastic happened. “It is only day-from-day when you get to ninety-seven,” said one.
Although one interviewee described only being “three-quarters of the way” through their life, others knew and accepted that they were going to die soon. One son-in-law describes his elderly mother-in-law giving a long-life light bulb to her granddaughter, saying: “Something for you, it’s not worth me having”. Most of the interviewees felt ready to die. “I’m ready to go,” said one woman. “I just say I’m the lady-in-waiting, waiting to go.” Some felt they were a nuisance to others, while others were more desperate in their desire to reach the end, suggesting they had simply lived too long. “Please don’t let me live ’til I’m a hundred,” one woman said to her proxy.
Several proxies discussed conversations that they had had about euthanasia. A son described a vivid memory of accompanying his mother to visit one of her friends who had dementia: “She said ‘Gordon, if I ever get like that, for goodness sake put a…’, it was her words, not mine, ‘put a pillow over my head, will you?'”
Most were not afraid of dying, either reporting that it did not worry them or their proxies saying they had not expressed any worries or fears about it. For some this absence of fear was rooted in positive experiences of others’ dying: One interviewee said of her parents: “They were alive, then they were dead, but it all went off as usual. Nothing really dramatic or anything. Why should it be any different for me?”
Proxies reported that death was rarely talked about: “That generation, they didn’t actually discuss death much, I don’t think,” said one. A few, however, talked openly about death and the future – one proxy described a conversation: “She said, ‘I should think I’ll snuff it soon, don’t you?’ I said, ‘I don’t know, you tell me’ and she just laughs. I mean, she… You can laugh with her about it, you know.”
Discussion of funeral preferences was more common than talking about death, although the extent of discussions varied. Some had made their preferences clear and had made plans themselves and paid for their funerals in advance. Others noted the difficulties of discussing funerals – one proxy described a conversation with her mother: “I said, ‘Do you think you would want to be buried or cremated?’ And she said, ‘Well, cremated, I think.’ I find it very difficult talking to her. I don’t feel that I can. You see, I say to my children ‘Oh, that’s a nice song on the radio. Oh, perhaps I’ll have that at my funeral’. And you couldn’t to my mum.”
The manner of death was of more concern than its imminence. Although some said they had not really thought about dying, many explicitly expressed the wish to die peacefully, pain free and preferably while asleep – to “just slip away quietly.”
“I’d be quite happy if I went suddenly like that,” said one interviewee, snapping their fingers.
When asked whether, if they had a life-threatening illness, they would want to receive treatment that would save their life or prefer treatment that would just make them comfortable, few people chose life-saving treatment. “Make me comfortable” was a far more typical response and proxy informants tended to echo the older people’s dominant preference for comfort rather than life-saving treatment.
Few people wanted to be admitted to hospital in the event of such an illness, though rarely gave reasons. One care home manager explained about her resident: “If she went to [hospital] quite poorly, I think she would be full of anxiety and I think it would exacerbate any illness she had. I think she would find it alarming actually.”
Family members were often aware of preferences. One niece said of her aunt: “She’s dead against going. She doesn’t like hospitals. She doesn’t want to go.” Her aunt, she said just wanted to go to bed and go to sleep without going into hospital – “I think that’s her ideal, just dying in her own home.”
A handful of interviewees viewed well-intended medical interventions as prolonging life unnecessarily, an issue usually, but not exclusively, raised by proxy informants. One 98-year-old couldn’t “see any point in keeping people alive”. One proxy described being annoyed when the doctor gave her relative a pneumonia injection: “She had no quality of life… was ready to go … [but] there was no consultation with us at all about it.”
“Death is clearly a part of life for people who have lived to such an old age,” says Dr Fleming, “so the older people we interviewed were usually willing to discuss dying, a topic often avoided.” However, most had only had discussions regarding end-of-life preferences with health care professionals, rarely with family members. Nonetheless proxies tended to feel they knew their relative’s preferences, though the study found in a couple of instances relatives’ guesses were wrong. A care home manager commented that it was not necessarily with older people themselves that professionals broached the topic: “Historically what happens in hospitals is they tend to… if it’s not asked beforehand they go straight to the relatives. They won’t broach it with the individual, which is actually […] against the Data Protection Act, and it’s nobody else’s business. But it is how the culture of hospitals works unfortunately.”
However, the same care home manager pointed to the practical difficulties of having conversations about end-of-life care preferences: “I’ve not had long discussions, because of [her] hearing problem. It’s very difficult to write them down on paper. And she’s got to shout the answer back at you and you’ve got to re-clarify it.”
“In our previous research we found the majority of people who die in their 90s or 100s are dependent on others because of very high levels of disability and cognitive impairment by the last year of life,” explains Dr Fleming. “Over recent decades most people dying in very old age have moved into care in their final year or died in hospital. To plan services to best support rising numbers of people dying at increasingly older ages we need to understand their priorities as they near the end of life.”
“Now so many more people have reached a great age before they die, it’s important we know about their views and their concerns, particularly in relation to end-of-life care,” says Dr Morag Farquhar, the study’s other lead author. “These are difficult conversations to have and no one wants to have to face their own death or that of a loved one. But having these conversations before it is too late can help ensure that an individual’s wishes, rather than going unspoken, can be heard.”
I was connected to her in a very personal way. When we were preteens, my best friend (also my cousin), and I used to sit in front of the TV in our sponge curlers and Lanz nightgowns, fantasizing about what it would be like to be Patty, always getting into trouble (but having fun) in high school. We loved, too, Cathy, her identical perfectly behaved but boring cousin from Scotland (with that adorable accent). I was always Cathy.
This is what high school would be like, falling in love with our French teachers, switching places to fool teachers, Cathy getting a flu shot when they thought she was Patty. And that flip haircut! Kind of like us.
Then came the drugs and divorces, and bipolar disorder, and no more sweet Patty Lane. The fairy tale ended. For a long time, her life was in decline. Just like a lot of us.
Something broke inside when I heard of her death. I’ve had friends die — one, at 37 — but it’s getting closer and closer.
My husband has started collecting Social Security and now, Medicare.
You know somewhere, in the back of your head, that you will die someday. I, more than most, was exposed to it early, diagnosed twice with cancer.
I suppose it’s all coming home to me because my husband is facing surgery. Yes, it’s minor. But it suddenly got him talking about wills and annuities and trusts and who to call (we’ve always kept our finances separate but he’s afraid he’s going to die and wants to make sure my son and I are taken care of). I guess be grateful for small things!
And then I realized, he’s going to die. Maybe not before me, but he will. We just celebrated our 22nd anniversary (actually been together 33 years and I want credit for it all!), and we’ve had our problems through the years. But I suddenly realized I loved him. What will life be like without him? We’ve been together more than half my lifetime. I don’t know what I will do if he is no longer there.
OK, so I’ll get the TV back (no more Bill O’Reilly) and I won’t have to pick up his ski coat off the floor, where he throws it when he comes home. And I won’t have to listen to any more diatribes about how Bernie Sanders will drive us to taxation hell.
You know this day will eventually come. But it just all seems so soon now.
Research has shown that 52 percent of Americans over 65 will not have enough money to maintain their style of living when they retire — because we haven’t wanted to think about dying. We haven’t made plans, so afraid of our impending mortality. Didn’t we all think we’d live forever? We were the Baby Boomers, after all!
As I said, I had an early preview so maybe it’s easier for me. But I still see my husband as the tall, skinny tennis star walking off the court with his trophy (and if I’m honest, me, too, in my short shorts and halter top).
He’s still athletic but his hernia has turned him into an old man overnight. Because of the pain, he’s had a hard time walking (and forget about getting in and out of the car!). It hasn’t stopped him from working at the two dental clinics he helps out at in New York, or even from using the elliptical and stationary bike at home.
But he still walks very, very slowly and it’s like getting a taste of the future.
Hopefully, the surgery will reverse that. But there’s no getting around it. We’re getting old.
I’m hoping next week he’ll be back to complaining that the paper towels are running out and returning to his endless “Camp Larry” Sundays, where he exercises for four hours at a stretch.
But I’m starting to think it’s the beginning of the end. Or maybe, it’s just the end of the beginning.
After a Canadian drugmaker doubled the price for the most commonly prescribed aid-in-dying drug, Washington Death-with-Dignity advocates created a cheaper new medication to help terminally ill patients who choose to end their lives under the law.
Valeant Pharmaceuticals
By JoNel Aleccia
Washington state Death with Dignity advocates have found a way to thwart a drug company that abruptly doubled the price — to more than $3,000 — of the lethal medication some terminally ill patients use to end their lives.
They’ve come up with a new mix of medications that induces death for about $500, said Dr. Robert Wood, a longtime University of Washington HIV/AIDS researcher who now volunteers with End of Life Washington, an advocacy group.
“We thought we should concoct an alternative that would work as well,” Wood said. “It does work as well.”
Now doctors in Oregon have adopted the drug mix, too, as a way to ensure that cost doesn’t prevent terminally ill patients from making the choice they want under the state’s right-to-die law. And in California, where a similar law takes effect later this year, officials are considering it as well.
“We’ve always had the belief that no matter who you are, whether you’re rich or poor, you should have access to a lethal dose of medicine that does what you want: to end your life in a peaceful and dignified manner,” said George Eighmey, president of the board of the Death with Dignity National Center, based in Portland.
The issue arose last year, when Valeant Pharmaceuticals International of Quebec acquired the rights to Seconal, the trade name of secobarbital sodium, the most commonly prescribed drug for aid-in-dying patients. The firm quickly doubled the cost, from $1,500 to more than $3,000 — and up to $5,000. That’s on top of previous retail price increases for the nearly 90-year-old sedative that once sold for $150 for a lethal 10-gram dose.
The impact on patients considering using the drugs was immediate, said Beth Glennon, a client-support coordinator for End of Life Washington.
“People were horrified. They were daunted. They thought it was criminal,” she said. “The cost increase has been significant for some people. Some are on a very fixed income.”
Some patients were worried about burdening their families with the extra expense of the medication, she said.
Health insurance often doesn’t pay for aid-in-dying drugs and they are not covered under Medicare. In Washington, the drugs aren’t covered under the state Medicaid plan or by several Catholic health systems that prohibit doctor-aided death based on religious objections.
So Wood and other doctors in the state decided to seek an alternative to the high-priced drug sold by Valeant, which is among firms under fire by Congress for hiking prices on desperately needed drugs.
They turned to a compounding pharmacist, who doesn’t have access to the exact ingredients included in secobarbital. The result was a less-expensive mix of three medications: phenobarbital, chloral hydrate and morphine sulfate, all in powdered form to be mixed with water, alcohol, applesauce or juice.
Alternative’s side effects
Last year, 55 of the 155 Death with Dignity patients seen at End of Life Washington chose the cheaper dose, Wood said. They opted for it even though the new medication tastes worse, burns the mouth and may take longer to work than Seconal.
“Roughly a third decided they’d try the untried and more burning method,” Wood said.
The other lethal drugs are bitter, often requiring patients to take anti-nausea drugs before ingesting them, he added.
Washington doctors shared their discovery with colleagues in Oregon, which was also grappling with the secobarbital price increase, Eighmey said.
In 2015, 16 of the 132 people who died in Oregon under the state’s Death with Dignity Act provisions ingested the new mixture.
Washington doctors also have been talking with colleagues in California, which passed a right-to-die law last year, becoming the fifth state to legalize the practice, along with Oregon, Washington, Vermont and Montana.
News reports last month suggested that Valeant increased the price as a reaction to California’s law, a contention rejected by company officials.
The increase came in February 2015, a month after the idea was proposed, but the law wasn’t signed by Gov. Jerry Brown until October, the firm noted.
In addition, Valeant said that secobarbital should be used for short-term insomnia, epilepsy and preoperative anesthesia and is not intended for any other use.
“The suggestion that Valeant raised the price to take advantage of a law that had not yet passed, for a use for which the drug is not even indicated, defies common sense,” officials said in a statement.
Valeant officials, along with those from Turing Pharmaceuticals, faced scrutiny in Congress this year after federal lawmakers released excerpts from documents detailing how drugmakers hiked prices to wring more revenue from new medications, including lifesaving drugs.
“Many companies are lining their pockets at the expense of the most vulnerable families in our nation,” Rep. Elijah Cummings, D-Maryland, said in a statement after releasing documents from Valeant and Turing Pharmaceuticals before a hearing on rising drug prices.
Valeant bought two lifesaving heart drugs, Nitropress and Isuprel, then tripled the price for one and increased the other sixfold, The Associated Press reported.
Under Death with Dignity law provisions, it’s up to doctors to choose and prescribe the drugs used to end patients’ lives, Eighmey said. Seconal became the drug of choice when Oregon’s law took effect in 1997 because it was used in the Netherlands, which provided a model for the first U.S. effort.
The drug was a popular sedative widely misused in the 1960s and 1970s, when it was associated with accidental overdoses, Eighmey explained.
It went off-patent in the early 1990s and some generic versions became available. But the drug fell out of favor as other sleeping aids, including Ambien, grew more popular. Because of the drug’s dwindling market, there were no generic competitors when Valeant acquired it and increased the price. Valeant reported the firm has sold only 1,000 units of Seconal since acquiring the brand in February 2015.
New drug of choice?
In 2014, 176 terminally ill patients in Washington received prescriptions to help end their lives and 170 died, according to the state Health Department. Of those who took medication, about two-thirds used secobarbital. The Washington act, which went into effect in 2009, allows terminally ill patients with less than six months to live to request lethal medications from their doctors.
The remaining patients used pentobarbital, a sedative used in death-row executions that became hard to get after European drugmakers cut off the U.S. supply to protest the practice.
As of 2014, at least 725 adults with terminal illnesses had chosen to end their lives with a doctor-prescribed dose of lethal medication in Washington. State figures on Death with Dignity Act patients for 2015 will be released this summer, officials said.
With stored supplies of secobarbital dwindling and the price remaining high, Washington’s concoction may become the drug of choice for most aid-in-dying patients, Eighmey said.
Most patients who end their lives under Death with Dignity provisions are educated and financially comfortable, like Ethan Remmel, a Western Washington University psychology professor and father of two who took a lethal dose of sedatives in June 2011, a year after being diagnosed with terminal colon cancer. He was 41.
The cost of the drug wasn’t a problem for their family, said his partner, Grace Wang, an associate professor of environmental studies at WWU. But she worries that financial need and a lack of insurance coverage might mean other families won’t have the option.
And the idea that a drug company would deliberately hike the price on dying patients?