[C]all it the new game of Truth. Players go around the table answering questions in their little blue booklets, but these questions aren’t geared to get them talking about that one time they went skinny dipping in Maui. Instead, the questions aim to launch difficult conversations, ones that may be painful, ones they may have been avoiding for far too long.
“Who haven’t you talked to in more than six months that you would want to talk to before you died?”
“What music do you want to be listening to on your last day alive?”
“Which is more frightening to imagine: suffering the worst physical pain of your life or not getting a chance to say goodbye to your family?”
This game is called Hello, and its goal is to get people talking about end-of-life issues in a way that’s easy and non-threatening. The most revolutionary aspect of it—and it’s such a simple thing—is that everyone can and should play. (Newsflash, friends: we’re all gonna die.) So often when it come advance care planning conversations, we single out the person who is sick or elderly, and it can feel like an interrogation. That is, if we even get to the conversations at all. According to Nick Jehlen, the lead designer of the game, people are often too nervous or distraught to delve into these real, complex discussions, or they feel it’s never the right time. The talks, he says, “just don’t happen.”
Families, friends, organizations and healthcare teams have gotten together to play Hello, which is created by Common Practice, a company that promotes better conversations about living and dying well. Some of the questions were written by backers of the Kickstarter campaign for their original game, My Gift of Grace. The topics range from the logistical (“If you needed help going to the bathroom today, who is the first person you would ask to help you? Who would you never be able to ask?”) to the abstract (“What do you think happens to you after you leave this life?”). Each player gives out game chips—“thank you chips”— to other players as they feel moved to, which creates, as Jehlen describes, “an economy of gratitude” within the game.
Jehlen says,“It’s challenging, and sometimes people do cry, but what we’ve really done is create a set of structures that help people be supportive of each other. Almost every time I play with a new group, people share things they’ve never talked about before, and just as importantly, they feel good about it.” He adds, “It sounds crazy, but the game is fun.” Of people who play Hello, 75% go on to complete an advance care planning step within a few months.
Talking about our own mortality doesn’t just save others from guilt, trauma and expense down the road—these conversations can actually improve our quality of life. They help us to really narrow in on what matters to us here and now. Perhaps a game can help get the ball rolling.
[S]ooner or later, the end is coming — for all of us. But women in particular have been at the forefront of the “death positive” movement, which aims to strip away the mystery and fear around the end of life and help us each find our own “good death.”
Amber Carvaly is a mortician and service director at Undertaking LA, the funeral home she coruns with Caitlin Doughty. A women’s studies major whose life’s passion has been to work harder, better, smarter, and kinder as a human being, she soon found herself in the nonprofit industry, preparing meals and holding birthday parties for LA’s homeless. When she lost her job after the economy crashed in the late aughts, she made friends with a funeral director. “It seemed like it had similar characteristics to what I was doing at the Downtown Women’s Center,” Carvaly remembers of their talks about funeral work. She wanted to continue helping people and decided to go back to school, this time to study mortuary science. “I had been emailing Caitlin throughout this,” Carvaly says, “although we had never met.” Eventually, Doughty asked if Carvaly was interested in helping her start Undertaking LA and the rest, as they say, is death-positive history.
Amber Carvaly of Undertaking LA.
“It is not death that is important, but how we live our lives as we near it,” Carvaly explains. “How we view and treat the dead is a reflection of society and our values. What I want is to change our hearts and souls and the way we literally see and process the world around us. I think our very existence and survival as a species depends on it.” Carvaly’s next big plan is to offer house death calls, where families are given a person to guide them through washing and dressing the body. “In my experience,” Carvaly says, “families have not needed anything spiritual or extravagant. They just want someone to stand with them and help give them the confidence to use the strength they already have within themselves to start.”
Melissa Unfred with her sidekick, Kermit.
The Summer before Melissa Unfred‘s senior year of high school, a local funeral home was featured on the news. They were a family-owned business looking for assistance and, as a joke, her mom turned to her and suggested she get a job. A budding rebel, Unfred did just that. “I was fascinated by the science and art involved in funeral service and embalming,” Unfred says. “And led by such a strong woman, no less! Billie White Everett [the home’s owner and one of the first female directors in Texas] made a huge impression on me.”
These days, Unfred educates people about home funerals and green burial, which focuses on returning the body to the earth in its natural state by foregoing embalming and using biodegradable materials like wooden caskets. She partners with an Austin crematory that shares her core values and is one half of Texas’s first certified therapy dog team working in funeral care, along with her furry sidekick, Kermit the dog. Originally adopted to be a pet and emotional support source for Unfred, Kermit’s knack for interacting with others, particularly the grieving, quickly became apparent. Now, the two are inseparable during transfers to funeral homes after someone has died, at graveside ceremonies, and everywhere in between. Together, they’re on a mission to clear out the smoke and mirrors of the funeral service, helping families understand their options so they can make an informed decision on what they want for themselves and their loved ones.
One of Lane’s hairwork pieces.
Courtney Lane of Never Forgotten braids hair for a living. She’s following a tradition called “hairwork,” which was part of the extensive Victorian mourning process. “What really makes hair art and jewelry special is that it can contain the hair of your loved ones,” Lane says. Her clients might provide her with their own hair to make into a romantic gift or a snippet from their child’s first haircut. Lane also works with cancer patients who lose their hair during treatment. “A cancer survivor once explained to me that this was an artistic statement that helped her feel like she wasn’t losing her hair, but transforming it into something new and beautiful,” Lane says. Very often, of course, the hair she’s working with is that of a deceased family member; because hair doesn’t decompose, Lane explains, it’s a perfect relic with which to remember our dead.
In addition to custom work for clients, Lane also makes art out of antique Victorian hair and travels to give lectures and workshops on the misunderstood history behind hairwork and its elaborate techniques. The first time she showed her art at a convention, a man walked up to her table and asked, in what she calls a Disney villain voice, if she could make him “something truly evil” if he brought her the hair of his enemies. Since then, she has gotten so many similar requests that she added a section to the FAQ on her website. The answer is no.
The theme of education runs throughout the work of Lane, Carvaly, and Unfred. For while death is ubiquitous, it is also misunderstood and maligned. “I do completely believe that humans should not be afraid of dead bodies,” Carvaly says. “By leading by example, I can show others that there is another way to approach our existence and demise. And that if I can do it, so can they.”
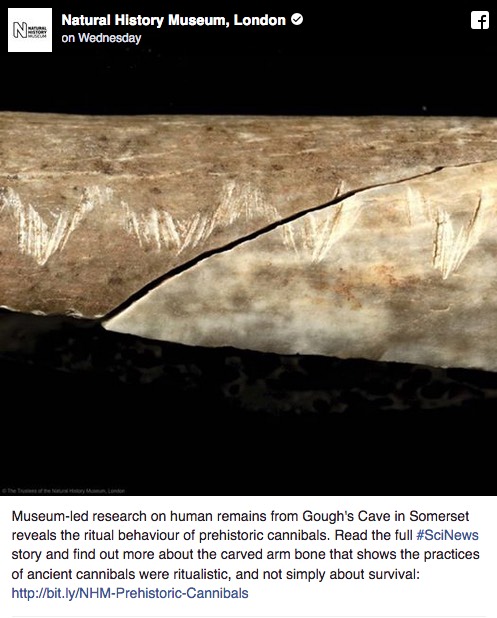
Prehistoric cannibals who once lived in a Somerset cave engraved human bones with zig-zag designs as part of a “complex” eating ritual, according to new research.
The bones, which had a number of deliberate cuts and human teeth marks, were discovered at Gough’s Cave in the Mendip Hills and are believed to be between 12,000 and 17,000 years old – when the cave was occupied by Ice Age Britons.
Researchers ruled out an initial theory that the marks were made during the butchery process, because they were found on a part of the bone with no muscle attachments. There is no indication on the skeletons that the humans had suffered violence before they died.
They concluded that the “zig zagging incisions are undoubtedly engraving marks, produced with no utilitarian purpose but purely for artistic or symbolic representation.”
The study, published in the journal PLOS ONE, says the marks may have represented the “story” of the victim’s life or a memorial to how they died. Whatever the reason, researchers agree it must have been part of a ritual or ceremony to mark the person’s passing, like modern day funerary rites.
“The sequence of modifications performed on this bone suggests that the engraving was a purposeful component of the cannibalistic practice, rich in symbolic connotations,” says Dr Silvia Bello, lead author of the study.
“Archaeologists have linked the engraving of objects and tools to ways of remembering events, places or circumstances, a sort of ‘written memory’ and ‘symbolic glue’ that held together complex social groups.
“Perhaps the engraving of this bone may have told a sort of story, more related to the deceased than the surrounding landscape. It could be that they are indicative of the individual, events from their life, the way they died, or the cannibalistic ritual itself.”
Gough’s Cave was first discovered in the 1880s and frequent excavations at the site found evidence that humans lived there for thousands of years, including “Cheddar man,” Britain’s oldest complete human skeleton, which dates from 7,150BC.
DNA taken from the skeleton was found to match that of Adrian Targett, a man living in the local area today.
The cave is 115 meters (377ft) deep and 3.405km (2.12 miles) long, and contains a variety of large chambers and rock formations.
Human bones have been found intermingled with butchered large mammal remains as well as flint, bone, antler and ivory artefacts, including a 13,000-year-old carving of a woolly mammoth.
The team has previously found skulls at the site which had been turned into bowls or cups, possibly to eat or drink from.
There are two things that movies consistently get wrong: sex and death. Unfortunately, as a society, we spend far too much thinking of sex, and too little time devoted to death – especially of a parent.
Caring for a dying parent is a difficult and emotionally challenging task. However, effective communication can ease the transition.
Movies consistently present death in a false or unrealistic way. Real-life death is not always dignified, simple or tidy. Indeed, death can be upsetting, messy, painful and traumatic experience for all parties involved.
Complications can arise during the course of an illness can lead to increasingly worsening circumstances. Immobile or semi-mobile patients may feel determined to walk and my try to get out of bed. As a result, some may fracture or break their hip. As bad as terminal illness is, additional complications can make quality of life worse. Patients may become restricted to their bed and may rely on a catheter.
Regardless of the attempts to prevent it, as soon as they return home, complications such as a yeast infection or urinary tract infection may occur. This causes a patient to become even more frightened and restless. How is anyone supposed to take care of a dying person? It’s a fairly straightforward to concept “nurse” a person back into good health, but how is anyone supposed to “nurse” them into death with dignity and compassion?
Then there’s the morphine. Dying parents may often feel agitated and restless, so much so that they might try getting out of her bed. The morphine may help to calm them down. Is it unethical to give it to them to address mental rather than physical pain? Although her hip fracture causes pain. Many children give their parents morphine more for their parents restlessness.
The only organ donors you see on “Grey’s Anatomy” are car accident fatalities. No one ever talks about mulling over whether or not to give someone’s organs away while they’re still conscious in another room.
These are the kinds of issues that children with dying parents struggle with every day. Many adult-children caregivers believe that their ill parent wouldn’t have wanted to live this kind of existence. They may have stated that they didn’t want a lingering, drawn-out death. This is why advance directives are so essential.
If you’re like most families (including mine), generally, the care of a dying parent falls on the shoulders (and back) of one sibling or family member. Although it’s rare for siblings to share parent care equally, it’s a family responsibility. Not treating it as such “will haunt you” later on. Even if you live far away from your ailing parent, you can still help out.
From ordering car service a couple times a week to paying bills online, anything that can be done via telephone or internet is within your reach, she notes. Just calling your mom more often “so she’s not so needy” can provide relief to the sibling carrying the heaviest load, says Russo, as can making the trip to be with your mom whenever possible, so your sibling can take time off.
End-of-life care is something that few people like to think about, let alone discuss. Avoiding the subject until it’s unavoidable, however, can be a “huge mistake” with devastating consequences for the sibling relationship. Call a family meeting when your parents are still healthy.
Such a conversation might start this way: Remember aunt so-and-so, and how our cousins were still fighting when she was on the respirator and they wouldn’t let her die and how painful that was for everybody?
We don’t want that to happen in our family.
Mom, Dad, do you have a living will? Have you assigned somebody to be the healthcare proxy? Though they may attempt to deflect such questions: nudge further. If you were on a respirator or in really bad shape, would you want us to do everything possible, or would you just want to go quietly? Who should make that decision? We’ll all want to do what’s right, but we may have different feelings.
It’s time to start an honest and open discussion of what dying really means. How can we help someone we love to pass on? What do “extraordinary measures” mean to different people? To some, it may mean CPR. For others, it might mean giving any medications that can help. Furthermore, what constitutes a tolerable living standard? For instance, what happens when someone is bedridden or unable to control their bowels?
There are few things more difficult than saying goodbye to a dying parent. These questions are undoubtedly tough ones. In most cases, they’re mentioned far too late.
Hospice care is for the dying. It helps patients manage pain so they can focus on spending their remaining time with loved ones. But in recent years, nearly one in five patients have been discharged from hospice before they die, according to government reports.
A study published last month in the journal Health Affairs finds that hospices with the highest rate of so-called “live discharges” also have the highest profits. The lead author is Rachel Dolin, a David A. Winston fellow researching health policy. Her paper found an association between high live discharge rates and high profit margins, but it didn’t determine the cause.
“It’s important to continue to study this area to get a better sense as to whether profits are driving the decision to discharge patients from hospice, rather than patient preferences and needs,” says Dolin.
To qualify for hospice care, two doctors must certify that a patient is expected to live no more than six months. But patient James B. Nelson discovered that sometimes the doctors are wrong.
“It was decided that I was not dying fast enough,” he told Arizona Public Media in 2015. “And so, to put it most succinctly, I flunked the hospice program.”
Nelson died a few months after giving that interview, but his situation isn’t all that unusual.
Government reports show that the median rate of hospice patients discharged before death has climbed steadily since at least 2000, peaking in 2012 and 2013 at almost one patient in five, though more recently the percentage has declined somewhat. But the rate actually varies widely from one care organization to another. Some hospices discharge less than 2 percent of their patients prior to death, while others discharge more than 80 percent. Non-profits have lower rates of live discharge than for-profit hospices. Regionally, live discharge rates are highest in the South.
It’s important to understand, though, that when patients are discharged from hospice, they don’t necessarily go anywhere. Hospice agencies, whether they are independent or affiliated with an institution like a hospital, usually deliver services to patients in their homes.
Medicare pays the bills for the vast majority of patients receiving hospice care, at a cost to the government of at least $15 billion a year. Federal regulators have questioned whether high rates of live discharge mean that hospices are making money by admitting patients who aren’t actually dying.
But these decisions aren’t that clear cut, says Dr. Joe Rotella, chief medical officer for the American Academy of Hospice and Palliative Medicine. “We see more and more patients that have conditions like Alzheimer’s disease or Parkinson’s disease that don’t always follow a predictable course,” says Rotella.
Some who study aging are concerned that certain hospices are gaming the system. That’s a worry of Susan Enguidanos, an associate professor in the Leonard Davis School of Gerontology at the University of Southern California. For example, she says that some hospices may be trying to avoid paying for costly treatments by discharging patients temporarily when they need to go to the hospital.
“Individuals that are going in for these very brief health issues are coming out and then, they’re being readmitted to those [same] hospices,” says Enguidanos.
That’s not a good reason to discharge someone, says John Keyserling, senior vice president for communications and policy at the National Hospice and Palliative Care Organization, the trade association for hospice providers.
“Any association between profit margins and clinical decision making is inappropriate and not something that the hospice community supports,” Keyserling says.
That hospice community has nearly doubled in size since 2000. Susan Enguidanos says it’s also changed a lot.
“Hospice organizations started as grass root efforts and were largely non-profit for a long time,” she says. “Now we’ve had a huge increase in for-profit hospices.” There’s a concern, says Enguidanos, that by discharging patients early, some hospices may be “trying to avoid costs that they should be responsible for.”
Whatever the short-comings of some hospices may be, Keyserling says that his biggest worry is that people who could be helped by hospice aren’t taking advantage of it in time. He says about half of patients die within 17 days of being admitted. And that turns hospice into “crisis care” instead of the comfort care it’s intended to be.
In summer fellowship, students pursuing health careers learn directly from the terminally ill
Skidmore College student Elisa Smith of MA, left, Union College student Matt Liquori of CT, center, and Colgate College student Yohary Fabian of Colonie with a practice mannequin at the Joan Nicole Prince Home
[M]atthew Liquori is spending his summer with dying people, and he knows what you’re thinking.
“Friends and family, when they hear, the first thing they say is, ‘Wow, that’s so depressing,'” he said. “But it’s really not.”
Far from it, the 21-year-old insists.
As part of a summer fellowship run by Union College, the incoming senior is spending eight weeks volunteering at the Joan Nicole Prince Home, a home where people with three months or fewer to live come to die in peace.
His program director calls it a crash course in death and dying — that human condition that strikes fear into the hearts of many but that future doctors, nurses and social workers will have to face head-on eventually. So why not face it sooner rather than later?
That’s how Liquori, a pre-med major at Union, recently found himself cooking chicken gizzards for a dying man and having one of his best days ever.
Rememberance board at the Joan Nicole Prince Home on Thursday, July 27, 2017 in Scotia, N.Y. The home is dedicated to providing a safe, comfortable and caring residence for terminally ill patients in need of a home during their final days. Five local college students are spending their summers caring for the terminally ill as part of a relatively new fellowship program offered by Union and Skidmore colleges.
It was the man’s first day at the home, and the student volunteers wanted to know what he liked so they could go shopping and fill the cupboards with food he might eat. But the 51-year-old — a gaunt, depressed man on the losing end of a nearly three-year battle with rectal cancer — had no appetite and little success when he did try to eat.
“It’s a tough transition and I think he was overwhelmed and not really willing to open up to us,” Liquori recalled. “So eventually we were like, what’s your favorite food in the world? And he responded, ‘It’s this Greek gizzard soup my mom and grandmother used to make growing up that we’d always have before our big Easter feast.'”
When the students went out and came back with the ingredients for the soup, the man suddenly grew animated. He walked them through how to make his passed-down family recipe, took selfies with the students and called his mom to let her know what was happening. By the time it was ready, he was so excited he was shaking, Liquori recalled.
“It was an awesome welcome for him because right away he was like, ‘It’s gonna be OK here,'” he said. “And that was really cool. It’s days like that that aren’t depressing because you go home and you feel great, and you’re like, that was a great day.”
The Joan Nicole Prince Home is a unique operation. Only two people at a time are allowed to live at the house, a handsome little cape at the end of a quiet cul-de-sac in Scotia. That’s on purpose — any more and the home would have to be run like a medical facility, with all its rules, regulations, poking and prodding.
That’s exactly what its residents are trying to avoid, and what its founders had in mind when the home was built in 2006.
Living room at the Joan Nicole Prince Home on Thursday, July 27, 2017 in Scotia, N.Y. The home is dedicated to providing a safe, comfortable and caring residence for terminally ill patients in need of a home during their final days. Five local college students are spending their summers caring for the terminally ill as part of a relatively new fellowship program offered by Union and Skidmore colleges.
Residents know they’re dying. Their doctors know they’re dying. By the time they arrive at the home, they’ve usually tried all the treatments, cures, medication regimens and so forth. Their time is up and they know it, and they just want to die in peace.
That’s hard to do in the cold and sterile atmosphere of a hospital, or at home where a loved one may not have the mental, physical or financial wherewithal to keep them comfortable. At the Joan Nicole Prince Home and other comfort-care residences, hospice workers visit to administer medical care and volunteers handle everything else — the cooking, cleaning, bathing, help going to the bathroom, or getting in and out of bed.
The psychological relief it provided Liquori’s patient, who wished to remain anonymous due to privacy concerns, and his wife was enormous.
“I can finally relax, you know? And my wife can finally breathe,” he said Thursday, puffing a cigarette on the home’s back porch. “She doesn’t have to walk in and go did you take this medicine? Did you take that medicine? Did you take this? Do I need to change your bandages? Do I need to change your colostomy? All that stuff. We can actually be husband and wife instead of patient and caregiver.”
Volunteers are needed 24/7, and three years ago board member Carol Weisse realized she had the ideal pool of candidates: wannabe doctors, psychologists and social workers.
Weisse teaches behavioral neuroscience, death and dying, health psychology and other courses at Union College in Schenectady. Hoping to marry the home’s need for volunteers and her students’ need for hands-on experience and research, she applied for a grant and launched the Community Action, Research and Education (CARE) Summer Fellowship Program, open to students from six liberal arts colleges across the state.
Students in the program volunteer 24 to 30 hours a week for eight weeks, gaining bedside experience and completing online coursework on death, dying and palliative care along the way. They also conduct research — last year students researched the changing nutritional needs of people in the final stages of life and turned it into an educational brochure for family members visiting the home to consult.
“Health care is very focused on cure — I’m going to cure this, I’m going to treat that, I’m going to give you medicine for this,” Weisse said. “But this experience forces students to step back and realize, there isn’t always a cure, but that doesn’t mean there’s nothing we can offer to alleviate your pain, your suffering. There is healing that happens at the end of life, and being present, being comforting and attentive is a form of medicine and it does provide healing.”
Liquori and the other student volunteers feel they’ve gained more invaluable insight into human health, psychology and empathy than they ever could have gained in the classroom.
Meditation room at the Joan Nicole Prince Home on Thursday, July 27, 2017 in Scotia, N.Y. The home is dedicated to providing a safe, comfortable and caring residence for terminally ill patients in need of a home during their final days. Five local college students are spending their summers caring for the terminally ill as part of a relatively new fellowship program offered by Union and Skidmore colleges.
Said Yohary Fabian, a 21-year-old pre-med student at Colgate University: “I want to be a doctor, and sometimes people die and you can’t save them. Sometimes there’s a disease and the knowledge for a cure just isn’t there yet. People suffer every day and we have to learn how to cope with it.”
Elisa Smith, a social work major at Skidmore College, found value in the art of silence — learning to be quiet and attentive, and not shying away from uncomfortable conversations.
“One of the hardest things has been listening to the residents talk about their fear of what’s to come,” she said. “But I found it was really helpful to (a resident) when I would sit out on the porch with him and just listen when he tried to talk about the things he was feeling. And I would say it’s one of the most life-affirming experiences I’ve ever had.”
Weisse’s dream is to one day grow the fellowship, which relies on grant funding, beyond the three homes it currently helps in the Capital Region. In addition to the Joan Nicole Prince Home, fellowship participants have volunteered at Mary’s Haven in Saratoga Springs and Gateway House of Peace in Ballston Spa. There are 30 such homes across upstate New York.
“We’re not going to learn how to be comfortable around death without practice,” she said. “And because health care and death have been so institutionalized over the years, we don’t really have a lot of practice anymore. This is sort of changing that culture.”
Part mortuary, part hotel, Japanese corpse hotels allow grieving families to spend the night near the bodies of their loved ones as they make their final farewells. Here’s a look inside of one.
[T]he minimalist rooms at the Hotel Relation here in Japan’s third-largest city are furnished with plain twin beds. Flat-screen televisions adorn the walls. Plastic-wrapped cups and toothbrushes are provided in the bathrooms. And just across the hall are the rooms where the corpses rest.
Checkout time, for the living and the dead, is usually no later than 3 p.m.
The Hotel Relation is what Japanese call an “itai hoteru,” or corpse hotel. About half the rooms are fitted with small altars and narrow platforms designed to hold coffins. Some also have climate-controlled coffins with transparent lids so mourners can peer inside.
Part mortuary, part inn, these hotels serve a growing market of Japanese seeking an alternative to a big, traditional funeral in a country where the population is aging rapidly, community bonds are fraying and crematories are struggling to keep up with the sheer number of people dying.
By custom, Japanese families take the bodies of their loved ones home from the hospital and sit for an overnight wake followed by a service the next morning in the company of neighbors, colleagues and friends. Then, in the afternoon, the body is sent to a crematory.
Continue reading the main story
But as neighborhood ties have weakened, funerals that once involved entire communities are increasingly the province of small, nuclear families. At the same time, Japanese society is getting old so fast and deaths per year are climbing so quickly that families sometimes have to wait several days before a body can be cremated.
The funeral for Hajime Iguchi at Sousou, a so-called corpse hotel in the Tokyo suburb of Kawasaki City, last year.
The corpse hotels offer a practical solution — a place where a body can be stored at low cost until the crematory is ready, and where small, inexpensive wakes and services can be held outside the home.
“We can say the supply doesn’t meet the demand,” mainly in urban areas, said Hiroshi Ota, an official at the Japan Society of Environmental Crematories. While Japan has an estimated 5,100 crematories, Tokyo, with a population of more than 13 million, has just 26.
“The demand for cremation will increase until the baby boomers disappear,” Mr. Ota said.
Japan has funeral parlors, too, an industry that developed as people moved from the countryside to the cities and it became difficult — and often impossible — to take corpses into high-rises. But they cater to larger groups and more elaborate ceremonies, and these days, that can seem a bit much.
In the bubble economy of the 1980s, “Japanese funerals were based on showing off to other people, and people cared how they were viewed by others,” said Midori Kotani, executive researcher at Dai-ichi Life Research Institute, an arm of one of Japan’s largest insurance companies. “But fewer and fewer people talk to their neighbors, so they don’t have to show off or think about how they are viewed by them.”
The corpse hotels are used by families who want a simpler affair, or want to skip a funeral altogether. According to Ms. Kotani, about 30 percent of deaths in the Tokyo area are not marked by a funeral service, up from just 10 percent a decade ago.
After cremation, families usually keep the ashes at home for 49 days before a burial service at a cemetery. On the 49th day, according to Buddhist tradition, the dead are believed to arrive at the next world.
Mr. Iguchi’s body on its way to a crematory.
When Hajime Iguchi died at age 83 last autumn, his sister and brother-in-law held his wake and funeral at Sousou, a corpse hotel in the Tokyo suburb of Kawasaki City. Mr. Iguchi, a lifelong bachelor, had died in a nursing home after a protracted illness, and had few friends left.
“Back in the day, we used to have funerals at home, but times have changed,” said his sister, Kunie Abe, 73. “Neighbors all used to know each other and would help one another out. But today, you don’t even know your next-door neighbor.”
The demand for “itai hoteru” is likely to grow. Last year, 1.3 million people died in Japan, up 35 percent from 15 years earlier, and the annual toll is expected to climb until it peaks at 1.7 million in 2040, according to the Ministry of Labor, Health and Welfare.
About 37 percent of Japanese women who died last year were over 90, with few surviving friends to mourn them. And close to one-fifth of Japanese men never marry or father children, leaving behind few relatives to plan or attend funerals.
The number of people dying alone is also on the rise. In Tokyo, for example, the number of people over 65 who died alone at home more than doubled between 2003 and 2015, the latest year for which government figures are available.
At the Hotel Relation here in Osaka, about a third of the customers forgo a formal funeral. Instead, they sit in the rooms with their dearly departed for a day or two, with only close family in attendance, and then send the bodies for cremation.
Relatives of Mr. Iguchi departing the crematory with his ashes.
“In the past, if you heard someone held a funeral just for family members, people in the neighborhood would say, ‘What kind of people would hold a family-only funeral?’ But now it is accepted,” said Yoshihiro Kurisu, the hotel’s president.
Corpse hotels are more economical than large funeral homes. According to the Japan Consumer Association, the average funeral in Japan runs 1.95 million yen, or about $17,690. The cheapest package at the Hotel Relation costs 185,000 yen, or about $1,768.
The package includes flowers, a room for the family to spend the night in the same room as the corpse, a traditional white gown for the deceased, a simply decorated coffin, transport of the body from the hospital and then to the crematory, and an urn to hold the ashes. Each additional night costs 10,800 yen, just under $100. Families who want separate rooms, wakes or funerals pay extra.
“Itai hoteru” first appeared about five years ago in Japan’s largest cities, and there are only a few across the country. Some have angered residents who do not want to live in such proximity to death and mourning.
Near the Sousou hotel in Kawasaki City, signs on fences protest, “Corpse storage: absolutely opposed!”
Hisao Takegishi, the hotel’s owner, said he understood why neighbors were uncomfortable. But he said his staff tried to be as discreet as possible when bringing in bodies.
A cemetery outside Tokyo. Nearly all people who die in Japan are cremated.
Inside, Mr. Takegishi painted the walls in pastel colors and equipped the rooms with green sofas and stools. They look more like start-up break areas than a setting for wakes or funerals. The entryway, with shelves of plants and a few books, evokes a spa.
“I did not want it to look too sad or lonely,” he said. Sousou has relationships with funeral directors and monks, and can help clients plan modest services.
Yuki Matsumoto, the executive director of the All Japan Funeral Directors Co-operation, which represents about 1,340 long-established funeral homes, said some owners of the new businesses paid little regard to standards or the dignity of the dead.
Japan does not require a license to open a funeral business, and there are few regulations for how they operate. “So in this situation, it is possible that bad-intentioned businesses can enter the industry,” Mr. Matsumoto said.
But Mr. Kurisu at the Hotel Relation said traditional funeral homes just resented the new competition. “I am hated by people in the business because I am driving down the prices of funeral services,” he said.
At Mr. Iguchi’s tiny funeral ceremony last fall, a monk chanted last rites as his body rested in a coffin lined with white satin. Five guests, all relatives, sat in folding chairs nearby.
After the chanting, they rose to lay flowers and origami cranes on Mr. Iguchi’s body, making a bright garland around his head and on his chest.
His sister, Mrs. Abe, leaned close to her brother’s ear. “So long,” she whispered.