In their 1976 classic, (“Don’t Fear) The Reaper,” Blue Öyster Cult sang that “40,00 men and women” die every day. Today, that number is more like 151,600. That’s a lot of bodies, and frankly, we’re running out of places to store them all. Ignoring sustainability entirely, how we dispose of our deceased is becoming a big problem. In Sweden, for instance, your grave is dug up twenty-five years after burial, your corpse is pushed farther into the ground, and another body is added on top—there simply isn’t space for new bodies. The Swedes are known for their compartmentalization (I see you, IKEA! Loveyour meatballs!) but when it comes to our final resting place, there’s got to be a better way.
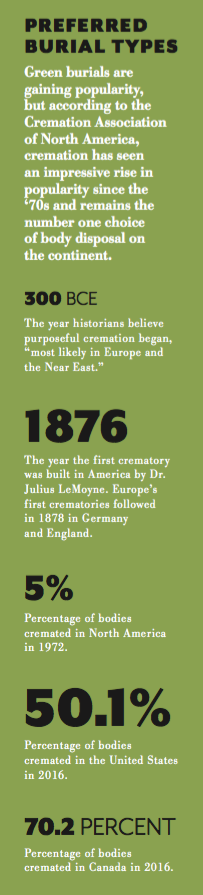
Environmental activist Edward Abbey, famously buried in the desert in a sleeping bag, stated that “[After] the moment of death . . . we should get the hell out of the way, with our bodies decently planted in the earth to nourish other forms of life—weeds, flowers, shrubs, trees, which support other forms of life, which support the ongoing human pageant—the lives of our children. That seems good enough to me.” And today, you can do just that. Although cremation remains the number one choice of disposal in North America, and traditional burial a close second, green practices are quickly catching up.
Cremation does indeed create less waste than a traditional casket and land plot, but the “natural gas that goes into a cremation is [equivalent to] two full tanks of an SUV, or a 500-mile car trip,” as mortician, author and “Good Death” advocate Caitlin Moran told Jezebel. Perhaps more disturbing is the amount of mercury released into the atmosphere during cremation due to…brace yourself…our dental fillings. You don’t see a pamphlet about thatat the dentist’s office. Bestselling author Mary Roach notes in Stiff: The Curious Lives of Human Cadaversthat “the average amount of mercury released into the atmosphere” is “three grams per cremation.” Maybe we all should have flossed more?
If you lived your life sustainably, why wouldn’t you die sustainably? We’ve provided an intro to green burials, but this is just the tip of the iceberg. You can be buried on a funeral pyre, thanks to the help of organizations like the Crestone End-of-Life Project; you can donate your body to science, perhaps at The Body Farm, where your decomposition will help forensic scientists solve crimes; or you can go full-on Edward Abbey and decompose back to the earth. (The legality on that last one is iffy, but hey, chase your bliss). We’ve all got to go sometime. Know your options, create a plan with your loved ones and research, research, research. Make your memorialization an eco-conscious testament to the way you lived your life.
What Constitutes a Green Burial?
To be considered “green,” according to Ellen Newman of the Good Green Death Project and TalkDeath, a burial must adhere a few basic standards:
For the Body:
-No embalming fluid.
-Natural shrouds or compostable/recyclable “basket casket” are utilized. Youcanhave a casket, but it must be made from biodegradable materials. Remains (if in powder form) must be in a biodegradable container.
For The Gravesite:
-No grave markers. Naturally occurring markers like trees or stones are fine.
-No vaults or grave liners.
-No non-native species planted on burial grounds; no maintenance for the plants or grounds.
Grief is a horrible emotion to feel, because it means that something has happened in your life that you wish you could avoid. In most cases, it’s because of the loss of a friend, family member, pet or other loved one. But just what happens when you experience grief and what should you do about it? Understanding the 7 stages of grief will start you off right.
The 7 Stages of Grief
Shock & Denial
When someone first brings you that bad news it can be difficult to believe it’s even real. You want to just shake your head and say ‘no way.’ You may start to feel a little numb and may feel no pain at all at the loss because of this. The shock and disbelief are actually suspending your pain and this may last for several weeks.
Pain & Guilt
Once your shock starts to fade away you’ll start to notice the pain. This is when it first starts to hit you that your loss is real. The pain may be extremely hard to handle and it may feel physical as well as mental and emotional. You may even start to feel guilty about something that you could have done or should have done for the person (even if it’s illogical).
Anger & Bargaining
Next, many people start to feel angry. You may feel angry with your religion, with someone who was taking care of that person, with the person in the other car that hit them or anyone else. It may be completely unreasonable who you feel angry with but you seek out someone you can blame for the loss and may even attempt to bargain to bring that person back.
Depression, Reflection & Loneliness
Generally this is one of the later things to take effect. When many of your family or friends are starting to overcome their suffering or starting to think that you should be overcoming your own suffering, you start to feel depressed. Even though the pain towards the beginning is hard, this may hit you even harder, because you’re truly coming to terms with what you’re going through and the loss you’ve experienced.
You’re not feeling the pain as much as feeling the change to your life that losing this person has made. Maybe you’ve lost someone you spend a lot of time with or the person you always told secrets to. These difficulties are going to start to cause depression, reflection on the old way things were and loneliness as you realize those times are gone.
The Turn
Finally, just when you think there can’t possibly be anything good coming ever again, you’ll start to experience the turn. You’ll start to feel a little better each day. It may be so slight that you don’t even realize it at first, and you won’t feel happy all at once. What you may feel is a little less pain, a little less sadness and more of a feeling of being okay.
Reconstruction & Working Through
This is where you’ll start to work your way through the aftermath of losing that loved one. Maybe you have to take care of some financial troubles either caused by the loss or the grief you went through while dealing with the loss. Maybe you need to just put yourself back together. This is the stage where it all begins.
Acceptance
The final stage is the one you’ll be in for the rest of your life. This is the one where you start to accept the loss fully and start to move on with your life. That’s not to say you ever ‘get over it’ but that you start to feel okay about it and you’re able to think about them and even talk about them again without feeling the despair or intense pain. It may make you sad to think about them, but it may also make you happy because now you can remember and be happy about the good times.
Keep in mind that the stages of grief are different for everyone. You may only spend a few days in disbelief and your sibling may spend weeks there. You may never go through a bargaining stage while your best friend spends a lot of time with it. There’s no right or wrong way to grieve, and there’s no timetable for an acceptable length of time to grieve. Getting through this pain, however, can be extremely difficult to do on your own. Seeking out professional help, like what you can get from Better Help, can make a huge difference in your life and in your healing process.
Threshold Choir members pray before visiting a patient at the Halquist Memorial Inpatient Center in Arlington, Va.
by Debra Bruno
[I]t’s a quiet afternoon at the Halquist Memorial Inpatient Center, a hospice, as four women huddle close, talking quietly in a tight circle before walking through the doors to sing to men and women on the threshold of death.
These women are part of the Threshold Choir, a group that brings the comfort of song to dying people.
A thin woman, who is in the last weeks of life, is the choir’s first stop. She is sitting nearly upright in a hospital bed, her daughter beside her. Leslie Kostrich, the group’s leader for this day, asks the older woman if she would like to hear a few songs. She nods; the singers set up folding stools and pull up close to her bed.
“We sing in a circle of love,” the women sing, a cappella and in three-part harmony. “In music we are joined.” As they sing, the woman gazes off with a faraway look in her eyes, as if she’s trying to remember something.
The group sings another song, and as they finish, the older woman claps softly. “Thank you,” she says. “Nice.”
It takes sensitivity, situational awareness and a dash of emotional intelligence to sing to the dying. The sound of soft harmonious voices can be very comforting as life closes down, but the songs can also bring forward the immediacy of death to family members sitting nearby. Singing in such an emotional environment takes practice and a recognition that it is less a performance than a service.
For the dying and their families, the singers are hoping to bring peace, comfort and a feeling of love. “We call it kindness made audible,” says Jan Booth, who with Kostrich is co-director of the Washington-area Threshold group.
It is also very life-affirming for those who sing in this unusual choir.
“When I tell people I’m in a choir that sings at the bedside of the dying, they’ll say, ‘Oh girl, what a good thing,’ or ‘Girl, you must have lost your mind,’ ” says Kadija Ash, 66.
But the opposite is true. “Sometimes I run” to rehearsals, she says, “because of the healing.” In the two years she has been a member of Threshold, Ash says, she has gone from having a fear of death to an ability to be more accepting of life’s ups and downs.
Kostrich, 60, who has been with the group for three years, likewise says: “This has changed my life. That’s not an exaggeration. It gave my life a spiritual dimension that I was totally unprepared to receive.”
Threshold Choir — which has more than 200 groups around the world — seems to have tapped into something both primal and much-needed: a growing desire not to recoil from death or abandon the dying but to face that ultimate truth and figure out how to help ease the isolation of those near the end.
Bedside singing is a way of “normalizing death,” says Kate Munger, 68, who founded the first group in the San Francisco area 18 years ago. Many of the choirs are started and run by baby boomers, who are comfortable shaking up the accepted way of doing things, Munger says. “We’ve done that for childbirth, for education, and now for our impending death.” She says the number of people participating in Threshold Choir has grown to about 2,000.
Similar deathbed choirs have also surged, including Hallowell Singers, based in Vermont, which recently celebrated its 15th year, says founder Kathy Leo. She estimates that Hallowell has as many as 100 spinoffs, mainly in the United States.
Although they sing some requested songs, such as “Amazing Grace,” Threshold Choir mostly uses a repertoire designed for singing around a dying person. The pieces tend to be limited to just a few words, and sung without accompaniment in three-part harmony.
The idea is to keep things simple and not tied to any spiritual tradition — for instance, “Thank you for your love” and “We are all just walking each other home.” Complicated verses could intrude on the process of dying, which often involves people retreating from the day-to-day and reviewing their lives.
During the afternoon at Halquist, the four Threshold singers — Booth, Kostrich, Ash and Margo Silberstein — move out into a hallway after their first group of songs. One hospice staffer says, “I love working on Thursdays because I love listening to this group.”
The group slips into another large room with four beds separated by curtains. A frail woman with brilliant blue eyes smiles at the group. In another bed, someone is making noises that are halfway between breathing and groaning.
The blue-eyed woman asks, “Do you know ‘A Mighty Fortress?’ ” The group knows some of the words to the hymn but ends up mostly singing “oooo” to its tune. After they finish, Kostrich offers, “We do have ‘Amazing Grace.’ ” “Oh yes,” the woman answers and quietly sings along with them. After they finish, she says: “Oh, thank you. That was just wonderful.” They go on to sing “Simple Gifts” and “He’s Got the Whole World in His Hands” and then a few Threshold songs.
A TV next to a different bed blares.
After they finish, they approach a man sitting at the bedside of a woman. Can they sing?
“She’s pretty well gone out, but you can try,” he says.
As they sing “Hold this family in your heart,” the man’s eyes redden. He shifts in his seat. They sing, “Rest easy, let every trouble drift away.” His chin starts to tremble. As they begin to sing “You are not alone,” the woman begins to breathe more loudly but doesn’t move. The woman in the bed across the room, where they first sang, calls out, “Beautiful!”
An hour later, as the group gets ready to leave the hospice, Kostrich says that singing with Threshold has given her a way to process her own family’s experiences with death. When her parents were dying in the 1980s, Kostrich says, no one acknowledged they were close to death, which didn’t allow her and her family to come to terms with the losses themselves. The Threshold Choir has both helped her in a small way alleviate her own loss and help others avoid that kind of pain, she says.
There’s another thing that comes out of Threshold singing: community. And that feeling is evident when group members get together for a twice-a-month rehearsal, often in a church basement in the District. All but one singer at this rehearsal is female, but they range in age from 20-somethings to 70-somethings, African American, Chinese and white, those with tattoos and those with carefully coifed hairdos. There are a lot of hugs and laughter.
Olivia Mellon Shapiro, 71, says that group members are her “kindred spirits.” When she retired from her work as a psychotherapist, she told a friend, “Now I want to sing people out in hospices,” Shapiro says. “My father sang himself out — he died singing, and I was very moved by that.” Her friend said, “Oh, that’s the Threshold Choir.”
“Now I have a new group that feels like home to me. It really does,” she says. “I’ve also always been a little afraid of death and dying, but I’ve always loved the idea of hospices. So the idea of singing people out in hospices to get more comfortable with the idea of death and dying appealed to me.”
(The group sings several times a month at Halquist in Arlington and also at Providence Hospital in Northeast D.C. through the nonprofit hospice provider Capital Caring.)
One of the singers, Lily Chang, 28, notes that the choir is helping her confront her own fears of loss.
Chang says she’s very close to her grandmother and, given her age, worries about her. “I remember telling my mom, ‘I don’t know what I would do’ ” if she died. “Thinking about it, engaging with it in different ways makes me feel better.”
[C]are at the end of life should address all of the important elements that play a critical role in ensuring a positive end-of-life experience for patients and families. Therefore, quality end-of-life care extends beyond managing physical pain to include psychosocial and spiritual needs.
Not all long-term care professionals carry the same understanding of the issues.
Frequently, nurses serve as advocates to support patients and families in making care decisions based upon their goals and values. Ideally, physicians, nurses and other team members work together to create an atmosphere of care and compassion in accordance with patient and family wishes.
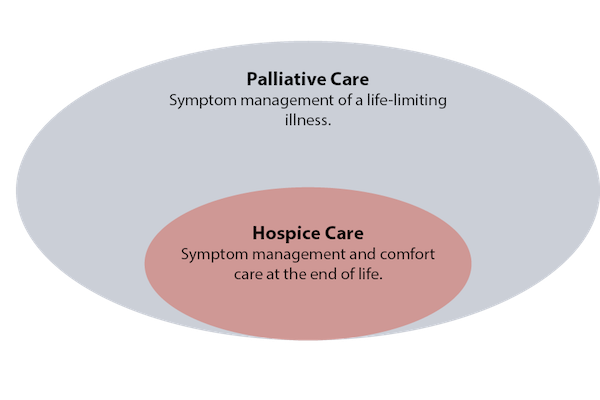
Although hospice and palliative care both aim to deliver quality holistic care, there are key differences.
The dimensions of hospice care
Hospice is the model for quality compassionate care for people facing a life-limiting illness. Hospice clinicians focus on pain and symptoms, and attend to the patient and family’s emotional and spiritual needs. Hospice is offered at a patient’s residence, such as their home or nursing home, or, if needed, in a hospice facility.
Hospice programs utilize an interdisciplinary team (IDT) approach to plan the care needed by patients and their families during the final weeks and months of life. The IDT is comprised of nurses, chaplains, social workers, physicians and medical directors, hospice aides, volunteers, bereavement specialists and other clinicians who develop and implement a plan of care that is formulated to relieve anxiety and suffering during the final months and weeks of a patient’s life. This approach allows the team to address physical, emotional, spiritual and social concerns that arise with advanced illness.
Hospice is available to people with all types of conditions and diseases, and focuses on comfort — not cure. Hospice provides care for the “whole person,” including physical care, counseling, spiritual needs, drugs, equipment and supplies related to the conditions that comprise the terminal prognosis. It also supports family caregivers, including bereavement support for up to a year after the patient’s death.
Financing hospice
Hospice care is reserved for people at the end of life who meet Centers for Medicare & Medicaid Services eligibility requirements and elect a comfort approach to care. The Medicare Hospice Benefit (MHB) requires that two physicians certify that a patient has less than six months to live if the disease follows its usual course. However, if a patient is still alive after six months, he or she can continue to receive hospice services if he or she meets eligibility requirements and demonstrates signs of progressive decline.
When a patient elects hospice, they sign off their Medicare Part A (hospital insurance) and enroll in hospice under the MHB. From that point on, hospice covers all services and care related to the terminal diagnosis and related conditions through Medicare, Medicaid and most commercial insurance.
The hospice IDT, together with the patient’s attending physician, is responsible for determining the plan of care. Under terms of the Medicare Hospice Benefit, the hospice agency is responsible for the plan of care and may not bill the patient for services. All costs related to conditions that affect the terminal prognosis are paid from a per diem rate that the hospice agency receives from Medicare. This per diem rate includes all drugs and equipment, nursing, social service, chaplain visits and other services deemed appropriate by the hospice agency. Care and medications not related to the terminal illness or related conditions continue to be paid for through original Medicare.
Distinctions of palliative care
The biggest differences between hospice and palliative care revolve around where the patient is in their illness related to prognosis, their goals/wishes regarding curative treatment, and how palliative care is financed.
Palliative care focuses on relief from physical suffering and caregiver burdens for individuals who are living with a chronic disease that may or may not be terminal, addressing their physical, mental, social and spiritual well-being. Atul Gawande recently defined palliative care “as the field devoted to providing people with serious life-limiting illness with expert care that serves their goals for quality of life, not just quantity of life.”
Similar to hospice, palliative care utilizes an interdisciplinary approach with highly trained professionals, including physicians, nurse practitioners, nurses, social workers, chaplains, and other disciplines.
Palliative care can be offered to people of any age, without restriction as to disease or prognosis. It may be appropriate for anyone with a serious, advanced illness, whether he or she is expected to recover fully, live with chronic illness for an extended time, or experience disease progression. Unlike hospice, patients receiving palliative care may continue to receive aggressive treatments, including life-prolonging therapies.
Conditions appropriate for palliative care include cancer, congestive heart failure, end stage renal or liver disease, chronic obstructive pulmonary disease, and dementia, among others. While palliative care is often appropriate earlier in the disease trajectory, referrals to palliative care clinicians are often not made until late in the disease process.
Palliative care focuses on relieving symptoms, such as pain, shortness of breath, fatigue, constipation, nausea, loss of appetite, difficulty sleeping and depression. Palliative care providers also support patients in carrying on with daily life so that they can tolerate medical treatments. In addition, patients receive support that empowers them to have more control over their care by improving communication so that they can better understand their choices for treatment. Helping patients and their caregivers coordinate care across care settings is a hallmark of palliative care.
Financing palliative care
Unfortunately, palliative care programs struggle financially because there is no reimbursement code specifically for palliative services and Medicare does not reimburse for interdisciplinary care management. Hospital-based palliative care is paid by the health system with some fee-for-service (FFS) billing for physician services. Medicare Part B covers physician and nurse practitioner (NP) fees for outpatient care delivered in the community or in clinics. Therefore, most community-based palliative care programs utilize NPs and physicians for home visits.
Other disciplines, such as nurses and social workers cannot bill Medicare for palliative home visits. Palliative care is also paid for through flexible bundled payments under Medicare Advantage, Managed Medicaid, ACOs and other commercial payers.
While Medicare doesn’t have a palliative care benefit, CMS has authorized demonstration projects that are testing different ways of meeting the needs of seriously ill patients. The Medicare Care Choices Model allows patients to receive hospice-like support services while concurrently being treated for their illness.
Demonstrated value
Costs for palliative care teams and programs are offset by fewer trips to emergency departments and lower hospitalization and rehospitalization rates. In addition, patients and families rate the value of palliative care services highly. This explains why 80% of hospitals with 50 beds or more have established palliative care teams and some are starting to consider outpatient palliative care programs. In addition, health plans and payers, including Accountable Care Organizations (ACOs), Integrated Delivery networks (IDNs) and other types of provider-driven managed care organizations, are beginning to offer community-based palliative care programs to their patients/members to extend the benefits of palliative care into the home.
Palliative care programs and advance care planning that include earlier conversations about patient and family goals of care are consistently demonstrating their value in helping patients live their final days in accordance with their wishes. Data shows that in communities that provide greater access to palliative care programs, patients are less likely to die in the hospital.
Furthermore, findings show that patients experience fewer admissions to the intensive care unit in the last six months of life and are less likely to die in an ICU
Today, palliative care is becoming recognized as option at any stage of advanced illness, not simply reserved for care at the end-stage of life. Its use should be driven by patient need, not disease prognosis. Hospice care remains the gold standard for end-of-life care. Together, hospice and palliative care offer compassionate care when it is needed most.
[I] was in elementary school when I first became aware of my own mortality. It was early in the morning. My mom was in the bathroom getting ready for work, and I was on her bed covered in tears, thrashing around and yelling “I don’t want to die!” over and over.
Like a lot of people, dying terrifies me, the finality of it so unthinkable that I try not to acknowledge it in my day-to-day life. So when an opportunity came to go to “Second Chance” — an interactive experience that uses theater and virtual reality to help people come to terms with their demise — I was both scared and intrigued. It was one of 175 activities that took place during Reimagine End of Life week in San Francisco, an event that consisted of panels, film screenings, and other experiences that encourage people to talk openly about death and how it affects us.
SF-based art collective Lava Saga spent three months creating “Second Chance,” transforming a two-story gallery in the city’s Mission district into an ethereal environment.
“We believe that immersion is a way to experience things, and when we have those lived and bodied experiences, we can start to answer some of those big questions around death or around life itself or any other big topic we’d like to explore,” said co-producer Scott Shigeoka in an interview.
“Second Chance” only allowed 10 people in at a time, and they all had to be strangers (one of Lava Saga’s few hard rules). It unfolded across four different rooms, with VR serving as a key piece of the production. My group entered the first space — a darkened room lit only by blue and purple lights — and found black futons on the floor, all of which had pillows and neatly folded white sheets. Next to them were Samsung Gear VR headsets and wired headphones that attendants asked us to put on after we sat on the beds.
The nearly four-minute VR sequence pulled me through a monochrome landscape filled with massive planets, intricate caverns, and pulsating tendrils that pierced the sky. An otherworldly hip-hop track from electronic artist Shigeto made the 360-degree journey feel lonely and isolating.
When the experience was over, I took the headset off and laid on the bed; another person came to pull the white sheet up to my neck. A cellist at the corner of the room began playing a peaceful but melancholic tune. I closed my eyes as our end-of-life doula (who had spoken to the group beforehand to address any concerns) read a poem from Buddhist monk Thich Nhat Hanh.
As far as the “Second Chance” narrative was concerned, we were dead.
Simulating Death Surprisingly, the VR music video wasn’t made for “Second Chance.” It’s a pre-existing project (known as “Hovering”) from creative studio 79 Ancestors. Lava Saga worked with VR and augmented reality curator Dream Logic to determine what kind of piece would best represent the transition between life and death.
It wasn’t easy. For awhile, they wondered whether they should even have a symbolic representation of death. After all, how do you visualize an experience that, by definition, is impossible to come back from?
“We picked [‘Hovering’] because it feels like going through a portal. And with VR in ‘Second Chance,’ we wanted it to serve that function, to be a transporting mechanism that people could go inside, be transported, and come out into a shifted reality,” said Dream Logic producer Kelly Vicars.
Though “Hovering” wasn’t created with “Second Chance” in mind, its abstract graphics made it a fitting choice for the production. During the design process, Lava Saga interviewed people who had near-death experiences, with many of them saying they were moving through a tunnel or seeing black-and-white images before being resuscitated. “Hovering” also worked well because it wasn’t scary and didn’t adhere to any specific religious beliefs.
“It was important for us to honor the diversity of cultures, traditions, and wisdom around death. … We wanted to make sure that whatever experience we used was really inclusive,” said Shigeoka.
Lava Saga and Dream Logic knew that for a lot of people, “Second Chance” would be their first opportunity to be in VR. So they tried to make the experience as seamless as possible, with attendants giving clear instructions on how to use the equipment. And Gear VR offered the least amount of friction due to its portability and ease of use (when compared to PC-based gaming headsets like Oculus Rift and HTC Vive). Participants just had to put it on and wait for “Hovering” to begin.
“My team’s goal is to use immersive technology to elevate art, to have the technology disappear,” said Vicars.
Breaking through taboo topics After dying in VR, my group entered a series of rooms that represented a kind of liminal purgatory state. One had thin sheets of white fabric hanging from the walls and ceiling, with actors and dancers (Lava Saga refers to them as spirits) talking to each other about their previous lives.
From there, “Second Chance” starts to pull back on its mystical interpretations of an afterlife and morphs into something a little more grounded: group therapy.
In the third room, we broke into two smaller groups with trained facilitators who asked us questions about our own lives. Shigeoka said this was often an “emotionally charged” space because of the stories people would share — about their hardships, mourning for loved ones who died, or anything else they just needed to talk about. This vulnerability is why it was so vital to go through “Second Chance” with strangers instead of friends or family members.
I didn’t let my guard down completely. I couldn’t quite squash the skeptic voice in my head, which was too loud and too stubborn to go away. But I still felt comfortable in those discussions, as well as in the 1-on-1 meetings that followed in the last room, where we were randomly paired with another person from our group. That I was able to share personal details about my life at all was remarkable given that we had only met an hour before.
“Second Chance” wasn’t a perfect experience; at times, I was bored or confused about what was going on. But the core conceit — getting people to express their feelings about a sensitive topic — was sound. It reminded me that sometimes, it feels good to have someone just listen to you.
“I hope that people emerge [from ‘Second Chance’] with a new perspective and a new relationship with what it means to die. And that’s [to] live,” said Vicars.
Lava Saga and Dream Logic consider this first run as a prototype. If the show ever returns (whether in San Francisco or elsewhere), they want to keep refining it based on the feedback they receive. One day, they might make their own VR experience to replace “Hovering,” or maybe even depict that life and death transition in a totally different way.
But the idea of using theater and immersive technology to break through cultural taboos is something both teams want to keep exploring.
“It’s so important for us to open up about [death] and it’s so important for us to change the narrative around it, to make it something that should be discussed and talked about. … We need to have a conversation that goes beyond the medical world around the end of life,” said Shigeoka.
[T]he perfect coffin for a gerbil is a Celestial Seasonings tea box. With the tea bags removed, the white wax-paper bag inside is the ideal size funeral shroud for a tiny body. This unfortunate factoid, like much of the information about how to dispose of a beloved pet’s body, comes from personal experience. I buried four gerbils in my backyard as a child, complete with incense on their graves and a few words.
As an adult with a puppy well on his way to being over 60 pounds, I hadn’t given much consideration to how I’d deal with other pet deaths until a friend asked me, “this is a terrible question, but what do you do when he dies?”
I dug into the question, and as I did I found that I wasn’t alone in wondering—but that there isn’t a great answer.
The experts I talked to emphasized that our relationship to pet loss has changed over the last century. “It’s not surprising to me that we feel such grief over the loss of a pet, because in this country at least they are increasingly considered family members,” says Leslie Irvine, a sociologist at the University of Colorado-Boulder. Sixty-eight percent of Americans own a pet, an increase of twelve percent since surveys of pet ownership started in the 1988, when it was already booming. Losing a beloved animal friend is made harder by the relative novelty of the experience, often being a person’s first experience with a close death, and by it being one of the few times most people chose euthanasia to end a life. And depending on the relationship, the loss of a pet can be more traumatic than the grief we feel after the death of family and friends. In part, this is because pets share some of our most intimate relationships—we see them every day, they depend on us, we adjust our lives around their needs—and yet publically grieving their loss is not socially acceptable.
We haven’t always felt this way, though. As a society, Irvine says, we’ve moved from thinking of pets as accessories or mindless pieces of furniture to thinking, feeling beings.
Pets become family members because they actively shape how we live. “A lot of people who have pets wake up at a certain time, not because of any alarm clock or any need of their own but because their dog needs a walk,” says Irvine. “Just as other humans participate in becoming family by doing these practices—getting up together, eating together, navigating the bathroom times, and all that—so do animals become part of the rituals that make family.”
And it isn’t just a daily ritual that makes pets familial. We form attachments to animals in the same way that we form attachments to people, says Cori Bussolari, a psychologist at the University of San Francisco. She points to a study in Science from 2015 that found when people gazed into a dog’s eyes, both the person and the dog had increased levels of oxytocin. Oxytocin, sometimes called the love hormone, regulates social interactions. It’s released when humans stare into each other’s eyes, and when parents look at their newborn children. “I’m sure if you did the study with other animals it would be the same,” Bussolari says.
I already imagine losing my puppy will be harder than burying my gerbils, but I also didn’t stare into my gerbils’ eyes quite as much. No matter the species, our bonds with our pets are unlike our other relationships. For one, Bussolari says, they’re entirely dependent on us. For another, Irvine says, “we idealize animals, especially dogs. We create them as these almost angelic characters, so we have this idea of unconditional love for us.” When they die, she explains, it almost seems like a violation of this mythos we’ve built around them.
On a personal level, the death of a pet is often a person’s first exposure to the loss of a close relationship, says Thomas Wrobel, a psychologist at the University of Michigan-Flint. Human death has been relatively sanitized, he explains. We have an industry for funerals and cremations, and you don’t typically have to deal with a dead body yourself. “With pets it’s a lot more in your face,” says Wrobel. “Unless you do the cremation option, you’ve got this dead dog you have to deal with, which is a lot more intimate experience of the death.”
With pets, you also have to decide if you are going to euthanize, and when. In a study of 305 pet owners, Bussolari found that almost seventy percent chose to euthanize their pet. It’s often medically necessary—the kindest thing to do for a dying animal—but the decision can wrack the owner with guilt. In 2005, Wrobel did a study of the relationship between symptoms of grief and attachment to pets. “In our results we saw that guilt was way up there [on the list of emotional responses], because a lot of people are carrying the animal to where it would be euthanized,” says Wrobel.Years ago, my cat, who I had rescued as a kitten, developed a urinary tract infection that lingered due to a weakened immune system from his feline HIV. I’d tried everything to help him get over it. One day, I came home and saw from his tepid movement that he was clearly in incredible pain—he was dying. Driving to the vet was excruciating, and my mom had to be the one in the room when he was euthanized because I was too upset.
“After the passing of a pet ninety-nine percent of people say to me in some shape or form, this was harder for me than the loss of my mom, or my grandma,” says Dani McVety, veterinarian and CEO of Lap of Love, a veterinary hospice network. She has found that the option to have in-home euthanasia and pet hospice makes death easier for families.
In-home euthanasia helps remove the negative experience of knowing that you’re driving your pet to their death in a place that you know causes them stress. In her practice, she sees the same kind of anxiety over deciding the right time for euthanasia at the end of a pet’s life. “I’ll tell them, I know you don’t want to hear this right now, but when this is done, you will feel relief,” McVety says. “And people do this thing after it’s done. . .they stand up and put their hands on their head and say, ‘Oh my gosh, I feel so relieved.’”
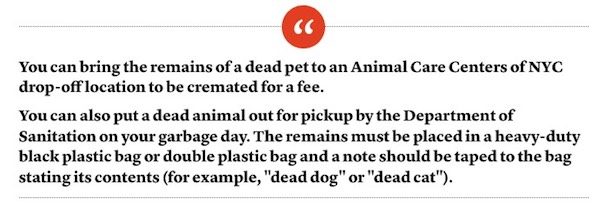
But despite the fact that 68 percent of Americans own a pet, and have grown to treasure them like members of the family, taking care of a dead animal’s body isn’t the same as dealing with a human corpse. In New York City, if you look up what to do with a deceased pet on the 311 page, you come to this statement:
If you think that’s appalling, you’re not alone.
“Wow. Wow, you end up just treating it like a raccoon. Wow, that’s crazy,” says McVety. The New York Department of Sanitation doesn’t keep data on how many pets are left on the curb so it’s unclear how often this happens. Other major cities, like Houston and Los Angeles, will pick up pets curbside, and in other cities you can call for pickup.
These guidelines are written so that the city has some response available, but they don’t take the emotional element into consideration, says Bonnie Beaver, professor of veterinary medicine at Texas A&M.
City services aren’t the only ones to fail to see how emotional a pet death can be.
“You feel often isolated, socially,” says Beaver, “because people don’t understand what you’re going through, because they might say, ‘get over it, it’s just a dog’—which is exactly the wrong thing to say.”
When you lose a person, there are rituals—the funeral, the memorial—and it’s acceptable to take time off work and talk about your loss. “What people grieving the loss of a pet don’t realize the first time they lose a pet is the strength of the grief and how long it lasts,” says Wendy Packman, a psychologist at Palo Alto University. “So it surprises the griever, and it really surprises the people who aren’t sympathetic to pet loss.” Although Packman has found that the depth and length of grief is similar to how we grieve people, this social stigma causes it to feel more painful.
“With disenfranchised grief is there is less support, and the grief can be even worse than for a person because there are no rituals,” says Packman, “and when people do go out and do a ritual, when they feel brave enough, they can be ostracized.”
As I was researching this story, friends told me about the lengths they went to in order to bury their pets properly, despite regulations about where and how you may dispose of animal remains. One snuck into their community garden at midnight to bury a pet rat under a rose bush. Another drove out in the middle of the night to bury their cat underneath a beautiful oak tree they pass on their daily commute. Even my gerbil burials, and the funeral I held for my cat were private affairs, in the backyard with my family—our secret, quiet grief shared together.
Packman believes this social acceptability of grieving for pets is changing, noting that she’s seen a rise in memorials for pets and pet cemeteries. But in the meantime, says Bussolari, we grieve our pets so deeply because we feel like we’re not supposed to. “We worry a lot about making people uncomfortable, because then they don’t want to be around us—and if they don’t want to be around us then we’re by ourselves,” she says. “But the reality is that the more we talk about grief, the more we normalize grief.”
CENSUS
By Jesse Ball
272 pp. Ecco/HarperCollins Publishers. $25.99.
[J]esse Ball is one of our most prolific experimentalists. His last few novels, starting with the excellent “Silence Once Begun,” demonstrate a mature style that feels less like an experiment than a means to communicate deep emotional truths without the clutter of too many narrative conventions.
“Census,” Ball’s eighth and latest novel, may be his most emotionally affecting book to date. It is also his most transparent. In a candid preface, Ball explains that he wrote “Census” in memory of his brother, Abram Ball, who had Down syndrome. Ball sets out to write a book that captures “what it is like to know and love a Down syndrome boy or girl.”
In “Census,” a father and son journey across a nameless, dystopian land. The father, a recent widower and retired doctor, has just received news that he is dying. Both he and his wife had always meant to travel, but because their son was born with Down syndrome, they talked themselves out of it. The cruelty of others kept them from the road: “Ever since he was born, our lives, my wife’s, mine, bent around him like a shield.” Now, with his wife passed on, his son grown and his own end very near, he devises a plan to become a census taker, which will take him and his adult son on a cross-country road trip.
The census itself is part of the novel’s central mystery. It is both a survey of the population and an existential measurement. The father explains, “I must, in speaking to a person, know what is special about that individual, and that data must pass through me … in such a way that what is … most special about the nation … could be known and felt.” He asks participants to tell their own unique stories, after which they are marked — tattooed — on a rib, proof that they have been tallied. While the census may sound like an Orwellian device, Ball is more concerned with his characters’ emotional lives than with authoritarian foreboding. The father and son move from region to region, entering strangers’ homes, administering the census. With each new encounter a story from the narrator’s life is revealed. The best of these recall him falling in love with his wife, a renowned clown and performance artist who is also one of the novel’s most dynamic characters. In one lovely scene, prompted by his encounter with two eccentric sisters who conjure the Beales of “Grey Gardens,” the narrator remembers a performance in which giant pieces of silverware, a knife and fork, hovered overhead as his wife and other clowns evaded them. In a novel that ruminates so heavily on death, such memories provide a celebratory sense of joy.
While Ball accomplishes the stated goal of his preface, bringing the son with Down syndrome to life, the census itself leaves a little to be desired. If the narrator aims to hear each citizen’s story, that which is “most particular, most special,” he never shares enough details to make a lasting impression. This creates a kind of flatline with regard to the central conceit. Without more of the particulars, “the small, the overlooked,” it’s hard to understand what the census is meant to measure.
Yet the spare and episodic encounters do take us to some tender places. In one scene, a mother who raised a girl with Down syndrome recognizes the narrator as someone who sees what she sees in their children: “They experience the world just as we do, maybe even in a clearer light.” More than a dystopian tale, “Census” is a profound and stirring meditation on love, loss and paternity.