Dying is taboo among health and care professionals who sometimes prioritise medical initiatives over individuals and families
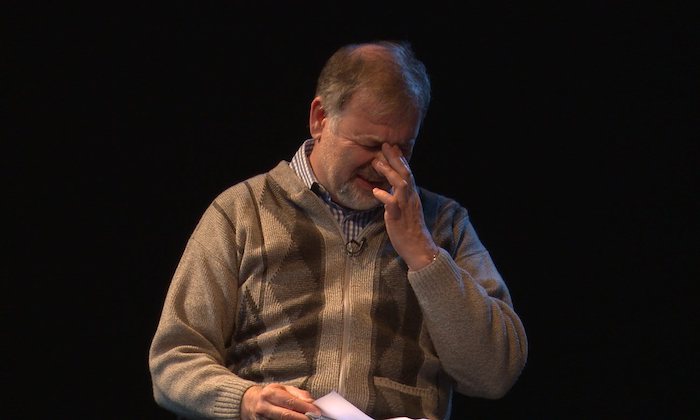
Don’t Leave Me Now, a play about early onset dementia, was performed at St Gemma’s hospice in Leeds to an audience of healthcare professionals.
[S]eth Goodburn seemed fit and well until two weeks before he was diagnosed with pancreatic cancer. He died just 33 days after diagnosis, spending much of that short time in hospital. In the emotional whirlwind of coping with the poor prognosis his wife, Lesley, felt their hopes for Seth’s end-of-life care were sidelined by medical professionals trying to do their job.
“The NHS focuses on the medicine and trying to fix people even when that’s not possible,” she says. “A lot of the conversations and decisions that we might have made were overshadowed by dealing with what was the next medical treatment and intervention.”
There is an ongoing conversation in the medical profession about how to care for terminally ill patients, given that the profession’s instinct is to preserve life. The issue is just one of many being address by Brian Daniels, a playwright commissioned by the National Council for Palliative Care (NCPC) to tell stories such as Goodburn’s through plays, and help educate healthcare professionals about patients and families’ experiences of end-of-life care.
Homeward Bound, a play based on a series of letters Lesley Goodburn wrote, in the months after her husband’s death, to medical professionals involved in his care, launched NCPC’s national conference this year to an audience of 300 healthcare workers.
In addition, Daniels’ plays on early onset dementia and palliative care for those with disabilities, have been performed in hospitals, hospices, care homes and to general audiences across the country. Daniels says: “[They] take people out of their professional role for a minute to look at the family and human side of the people they’re dealing with.”
For Goodburn, that human aspect is key. She could not fault the professionalism of those involved in caring for her husband, but says poor communication could leave the couple feeling worse. “There were just so many things where people weren’t cruel or unkind or deliberately unthinking, but just didn’t really think about what it was like to be me and Seth. He went from being well and living a normal life to suddenly being told that he was dying.” She says, for example, a physiotherapist asked Seth to march on the spot as part of an assessment to see if he was able to go home, as he had previously wished, seemingly unaware that his condition had deteriorated and he was dying.
An actor in Don’t Leave Me Now.
Claire Henry, chief executive of the NCPC, says plays such as Homeward Bound are designed to encourage medical professionals to reflect on the people going through this traumatic process. “We obviously work very closely with people who have experience and they tell us their stories. Some are good, some not so good. Healthcare professionals don’t go to work to do a bad job, but sometimes they don’t think of things that affect people in a broader sense.”
What impact does a play have that a lecture, for instance, cannot? Don’t Leave Me Now, another play by Daniels, about early onset dementia, was performed at St Gemma’s hospice in Leeds to an audience including nurses, housekeeping staff and workers from other local hospices. Dr Mike Stockton, its director of medicine and consultant in palliative medicine, says the play enabled them to see some of families’ and patients’ challenges through a different lens. “It’s sometimes hard to have a full understanding … of what people may be going through and the reasons behind their actions or the emotional challenges, adjustments or the resilience that people need.”
Lynn Cawley agrees. There was barely a dry eye at a performance at Morley Arts Festival in October of Bounce Back Boy, the powerful dramatisation of her adopted son, Josh’s, story. Josh was severely disabled following a serious head injury as a baby, and later adopted by Cawley. Despite pioneering medical treatment throughout Josh’s life, Cawley says he was denied admission as an inpatient to a local hospice because his needs were too complex, and died a difficult death at home. She is fighting to end what she describes as end of life discrimination against those with disabilities.
Cawley thinks a play is an effective way of communicating that message, and for getting people to think about palliative care more broadly. She says: “When it’s someone’s real life story, people put themselves in it [and] they might think of a patient that they know. We hope that it will change policy but also people’s attitudes.”
For Stockton, working in a hospice, the wider issue of how treatment is balanced with patient comfort is a daily consideration. He says the two can often be done together: “It is about having early, thorough, open, honest, transparent conversations with people about what they want.”
For Cawley, as a carer and mother who went through the palliative process, those open conversations about dying are key. “We even find it hard to say the word,” she says. “When we’re watching Casualty on a Saturday night and they’re trying to tell a relative that somebody is dying, but they won’t say the word dying or death, we’re just like – say death!”
Traditionally, the “Day of the Dead” is a time when family and friends gather to remember friends and family members who have died. But it’s also a perfect time to think about your own death – if you dare.
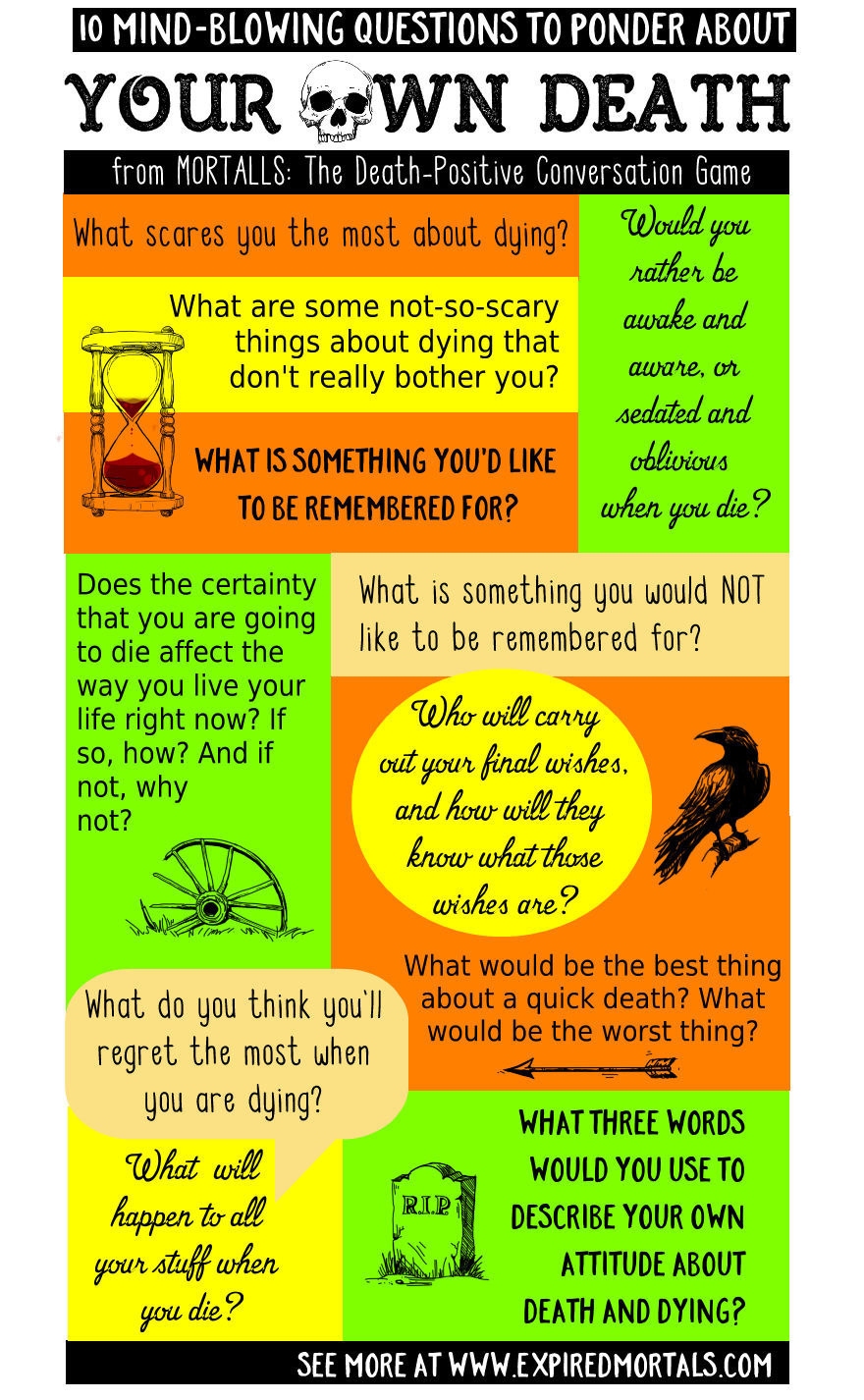
Care to face your own mortality? Here are 10 Mind-Blowing questions to ponder about your own death.
Most people won’t go there because it’s either too scary, too painful, or we just pretend it will never happen to us. But ready or not, there’s a 100% certainty death will eventually get up close and personal with every one of us. Here, from MORTALLS – The Death-Positive Conversation Game, are 10 mind-blowing but worthwhile questions to ponder about your own death… if you are willing to do so:
What scares you the most about dying?
What are some not-so-scary things about dying that don’t really bother you?
When you die, would you rather be awake and aware, or sedated and oblivious? Why?
What would be the best thing about a quick death? The worst thing?
What do you think you will regret the most when you are dying?
What is something you want to be remembered for?
What is something you do not want to be remembered for?
Who will carry out your final wishes when you die? How will they know what those wishes are?
Does the certainty that you are going to die affect the way you live your life right now? If so, how? And if not, why not?
What three words would you use to describe your own attitude about death and dying?
[E]vi Numen, 33, of Philadelphia, could be considered a little death-obsessed. She’s the curator and founder of Thanatography.com, a site that showcases the work of visual artists exploring the themes of death, grief, and loss. Previously, she worked at the Mütter Museum, known for its collection of medical oddities and pathological specimens, such as presidential tumours, murderers’ brains, and books bound in human flesh. She has also recently added a line to her résumé — she’s a “death doula” in training — one of the first in the United States.
Evi Numen
Numen can be excused for being a little morbid. When she was 20, she survived a car accident that killed her partner on impact. Earlier that night, he had told her he was going to propose. While in the hospital recovering from her injuries and raw with grief, she kept asking if she could see his body in the morgue. “I needed to confront his death to truly believe it,” Numen says. “My doctors thought I couldn’t take the sight of him, dead and broken, but to this day I believe it would have helped. Seeing him in his coffin during the funeral a week later felt staged and artificial.”
Last April, when her late partner’s father was in rapid decline with cancer, Numen rushed to his side. “I held his hand, listened, and talked to him when he could, and also allowed his loved ones to take a break from the bedside. What I couldn’t do for my partner, I tried to do for his father.”
A large part of the assistance Numen provided was for his family. “I had to remind them it was okay to take care of their own needs. I couldn’t “fix” anything, but I could bring food so it was there when people needed it, or stay by the bedside and encourage family members to go for a brief walk to get some fresh air.”
Caregivers [of the dying] often need to be ‘given permission’ to care for themselves properly.
After her partner’s father died, Numen knew she had found her new calling. She did some research and found the International End of Life Doula Association (INELDA). “Immediately, I knew this was the right next step,” says Numen. Cofounded by former hospital social worker Henry Fersko-Weiss in February 2015, INELDA trains people to provide emotional support for the dying — and their family members. Ferko-Weiss was inspired by the concept of doulas who support a mother and her partner during pregnancy and childbirth. “I kept seeing people die in ways that I thought were unfortunate or even tragic. I was trying to figure out how to change that. To me, the principles and spirit and techniques of birth doulas could be interpreted and adapted for the end of life,” says Ferko-Weiss.
A certified death doula can help not only the dying person, but will assist their loved ones throughout the entire death process, from coming to terms with mortality weeks or even months before the death to remembering and memorialising their loved one after passing.
Numen took a 22-hour training with INELDA and has logged more than 20 hours of volunteer training at two different area hospices. She’s been coached to become familiar with the physical changes the body goes through directly preceding death — and in helping comfort and counsel the dying person and their family from the point of a terminal-illness diagnosis all the way through even a year after a death. “I think many of us have the tendency to be problem-solvers and try to offer solutions to someone who is hurting, but there is no solution to dying,” Numen says. “It is easy to develop the habit of offering platitudes to such a situation, such as, ‘This too shall pass.” But that’s not actually comforting to a grief-stricken person. I know this from my own experience. Instead, I serve as an active listener, letting the other person really talk about all their conflicting emotions.”
Numen says that one of the most fascinating parts of her training was learning how to recognise when the person is “actively dying.” “Most of us know what the birthing process is like — foetal development, labor, contractions, water breaking, and such are fairly common knowledge in the Western world. Yet very few of us know anything about what it looks like to die: Your appetite decreases, your skin changes colour, breathing sounds different. There is a huge discrepancy in how we view the two ends of human life. It is easy to see how such ignorance about death can lead to avoidance and fear.”
Numan had asked the nurses at a hospice where she was volunteering to call her if they needed someone to keep vigil for an imminently dying patient, especially if their family couldn’t be there. “My objective was to be with the person who needed me the most,” she says. She was called to the bedside of an elderly man in end-stage pulmonary disease. He had no family present and was unable to communicate. She was his sole companion in his final moments. She knew from her training that he only had a few hours of life remaining.
Over the course of seven hours, Numen played Clint Mansell, Erik Satie, Rachmaninoff, and Chopin on her iPad as she sat by the man’s bedside and watched him breathe. “His breath cycles grew further and further apart, but only by seconds, which to me felt like minutes as I found myself holding my breath with him,” says Numeb. “I knew he was very near. Within an hour, his breath got steady but oddly mechanical, more like a reflex than an action, and then the next inhale never came. I called the nurse and she confirmed the death. It was easier and more peaceful than I thought it would be, and yet it affected me more than I expected. I had, after all, trained for this, read about it, and kept vigil to other dying patients, but his passing was the first I had witnessed.”
Despite all her preparation, Numen was so deeply affected by the experience that she had to skip her next scheduled shift. “Being there for that man, when no one from his family was able to, affected me more than I thought it would,” she says. “I didn’t cry — I felt it wasn’t my place to, like I was just a stand-in for his family. There is a weird sense of intruding, especially when keeping vigil for complete strangers, that I have not been able to reconcile yet.” It also had a personal resonance for her. “Witnessing a death brought up the other losses in my life, and I had to honour these emotions before I could return to keeping vigil for someone else,” Numen explains.
Witnessing a death brought up the other losses in my life, and I had to honor these emotions before I could return to keeping vigil for someone else.
Despite her unanticipated reaction, she is even more committed to her calling of caring for the dying than she was before. “It wasn’t gross or scary, but it was certainly difficult. Every death will be different, and maybe it will get easier or less nerve-wracking, but it will not get any less worthwhile. Even if I never get to talk with the patients I attend to, knowing that I brought some small amount of comfort is enough.”
She’d also like to see more people become comfortable with ageing and the dying process. In a culture where ageism is rampant, Numen has found that learning about the end of life has actually made her less apprehensive of getting older — and the inevitable end. “Most of the patients I’ve seen close to death were peaceful and tranquil. They seemed comfortable and had this beautiful glow about them, this serenity that I didn’t expect to see. I’m still fearful of sudden death and the suffering of prolonged illness, but not of the dying itself.”
Numen also hopes that more family members will recognise that a death doula can be an option that can bring enormous comfort in someone’s final moments. “It’s about regaining control over an uncontrollable process,” she says.
“I could see that they were slowly leaving the sphere of TV commercial old age… and moving into the part of old age that was scarier, harder to talk about, and not part of this culture.”
– Roz Chast, “Can’t We Talk about Something More Pleasant?”
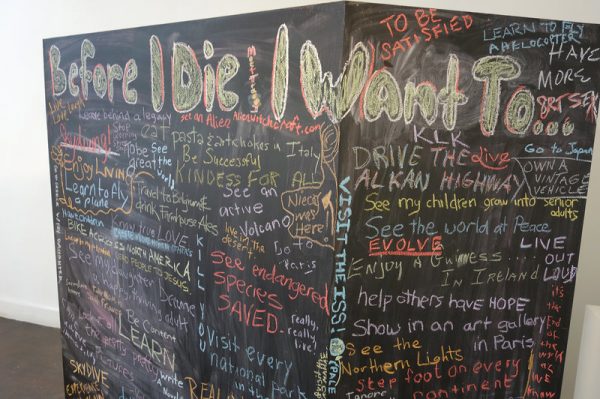
A chalkboard “bucket list” stirred imaginations and got people talking at an Indianapolis festival designed to help make conversations about death easier.
It’s a topic we avoid at all costs: the inevitable descent each person makes from that American ideal of youthful independence to frailty and death. Fearful of following that path ourselves, we resist discussing it – even as loved ones venture closer to that inescapable end.
In recent decades, American culture has opened to permit candid conversations about many topics once off the table – from gender identity and racism to addictions and disorders. But when it comes to end-of-life discussions, there’s still strong resistance. Those who seek to live sustainably can find that challenge enough, without facing what it might mean to die with integrity.
Many societal undercurrents reinforce our resistance. With urbanization, ties to the natural world have grown tenuous and we witness the life-death cycle less frequently. When we do, it’s often on screen – far removed from our daily reality.
Countries like Mexico and Poland hold collective rituals that help normalize the inevitability of death, but Americans prefer Memorial Day picnics, parades and summer-season sales. Our commercial culture worships youth and novelty, while portraying old age as a protracted talk with your doctor about pharmaceuticals.
Advances in medicine lend hope that we might keep death at bay, an illusion many doctors reinforce. “Our decision making in medicine has failed so spectacularly,” surgeon Atul Gawande writes in Being Mortal, “that we have reached the point of actively inflicting harm on patients rather than confronting the subject of mortality.”
Our cultural resistance to discuss life’s end causes widespread suffering for the dying, depriving them of what Gawande calls the right “to end their stories on their own terms.” Pressured both by medical personnel and by family members, patients can spend their final weeks in Intensive Care Units, swathed in tubes and surrounded by strangers. Even though 80 percent of Americans would prefer to die at home, only about 20 percent today do.
Denying dying people the chance to take what control they can has far-reaching repercussions for family members – who can struggle for years with the death’s emotional, spiritual and financial aftershocks. Many of them experience a sense of lingering regret over lost opportunities for connection in the final days, and some cope with debilitating medical bills. A quarter of households in one study had medical expenses in the five years before a member’s death that exceeded their total household assets.
Costly late-life medical interventions drive up health care costs, straining the budgets of families, businesses and government. Roughly 30 percent of all Medicare expenditures go to the 5 percent of patients in their last year of life.
We cannot afford to continue along this path; it is not sustainable by any measure.
Fortunately, the culture is starting to shift – aided by Gawande’s book and resources like The Conversation Project and Death over Dinner. These efforts address the gap between the 90 percent of Americans who acknowledge they should have end-of-life discussions and the meager third who do.
Columnist and author Ellen Goodman was among those who launched The Conversation Project in 2012 after realizing she’d never had those crucial value discussions with her own mother while there was time. People postpone these talks, Goodman told me, “feeling it’s ‘too soon.’ What we’ve learned is it’s always too soon until it’s too late.” The opportunity is lost once someone lands in the Emergency Room, ICU or Alzheimer’s care facility.
People envision end-of-life talks primarily with elderly parents, but they should occur among all adults. Despite initial reservations, many people find that these dialogues lead to warm exchanges and what Goodman calls the sharing of “deep family stories.”
Even in close-knit families, the responses of loved ones may come as a surprise. People often express desires “besides simply prolonging their lives,” Gawande writes, prioritizing concerns like avoiding suffering, bonding with family and friends, and remaining mentally alert. Contemplating the end of life can help us clarify what matters most – not just when time becomes short, but every day.
Ideally, these heartfelt exchanges lead to completing paperwork that can help guide family members and medical practitioners. The Conversation Project recommends that individuals authorize a medical decision-maker; complete an Advanced Health Care Directive (templates can be found online), and discuss end-of-life wishes with their health care provider. Medicare recently began compensating doctors for time spent having these discussions. Those who are at a late-life stage may also wish to complete and post a Do Not Resuscitate (DNR) form.
One of the many benefits to initiating these dialogues early, Goodman notes, is that it can help family members agree to back the patient’s wishes. Absent that consensus, relatives can unwittingly make the process harder for a dying person through their own resistance to letting go. Roz Chast captures this poignant dynamic in her graphic memoir, portraying how her mother – facing her husband’s impending death – challenged the “defeatist attitude” of hospice and asserted “I told Daddy he was coming with me to 100 if I had to drag him kicking and screaming!”
The prospect of death – whether our own or that of a loved one – is inescapably fraught with fears and uncertainties. It’s easy to see how we’ve drifted into a kind of denial, and slipped into medically managing the end of life despite crippling personal and societal costs.
We owe it to ourselves and each other, though, to discuss what matters most in our waning days. Having that dialogue with loved ones could help us remain authors of our lives through the closing chapters.
[M]y mother once told me a very sweet story about how I, as a toddler, handled my grandmother’s death. After the funeral, my mom asked me if I knew where Grandma had gone. I told her, as matter-of-factly as a 2-year-old could, that she was in a garden, surrounded by daisies (her favorite flower).
Even at such a young age, I’d developed a sense for the appropriate kinds of euphemisms for death — and I knew that sharing them would bring comfort to my mom. But that didn’t change the fact that my grandmother was dead — like, she was dead and buried and there weren’t any daisies in there with her, though I didn’t quite comprehend that yet.
It was actually much later, when I was 17 and attending another relative’s funeral, that the reality of death truly hit me. My uncle had died after being diagnosed with cancer way too late, and his passing was a real shock to the family. The memorial service was at his house in Virginia and the choir from his church sang some upbeat hymn about going where you were always meant to go. Listening to that, and knowing how he died, I thought, This must be a joke.
I bristled at the idea that dead people were anything other than dead. On one hand, I found it naive to think about death in such rosy terms, inwardly rolling my eyes at those who did. On the other, I believed that death was supposed to be frightening, and by rejecting the idea of an afterlife or deliverance I all but cemented that fear in my mind.
In other words, I gave myself two options: I could scoff at death or fear it wholeheartedly. Multitasker that I am, I decided I could do both.
I found myself viewing death as two very different (and equally problematic) beasts — a hulking, dark thing that we only discuss in whispers and a lurking shadow that simply absorbs the rueful jokes we hurl at it.
Neither of these images get death quite right, but there I remained, with death constantly on the brain. For fear of seeming morbid or like a total downer, I kept most of my thoughts about death and dying to myself. Yet, a question nagged at me — Was I alone in feeling this way?
The urgency of that question has only increased over the course of this year. That’s why, this fall, R29 conducted an informal survey about death, to which more than 300 people, mostly millennial women, responded.
Nearly half of all respondents said they learned about death by the time they were 5 years old, citing such sources as dead pets, 9/11, Mufasa, and, like myself, the death of a loved one. They grew up believing that the deceased ended up in God’s arms, went to heaven, took on another earthly form, or were left to fade into nothingness.
Regardless of their foundational experiences with death, most people still think about it — and in a small, strange way, I found that comforting. “Ever since turning 30, I think about death every couple hours,” one person wrote. “It’s almost the only thing I think about,” wrote another.
The thing is, most people don’t simply fear death or laugh at it. Instead, people describe how they use death to interrogate their religious beliefs, take stock of their health, and motivate themselves to spend time with distant, elderly loved ones.
Many said they hope they’ll die quickly and at an advanced age. Some alluded to suicide attempts (If you’re experiencing suicidal thoughts, please call the National Suicide Prevention Lifeline at 1-800-273-TALK (8255) or the Suicide Crisis Line at 1-800-784-2433.) or an unshakable conviction that they’ll die young. One person qualified their acceptance of death like this: “I deeply fear dying, but don’t fear death.” In total, 71% admitted to having imagined their own death.
I’ve been turning that number, 71%, over and over in mind my since first seeing it. For one thing, it answers my question: I’m anything but not alone in constantly thinking about death. It also makes me regret that we didn’t ask how many of them ever told anyone about imagining their own death. I wonder how much higher or lower that number would be.
Here’s what I want to tell everyone who thinks about death on the daily: You’re not morbid. You’re human. And you don’t have to keep those thoughts to yourself. After all, chances are, most other people are thinking them, too — and death is neither a beast nor a shadow.
It’s something that informs and gives meaning to how we live. As one person put it: “The more I learn about death, the less I fear it.”
Welcome to Death Week, in which we’ll attempt to unpack our feelings, fears, and hang-ups about death, dying, and mourning. We’ll do our best to leave no gravestone unturned.
While end-of-life doulas, also called death doulas or death midwives, aren’t medical professionals, they can supplement the work of hospice staff by providing ease and comfort to patients and their families.
Doulas have typically assisted women during childbirth, or to support the family after the baby is born. But recently some doulas have shifted their focus to helping dying patients and their families.
Merilynne Rush and Patty Brennan, alternative health professionals, will offer Michigan’s first end-of-life doula training Nov. 18-20 in Ann Arbor. The sessions are geared for family members and friends of the dying, hospice and palliative care workers, midwives and doulas, clergy, therapists, life coaches, and anyone interested in preparing for their own death. It is not recommended for the recently bereaved.
While end-of-life doulas, also called death doulas or death midwives, aren’t medical professionals, they can supplement the work of hospice staff by providing ease and comfort to patients and their families.
Death doulas typically have experienced loss and want to encourage conversations and decision making about dying so patients and families can make their last days and the bereavement process more meaningful.
Each doula’s services are tailored to the specific needs of each patient and his or her family. They can include helping to create a death plan and caring for patients whether in a hospital or at home. Death doulas provide spiritual, emotional and psychological care to patients and their families, and can help plan home vigils and funerals.
Fees for their services also vary widely; some charge per hour, others offer packages for specific services, and some work on a volunteer basis or waive their fees for families who can’t afford their services.
“As more and more of us live longer and face chronic and life-limiting illness, the period of dying has extended from a few days or weeks to months or years,” Rush said. “Medical care focuses solely on cure and treatment. Patients often feel adrift among medical choices while grasping for ways to live with illness in full awareness that death will come. Life choices include acceptance, growth and sharing gifts of love and preparation. There is much meaning to be found during the dying year that is profound and life affirming.”
Deanna Cochran, a former hospice nurse from Austin, Texas, became an end-of-life doula after her mother’s death. She now works with patients who call on her to help them write advanced directives, plan funerals and prepare their family for their passing.
Cochran notes that death is a topic many people continue to feel uncomfortable addressing with their loved ones. Doulas can break the ice and serve as an impartial third party who facilitates conversations about end-of-life wishes.
“I started my private practice to help other families have the same end-of life experience that my mom had,” Cochran said. “My mom didn’t want to die in a hospital. She got to stay in her home with her family and dog and to remain comfortable, despite having an aggressive cancer.”
During the training sessions in Ann Arbor, participants will attend several workshops: assessing the needs of the dying, what is “good death,” how to hold a vigil, hands-on comfort measures, and working with the hospice and palliative care team, as well as doula practice considerations. Day three covers how to have a home funeral, a normal extension of hospice care which brings healing and comfort to friends and family through hands-on involvement in care of the body after death.
The event takes place at the Center for the Childbearing Year, 722 Brooks St. in Ann Arbor. For information and to register, visit center4cby.com.
As a hospice volunteer, I once asked a woman I’d been visiting for several months what she wanted for her upcoming 75th birthday. She was wheelchair-bound, living in a nursing home, and in the last stages of metastatic breast cancer.
“Life,” was her answer.
Life. Of course. We all want to live as well and as long as we can. Eventually, though, our bodies betray us and we begin to show the telltale signs of aging. And, as we age, we have to reconsider and accept who we are now, and think seriously about how we want to live throughout our last chapters.
No one wants to think about the prospect of death. But as we lurch into old age, we are faced with the prospect that many of us will need what our medical system does not currently provide: high-quality end-of-life care. It’s more than a personal concern; it’s a pressing societal issue. Projections are that, by 2030, one-fifth of the population will be 65 and older, compared to 13 percent in 2015, and 9 million people will be over 85.
Currently, our country’s end-of-life care is fragmented, costly, and unsustainable. Too much aggressive care is given that is futile and ruinous to people’s quality of life. Doctors frequently don’t discuss with patients and family what truly matters to them and offer comfort; and those left behind are often wracked by a sense of guilt, haunted by the choices they’ve made in the heat of the moment without really knowing their loved one’s wishes.
Fortunately, there are people, places, and organizations that are taking a serious look at how to improve quality care, and some are making strides in the right direction.
In my book, Last Comforts, I chronicle the current realities of end-of-life care, and point to some of the outstanding pathfinders and innovations in this field that could make a difference for all of us. It’s not just about “brink-of-death” care. It’s about how to better educate doctors and nurses; provide more effective dementia care, design and operate better long-term care facilities, recognize the unique challenges of minority and LGBT people, and provide better training and a living wage for the nursing assistants and home health care aides who do so much of the hands-on care for elders. Ultimately, we need to understand how public policy decisions about palliative and hospice care affect us.
What can we do as individuals? The first, and probably the toughest, task is to look our own mortality squarely in the eye. That’s no easy feat, and certainly not encouraged in our death-denying culture. But if we do, we can be better advocates for ourselves—and our loved ones—and can begin to understand the many choices we will have to face, and take some responsibility for ensuring our wishes are met.
Here are some of the lessons I’ve learned—from my experience as a hospice volunteer, as well as from my research as a reporter—on how people can prepare better for the end of life:
1. Educate yourself about the different key treatments for end-of-life care, so that you can make informed decisions
Before we can talk to our family or friends about what matters to us and what we’d want at the end of our lives, we have to think about it seriously—and get better educated about it.
These are profound questions about the very heart of our lives: If you had a limited amount of time left to live, what would be most important to you? What would make life continue to be worth living? What would you be willing to tolerate, in terms of rigorous and aggressive treatment, in order to achieve a longer life?
That’s the framework for looking into the many tools that hospitals have at their disposal to prolong life, and how those tools may be employed at critical moments. It helps to know in advance what these life-saving procedures actually look like in practice, so you can better assess which, if any, would be acceptable to you, and under what conditions.
If you’ve never had to consider these kinds of aids before, it can be difficult to envision. You may just end up relying on your doctor’s recommendations or, more problematically, movies and TV portrayals, where unrealistic outcomes are the norm.
CPR, advanced life support, intubation, and feeding can be life-saving, particularly when you are young and have an acute condition. But, for the elderly, they can often significantly decrease quality of life without providing much benefit. For example, many doctors will prescribe feeding tubes to patients with dementia, even though it can lead to pneumonia, infections, and ulcers, and may not prolong life much.
To better decide for yourself, it might help to read about these procedures, or to even watch videos that show what the treatments involve, which you can find here.
2. Start conversations with loved ones so that they are clear about your wishes for care
Adult Daughter Talking To Depressed Father At Home
If you’re clear about what you value and how you’d want to be cared for toward the end of your life, don’t keep it a secret! This is the time to have a conversation with your loved ones about what you want—particularly critical guidance for them if you are in a medical crisis and cannot speak for yourself. And bear in mind that this is not a one-time conversation. Your own feelings may change over time, depending on your circumstances, and if they do your loved ones need to know.
Nobody wants to talk about these things. How do you start? Remember when our children were younger and we looked for “teachable moments” to discuss pressing issues? I believe in looking for “teachable moments” for talking about serious illness and end-of-life issues, too. If a friend of the family or the parent of your child’s best friend is going through a medical crisis, for example, it might be a perfect time to turn the conversation to your own family, and your own thoughts and feelings on the matter.
If you need a good prompt, The Conversation Project offers useful “starter kits” to kick off a discussion, including one for those suffering from dementia.
If you cannot speak for yourself in a medical crisis, an advance directive and a designated health care proxy will help to navigate the system more smoothly on your behalf. Choose a health care proxy who not only understands what you want, but is willing and capable of carrying out your wishes. You can find advance directive forms for each state at Caring Connections, a program of the National Hospice and Palliative Care Organization.
3. Understand the benefits of palliative care and hospice care and know when to ask for them
Palliative care is a medical specialty that is available to anyone with a serious illness, whether or not you are dying. Palliative care addresses your symptoms, whether they’re physical, such as pain or nausea, or whether they’re emotional or spiritual. Interdisciplinary teams of caregivers including doctors, nurses, and social workers are dedicated to providing coordinated care that plans your care based on your goals and values. And you can still receive curative care concurrently. Palliative care may or may not lead to hospice care; but it will allow you to decide how you want to be cared for over time as your illness progresses.
Research suggests that palliative care is an important factor in determining how families rate the quality of end-of-life care received by loved ones. In one study, cancer patients who were randomly assigned to receive early palliative care versus standard medical care reported better moods and quality of life throughout treatment, and they lived longer on average, even though they received less aggressive treatments. A recent review of research found that, for oncology patients, early palliative care improves quality of life, “mood, treatment decision-making, health care utilization, advanced care planning, patient satisfaction, and end-of-life care.” It also may improve symptoms and survival.
Hospice care differs from palliative care in that it provides comfort care only if your illness is life-limiting and you have a prognosis of six months or less, and you must forgo any treatments aimed at curing the illness. Hospice care is provided mostly in people’s own homes (and that includes assisted living and nursing facilities), but can also be provided in a hospital, or in a dedicated hospice facility. Though some people avoid hospice because they (mistakenly) believe that it means “giving up,” at least some research suggests that hospice patients are more likely to live as long (or longer) than terminally ill patients in hospitals.
Both of these services can make a tremendous difference in the experience of facing a terminal illness. Just having a say in one’s care and knowing that medical staff and loved ones understand your wishes can be a huge relief.
4. Learn how to communicate effectively with doctors and medical staff
Many doctors are far better at the art and science of medicine than they are at actually communicating with patients. And yet, if you have a serious illness and have to make informed decisions about your care, you want someone to communicate your choices, the risks and benefits of treatment, and the pros and cons of different options, as clearly as possible. Your doctor should be comfortable talking to you about end-of-life wishes in an honest, meaningful way, and listen, show empathy, and encourage questions. Research has shown that patient satisfaction goes up when doctors employ these types of skills, and they can have an impact on outcomes as well.
Be prepared to ask questions about recommended medications or surgeries and their side effects, alternative therapies, and the anticipated outcomes of treatment versus no treatment. Too often we leave the office without this vital information and end up making decisions for expensive and futile treatments that do little to prolong life and can have serious consequences on the quality of the life left to us.
It’s often helpful to bring along a supportive family member or friend to a doctor’s appointment to take notes; or, if that’s not possible, to record your conversations with your doctor. That way, if you receive bad news and find yourself overwhelmed with emotion, you’ll have the important information written down or recorded to refer to later once you’re feeling calmer.
5. Research nursing and assisted living facilities in your community, in case you need them
I’d bet that nobody ever thinks, “Gee, when I get older, I really want to go live in a nursing home.” We’d prefer to remain independent and age in place in our own homes. And, indeed, more options are becoming available for that to happen. This is encouraging, since reports suggest that aging in place can have emotional and health benefits for those who can manage it.
But, for some of us, end-of-life care may involve assisted living or nursing home care, especially if we live long into old age. Not all of us will have supportive family and friends available to care for us if we need help. Many do not have adult children; or have adult children who live too far away to provide daily care. Luckily, there are some innovative long-term care developments that offer patient-centered care. That means that you spend your day according to your schedule, not an institution’s: rising, dining, dressing, and participating in activities as you choose. Moreover, there’s much to be said about living with others in a setting that can combat the loneliness and isolation that afflict so many elders living alone and that contribute to poor health.
You can learn more about culture change and patient-centered care in long-term care settings from two organizations, The Pioneer Network and LeadingAge. The Pioneer Network offers a list of excellent questions to ask if you’re considering a move to assisted living. You can also compare quality of care in a nursing home by checking Medicare’s Nursing Home Compare website, and looking at their guidebook for how to assess staffing, operations, and care at a nursing home.
6. Advocate for better end-of-life care for everyone
This essay is adapted from Last Comforts (Cypress Publishing, 2016, 350 pages)
In addition to planning for our own care, I can’t emphasize enough how important it is to advocate for everyone. Our current system is plainly unsustainable. I believe that for aging baby boomers, it’s time to tap back into our activist genes and address the many intertwined social and medical issues involved in end-of-life care.
The very foundation of how society pays for palliative care should be rethought and adjusted to respond better to the way people really die now (as opposed to how they died in the ‘70s, when hospice began). The way we deal with multiple cultures and differences in sexual and gender orientation has to become more sensitive. The way we design and operate long-term care facilities has to change to better enhance the dignity and quality of life of their residents. The way we train and compensate direct care workers, such as certified nursing assistants and home health aides, needs to reflect the growing importance of their role. The way public policy addresses medical care but not the critically important element of non-medical support for the very frail has to change, too.
In the medical realm, we can support initiatives aimed at compensating professionals who go into palliative care fields. It’s still too often the case that tests, procedures, and treatments are reimbursed at a higher rate than are the compassionate discussions with patients and their families that are the heart of good end-of-life care.
We must do all what we can to arm ourselves with knowledge, to communicate clearly with others about our wishes, and to advocate for quality end-of-life care. Our lives, literally, depend on it.