Hospice care provides a team of physicians, nurses and other professionals to help manage the spiritual and emotional aspects of end-of-life care.
By Melisa Rile
Renee Beccue
Renee Beccue helps ease the process of dying.
She is an on-call registered nurse with Lower Cape Fear Hospice in Wilmington. Beccue, originally from Buffalo, N.Y., had primarily worked in intensive care units with burn patients.
She had accompanied doctors when they announced deaths of patients to their families and saw that this experience could allow her to transition into hospice nursing.
“Hospice and palliative care is a growing field,” said Beccue.
Part of what hospice care provides, is in-home equipment for patients, such as hospital beds, so they can spend their last days in the comfort of their own home. There is also a team of physicians, nurses and other professionals to help manage the spiritual and emotional aspects of end-of-life care.
And while hospice doesn’t provide in-home, around-the-clock medical care, it does have providers on call to help manage medical needs.
That’s where Beccue comes in.
Beccue doesn’t have a fixed caseload of patients, but she receives calls at night when hospice patients are in need of medical care that the family or caregiver feels is outside their capability. Beccue travels to a few counties for on-call needs, including Onslow and Pender as well as New Hanover.
The calls she receives can be anything from discussing fall prevention to pronouncement of death. Part of the medical care received in home is to help the patient remain in the home with fewer trips to the hospital.
“We try to prevent readmission to the hospital,” Beccue said.
Her care as a hospice nurse is twofold, therapeutic listening and education. Education consists of teaching the family or caregivers the basics of caring for a sick person who will continue to decline. Beccue calls this the “palliative care mindset, not curative.”
She teaches the family to change the bed and bathe the patient while he is still in the bed. Beccue says the care needs of hospice patients are constantly changing because they continue to get sicker. She also teaches the family what they can expect to see from the patient depending upon his disease.
Beccue also helps patients understand what they are experiencing. She consoles them and emphasizes the importance of “judgment-free” care as a hospice provider. Beccue realizes that many people are not familiar with the medical terms being used and she sincerely tells families and patients to call her with any questions.
Beccue primarily tends to the patients’ medical needs, but in the process of dying, people often work through a life review. Many patients do not truly grasp their prognosis for a variety of reasons until Beccue arrives at their home. She sometimes helps patients face the truth that she has been assigned to them because they have a prognosis of six months or less left to live.
“That’s when they cry,” Beccue said.
She tries to be the voice of reason and help them to understand that the feelings they are experiencing are normal. She can assist with adjusting medication when anxiety is overwhelming and to help mitigate physical pain.
Beccue says it’s important to allow patients to feel. “You can’t make a stage 4 diagnosis nice,” Beccue said.
She has seen patients move through bitterness, anger and unresolved issues and hospice does provide social workers to help counsel the patient through that process.
While death is frightening for many people, Beccue sees it as a part of living. And death isn’t all scary and sad. Many times she turns on music for patients, helps them sit by their favorite window and watch the birds they’ve enjoyed their whole lives. Also, the presence of beloved pets is important to comforting patients.
Some patients want to sit and look at the garden they worked in for years. Beccue says one patient asked to sit by the window and watch the golf course every day.
After years of being with hospice patients Beccue has learned a few tips about working with the dying. She recommends being upfront and honest about prognosis, allowing honest feelings about that prognosis and ultimately finding peace and joy in death, which is the ultimate rite of passage for all of us.
Most of us won’t get any say in how or when we die. But even knowing that, the question of what makes a good death feels important, even urgent. What is the best that we can realistically hope for, at the end? If you subscribe to an organised religion, you might focus on living virtuously in the hope of a posthumous reward. The rest of us need to know how to go about dying with some dignity and grace, amid the grubby imperfection of the real world. The Australian writer Cory Taylor managed it, and she has left us her wisdom and experience in this book, which is part memoir, part critical examination of western society’s dysfunctional relationship with mortality.
Taylor was 60 when she was told that what had started off as a melanoma was now incurable cancer. She had already witnessed the reality of “dying badly”: both her parents died in nursing homes after long and humiliating descents into dementia. The last time Taylor saw her mother, she watched as a nurse changed her nappy. “The look in my mother’s eyes as she turned and saw me,” she writes, “reminded me of an animal in unspeakable torment.” Taylor’s one comforting thought when she received her own terminal diagnosis was that she wouldn’t have to go like that: she had the time, and the mental capacity, to find her way towards a better death.
En route, she became something of an ambassador for the dying. When she first found herself in a ward of terminally ill people, it was as if she “had stumbled out of a land of make-believe into the realm of the real”. Death, she realised, was the great unmentionable; a “monstrous silence” that left those facing it lonelier then ever. There was very little help on offer to a non-religious person who wanted to die well. Why, she found herself wondering, do doctors avoid talking about death with their patients? Why is there so much funding for hugely expensive cancer treatments, even when they are ineffective, and so little for research into palliative care and support? And why have we allowed the debate about assisted dying to be dominated by religious groups?
Taylor was tempted by assisted dying. After several almost comically unhelpful interactions with medical professionals (her family doctor, referring her for counselling, wouldn’t describe her problem as “dying” but rather as “adjustment disorder”), she joined Dignitas and Exit International. She even got as far as ordering a euthanasia drug from China. But though the knowledge that she could end it herself was important to her, she couldn’t actually do it. In the absence of a supportive legal system, she would have had to take the drug alone, and she worried about the impact on her loved ones and the people who found her. She didn’t want the word “suicide”, with its connotations of mental turmoil and despair, on her death certificate.
“It surprises me that I have any qualms at all,” she writes of that decision, “since I have never thought of myself as a person of particularly high moral standards.” Along with the precision of her writing, it is Taylor’s lack of self-righteousness that lends this book its very special quality. She doesn’t embark on a “spiritual journey”, set herself up as any kind of guru, or even offer answers as such. There is no phoney narrative of redemption – indeed, much of the narrative is devoted to exploring rifts in her family which remained irreconcilable to the end. There was a depressed grandmother, and a property dispute in her mother’s generation; then her mother and father divorced after many miserable years in which he dragged his family around the world on a series of wild goose chases. Taylor was estranged from her father when he died, and she wasn’t on particularly good terms with her siblings. “A different family might have managed to put all this history behind them,” she writes; hers did not.
In the absence of happiness ever after, we are bound to hope for some sense of resolution. Taylor, for whom writing was an obsession since childhood, focuses on remembering the experiences that shaped her character, and finding the right words to describe them. She is sparing about what she includes, but each scene has a luminous quality, a little like her description of the light in Fiji, where she lived briefly as a child: “so pure that it infused every object with an extra intensity, so that a flower was not just red, or a blade of grass just green.” We see the moment in which she first recognised desire (in the eyes of her mother, meeting a handsome Texan), and her first intimation of mortality, watching a kookaburra swoop down from a branch to kill a skink. We see her going to buy her Fijian school uniform, “pink, mint-green … open-weave cotton with its delicious sugary smell”.
She seems to say that our lives, in all their glorious messiness, are their own reward. “The accident of birth is just that. And so is everything that happens afterwards, or so it seems to me.”
Taylor died in July, shortly after this book was published in Australia, and there is no end note to tell us whether her desire for a good death was rewarded. Naturally, I googled it: she died peacefully, surrounded by her family. Somehow I knew that would have been the case. But then again, perhaps she just got lucky.
Supporters of “death with dignity” have succeeded in legalizing medical aid-in-dying in five states by convincing voters, lawmakers and courts that terminally ill patients have the right to die without suffering intractable pain in their final days or weeks.
When Gov. Jerry Brown signed California’s law in 2015, he said: “I do not know what I would do if I were dying in prolonged and excruciating pain” and that it would be a “comfort to consider the options afforded by this bill.”
Yet the latest research shows that terminally ill patients who seek out aid-in-dying aren’t primarily concerned about pain. Those who’ve actually used these laws thus far have been far more concerned about controlling the way they exit the world than controlling pain.
The research suggests that patients’ motivations are more complicated than they’re often portrayed and could affect or shape how people vote on the issue in other cities and states.
Colorado voters will decide on a ballot initiative to legalize physician aid-in-dying in November. The city council in Washington, D.C., voted to legalize the practice this month, though a final vote must still be held.
“It’s almost never about pain,” said Lonny Shavelson, a Berkeley, Calif., physician who specializes in the care of the terminally ill and who began writing prescriptions for lethal doses of medication in June, when California’s law took effect. “It’s about dignity and control.”
Pain ranks near the bottom of a list of patients’ concerns in Oregon (PDF) and Washington (PDF), the first two states to legalize physician-assisted dying, which provide the most complete details about people’s motivations. Only 25 percent of the 991 Oregon patients who died after taking lethal prescriptions from 1998 to 2015 were concerned about pain or had inadequate pain control, according to reports filed with the state by their doctors. In Washington, 36 percent of 917 who died were concerned about pain.
In contrast, at least 90 percent of patients in both states were motivated by a loss of autonomy, state records show. Forty-one percent of patients in Oregon and 53 percent in Washington said they feared burdening the people they loved. Montana, Vermont and California also permit aid-in-dying, but haven’t released detailed information about patients’ motivations.
Seeking Control
Compassion & Choices, an advocacy group that supports aid-in-dying, focuses heavily on the need to relieve dying patients of pain.
One of the group’s new ads promotes the District of Columbia’s Death With Dignity Act as giving “a dying person the option to avoid the worst pain and suffering at the end of life.” The widower of Brittany Maynard, a 29-year-old California woman who became the best-known advocate for the right to die, has spoken publicly in support of the legislation. Maynard, who had an aggressive brain tumor, moved to Oregon in 2014 in order to use that state’s aid-in-dying law. She died that year after using a lethal prescription.
“The dying process is what Brittany feared,” said her husband, Dan Diaz. “She was afraid that her final few days on this green earth would be ones where she was tortured by the tumor.”
Mary Klein, a 68-year-old resident of the District who is fighting advanced ovarian cancer, said she wants choices at the end of her life.
“I want to have the option to control my own body and control my own life,” said Klein, a retired journalist and artist who appears in a video supporting legislation to legalize aid-in-dying in the city, created by Compassion & Choices.
Although Klein says she may also enroll in hospice care, which focuses on the needs of people with six months or less to live, she wants to have an alternative if the services don’t meet her needs.
“The dominant reasons for wanting euthanasia or assisted suicide are psychological and involve control factors,” said Ezekiel Emanuel, chair of medical ethics and health policy at the University of Pennsylvania. He noted that most of those who’ve used aid-in-dying laws are white, well-insured and college educated. “These are people who are used to controlling every aspect of their lives, and they want to control this aspect of their lives.”
A study of 56 Oregon patients interested in physician aid-in-dying reached similar conclusions. Although patients were concerned about the risk of future pain, they ranked “current pain” as unimportant, according to the 2009 study in Archives of Internal Medicine (now known as JAMA Internal Medicine). Patients told researchers they were primarily motivated by a desire to “control the circumstances of death and die at home,” as well as a loss of independence, poor quality of life and their inability to care for themselves.
The patients interviewed “look forward to this period in their terminal illness, this time in which they will be not in control, when they will be dependent on others, when they will have a bunch of physical symptoms that will undermine their quality of life, and they want to avoid that,” said Linda Ganzini, a professor of psychiatry and medicine at Oregon Health & Science University.
Critics of aid-in-dying laws have for years warned that they could set the country on a “slippery slope,” in which lethal prescriptions are dispensed not just to the terminally ill, but to anyone with a disease that harms their quality of life. Those fears haven’t come to pass. But physician Ira Byock, who specializes in palliative care, said aid-in-dying laws are creating a slope of another kind. Instead of helping only terminally ill patients in physical pain, they’re being used by patients in psychological distress.
“It’s a bait and switch,” said Byock, executive director and chief medical officer for the Institute for Human Caring of Providence Health and Services, based in Torrance, Calif. “We’re actually helping people hasten their deaths because of existential suffering. That’s chilling to me.”
Although right-to-die campaigns suggest that excruciating pain is often unavoidable, Byock said that “we can relieve the suffering of almost everyone that we care for if we have the time to prepare.”
Hospice staff are on call 24 hours a day to help patients in pain, Byock said. Palliative care and hospice teams also can train family caregivers how to administer emergency pain medications that take effect before nurses can arrive.
Hospice may have alleviated some patients’ concerns, said physician Thomas Smith, director of palliative medicine at Johns Hopkins Medicine in Baltimore. Just 64 percent of Oregon patients and 82 percent of Washington patients last year actually used the lethal medications they were prescribed. Others died without taking them.
“Many people who have the prescriptions don’t use them,” Smith said. “That suggests to me that some people find meaning and purpose and adequate symptom control, not just that they are too weak to take the pills.”
Many Kinds Of Suffering
Barbara Coombs Lee, president of Compassion & Choices, said it’s difficult for people to predict how they will feel as they face a deadly illness. While a healthy person might not imagine being able to tolerate physical disability, people facing the prospect of an early death are often willing to accept harsh treatments or a reduced quality of life in exchange for more time.
That change in perspective could help explain why some of those who advocate for the right to die, including those who obtain lethal prescriptions, never actually choose to hasten their death, Coombs Lee said. But she said that having the prescription on hand can ease patients’ anxiety and give them peace of mind, because they can control the timing and method of death.
Coombs Lee also notes that people can suffer in many ways beyond physical pain. Maynard’s brain tumor caused her to suffer frequent seizures, for example. Coombs Lee also described the case of a dying woman who took a lethal prescription after she began leaking fecal matter, which prevented her from ever feeling clean.
Coombs Lee quotes the woman, Penny Schleuter, in her book, “Compassion in Dying: Stories of Dignity and Choice.” Schleuter said the pain from her cancer could be controlled. But, she added, “I like doing things for myself, and the idea of having somebody take care of me like I am a little 2-month-old baby is just absolutely repulsive. It’s more painful than any of the pain from the cancer.”
Coombs Lee said, “everyone who is terminally ill has some kind of nightmare that would be worse than death to them. They want to achieve sufficient control to avoid that nightmare for their family.”
Dan Diaz said people shouldn’t underestimate how devastating it can be to lose one’s autonomy.
“If I find myself in a situation where I can’t go to the bathroom on my own, where someone has to change my diapers, where I can’t feed myself, where I can’t care for the people around me, where other people have to move me around to keep me from having bed sores, I would then submit, is that really living?” Diaz asked.
Some people who pursue physician-assisted death “don’t want to be in a hospital, don’t want to be connected to tubes,” Coombs Lee said. “They say, ‘I want to be at home with those I love. I don’t want to be delirious or unconscious at the end of life.’ Those are all things that play into their fears about what their disease might descend into.”
Donna Kaufman (left) and Monica Bhargava in “Extremis,” a documentary on end-of-life care.
[T]oo often, we put off the discussion. It’s too uncomfortable.
Then, suddenly, a parent or spouse is in the emergency room, and the doctors need to know: The outlook is bleak. How aggressive should they be in their treatment? What would your loved one want?
In September, Netflix released a documentary, Extremis, that aimed to bring the issue to a wide audience.
It struck a chord with Meredith MacKenzie, an assistant professor at the Villanova University College of Nursing, who specializes in end-of-life health-care issue. She recently spoke to us about it.
You watched the film. Was it good? It was a good representation of just what these conversations look like in the intensive-care unit, or in a hospital setting in general.
I think most people think they are either going to be walking down the street one day and have a massive heart attack and keel over and die, or they are going to go to sleep one night and never wake up. Here’s the problem with that: Especially among older Americans, a very, very small number are going to die suddenly. Most are going to die in a longer, more drawn out process. You’re going to get sick, but it won’t be clearly obvious that you’re going to die right away. You’ll have this gradual decline. Over half of Americans will die in the hospital setting. Among those 65 and older, more than a fifth will die in the ICU.
But ICUs and hospitals in general are not good places for decision making. They are really crowded, really noisy. Alarms are going off. Machines are beeping. Carts are being wheeled by in the hallway. You’ve got nurses and doctors coming in and out. People need to start thinking about this before getting to the hospital, before the ICU.
The film showed how everyone struggles with this. One physician said, “Your mother is unlikely to wake up. Even if she does wake up, it is not going to be a great quality of life.” Those conversations are hard. They’re hard for families. They’re hard for doctors. They’re hard for nurses. And they’re hard for patients.
Let’s talk about the families. As the film was closing, we heard the endings of the patient. But we never heard the ending for the loved ones, the family. My research is focused on family caregivers because they are the survivors of end-of-life care. How end-of-life care went has profound effects for a family. The likelihood of depression, suicide, guilt over what happened, it all hinges on what happened those last few weeks or days of life.
Family members in the ICU are terrified they are going to make the wrong decision. They have to keep living and think about the decisions they made, in some cases agonize over the decisions they made. Sometimes, they opt to do everything because they are afraid they are going to have to live with “Did I kill my mom? Would a miracle have happened?” Or, on the flip side, I’ve had family members who have done everything and then say, “I feel like at the end that we were torturing her.” That is a lot to live with.
What about your own journey through this? I started out in the ER. I did not want to research end-of-life. My job was to save people’s lives. But I really struggled with seeing patients for whom we went to extreme measures to “save their lives.” I will never forget my first code in the ER. The patient was brought in by ambulance. We worked the code for 45 minutes and finally got a heartbeat back. And we were all celebrating. But I remember having this sinking feeling: He had been unconscious for so long. He was in the ICU for six days and ended up dying without ever regaining consciousness. I remember thinking: Did we do the right thing? He had tubes down his throat, multiple lines in his veins, a catheter, a feeding tube. He was on a ventilator. We had also done chest compression, so his ribs were broken, his chest was bruised, his face was bruised. I don’t know that we did the right thing.
Now, I work with a lot of older adults, many with heart failure, which is a really common diagnosis. One in five will die in a year. I start the conversation by asking them, “What is the most important thing in life? How do you spend your day? If you could not do that, would life still be worth it to you?”
I had one older gentleman who spent most of his time sitting at the kitchen table, drinking tea, chatting with his wife, seeing children and grandchildren or neighbors. This was very important to him. I said to him, “You are going to get sicker. I want to talk about at what point might you say you don’t want to go to the hospital anymore?” He said, “I don’t know that I do. I hate the hospital. I never get sleep. They limit visits.” So I said we could talk about other alternatives.
He lived a good three years, a little longer. And he passed away with hospice at home. In his last six months, he had a couple episodes that we managed, symptom-wise. He ended up with, as far as deaths go, a pretty good death. He was able to talk with family and hang out at the kitchen table up to the end.
So, more people should have advance directives and living wills? For the last 20 years, we have been on a major kick to get people to complete advance directives. We have done a semi-good job. Among Americans 65 and older, about 45 percent have completed advance directives. That’s the good news.
But there have been a couple interesting studies showing that even among people who have completed advance directives, if you ask them if they have shared it with their primary care provider? No. Have you talked about it with your family? Well, no. There is a big difference between having that piece of paper and anyone else knowing about it.
The second challenge is that most advance directives, including the Pennsylvania official form, have wording that says “if you are in a state of permanent unconsciousness . . .” Here’s the thing: When does your health-care provider know you’re in a permanent unconscious state? Families say to me, “Is our mom ever going to wake up?” I can give them some percentages. Can I ever say with absolute certainty this person is never going to wake up? Until they’re dead, that’s a tough call.
This has all been rather grim. Any encouraging words? It is true that over half of Americans die in the hospital. But there’s the other almost half who die at home, who die in an assisted-living facility. I think what people need to know is that it is possible to have a meaningful, peaceful, symptom-controlled death outside the hospital. It is possible to give yourself the time you need to say the things you need to say and to have the experience you might want to have. For patients who opt for hospice, they actually live longer than patients who decide to have aggressive care. It’s one of the odder things of life.
It’s not about letting someone die. It’s about acknowledging that death is inevitable. No one can cheat death forever, but we can have some say in how it happens.
One of the most important things is, talk to your loved ones. Talk about what is meaningful in your life. Talk about what you might want, what you might not want. Watch that film and think about, if I was in the ICU, would I want a breathing tube? If you have a chronic illness, at what point would you say, “I might not want to pursue aggressive care”?
It’s hard to think about this when you’re healthy. But that is the time to do it. No matter how uncomfortable talking about dying is, dying without talking about it is more uncomfortable. Think about it as a gift you give to people who have to make those decisions.
Keely Dowton (right) and her mother who died last year.
[D]uring this time of the year death appears in a guise of make up, costumes and candied treats. Often portrayed by colourful eccentric images, celebrations such as Halloween and the Day of the Dead were traditionally about remembering the dead and the memories of lost loved ones.
But talking about death is not easy if you’re British. When broached, the topic seems to make people feel uncomfortable and can even be judged as a morbid conversation subject. But death is part and parcel of what it means to live. We talk about having the ‘time of our lives’ or ‘living life to the full’ but often try and forget what inevitably follows.
We wanted to talk more about death so asked readers for their experiences of grieving and what death means to them. Here’s what some of them said.
‘Grief is so overpowering – it consumes you’
Having lost my mother 17 months ago the experience of losing her is still very raw for me. Mum went to her doctor with a minor stomach upset and died four weeks later with an aggressive bowel tumour. She had no previous symptoms and wasn’t even unwell. It came as a complete shock with total devastation to her family.
Grief is so overpowering – it consumes you. First the numbness and autopilot mode then the heaviness of despair, then the oceans of tears, then the questions of the pointless, futility of life. Then anger, then deep despair, then numbness and repeat. Repeat. 17 months on and I still question all of it; but I cope by leaning on my loved ones and I cope by using my mum’s strength to spur me on. Ironically, she is the one that gets me out of bed in the mornings.
My life has changed drastically. After mum died I resigned from my job, married my partner of 22 years (we married on mum’s birthday as a gift/gesture to her), I got a dog and am now planning a move with my husband to Sri Lanka for a few years. I see my life in two parts; my old life with mum and my new life; one I didn’t want or choose but one that I’m trying to embrace. I try to live my life as my mum wanted; with gusto and enjoying the little things. I’m trying at least.
Keely Dowton, 44-year-old teacher living in Essex
‘I said ‘Good morning’ to a photo of him each day’
I lost my father seven years ago. It was totally unexpected and at the time I could not deal with it. I said ‘Good morning’ to a photo of him each day as I did in person before. I threw myself into planning the funeral, keeping busy meant not thinking about what had happened.
Just after he passed away, I noticed a robin that would watch me when I was gardening. The robin visited the garden most days and would look towards the house. There are some people who think that symbolises that a loved one who has passed is okay. That brought me some comfort even if I don’t completely believe it. I like seeing robins in the garden, even when they are being fiercely territorial. Seeing them is associated with my dad now. I talked about my dad in the present tense for a long time, maybe a year after he had died. Even now it feels incorrect to talk about him in the past because he lives on in my heart and mind. He always will. That’s love.
Anonymous, 39-year-old teacher living in the Midlands
Joanne and her husband
‘Dealing with death is relatively easy compared to getting on with life without them’
Death means my husband. It is something I’m familiar with now as I have lived through his. I lay with his dead body for half an hour and felt peace. Other people’s death isn’t scary for me anymore but mine is as I fear for my children.
I think it’s more difficult to talk about death if you haven’t had any personal experience of it. A lot of the time it’s very clinical, with the funeral director taking the body away fairly swiftly. There’s not often the chance to spend time with the dead and say goodbye. It’s almost frowned upon. I took some pictures of my husband dead; before and after he was embalmed. It doesn’t feel right sharing that fact with people as I’m worried they’ll think it weird. It didn’t feel weird to me.
Even though my husband suffered with all the indignities of cancer I believe in the end he had a good death. He’d put his affairs in order, planned his funeral, said goodbye to loved ones and ultimately died in my arms. If if wasn’t for the fact that he was only 48 it would have been perfect.
Dealing with the death was relatively easy compared to getting on with life without them. That’s the hardest bit. When the funeral flowers and cards stop coming. When friends no longer bring cooked dishes round. That’s when the shit hits the fan and you see the size of the hole they have left.
Joanne Baker, 47-year-old full-time parent of two children living in Guiseley
‘I gave her a bag of popping corn – she was being cremated and would have loved that!’
The death of my mother last year was like watching a transition from pain to peace. I miss her so much. The horror of the last 12 hours in A&E and hospital side ward as she slipped into unconsciousness will never leave my memory. The nurses were kind but no one could save her from her journey. As she took her last breaths, I told her to go find her mum now and that we would be OK. It was a privilege to share those moments but terrifying.
I’m a Christian. My mother pre-paid for a cardboard coffin, and at her request we pasted all the grandchildren’s art work on it. Her lid was open and we spent an hour talking to her. Her spirit felt close. I placed momentoes in her coffin and a bag of popping corn just for fun in her hand. She was being cremated and would have loved that!
Jayne Gale, 47-year-old nurse
‘I did not cry at the funeral, nor did I go to view his body’
I experienced my dad’s death at the tender age of 13, in June 2003. I did not cry at the funeral, nor did I go to view his body. I couldn’t believe he was gone for good. Many times I dreamt of bumping into him on the street. I thought he would come back, even though I knew and understood that he wouldn’t.
I think most people find it hard to talk about death either due to a trauma or the death of a loved one, and in many African customs it is taboo to do so. Though it’s been 13 years since my dad left I still weep as if he just died. He was my hero. I have been praying over it, and God has helped me to accept the reality, and to stop living in denial.
Grace, 26-year-old living in Nairobi
Mourners attend a vigil for bus driver Manmeet Alisher at a Sikh temple in Brisbane, after he was burned alive when an incendiary device was allegedly thrown at him while he was letting passengers on at Moorooka
‘There is nothing to fear about death’
I lost a little boy who was just two months old – he suddenly passed away one night unexpectedly. I did not understand how this could happen to me – not even as a punishment because I felt I had never done anything that would have deserved such a chastisement.
This was when I started to try to find an answer, so I began reading about what happened after death, the meaning of life and death, why we are here on earth and so on. I got the answer after 30 years of research, so I know now why this happened to me. To me, death means to continue to live in a different form in another dimension where I will be able to meet all my dear ones who died before me and most importantly review all my past life on earth. I will then know if and how I have progressed spiritually. This will be done without judgment, just with love. Then, I will examine and decide what still has to be improved and go back to earth for another experience.
In 2012 my mother died at the age of 84. She suffered a lot and wished she could die as soon as possible “waiting for the angels to take her”. One day she had an accident at home while cooking – she was burnt and taken to hospital where she died two months later. At the very minute she died, I felt filled with an unutterable sensation of happiness which I couldn’t explain at first and I understood when I was told the precise time when she died. I was so happy that she had been freed at last. My sisters got depressed and didn’t understand my reaction at first, but I told them how I felt and they agreed that it was the best way to deal with our mother’s death.
I hope there will be more records similar to mine, so that people grow aware that there is nothing to fear about death – no judgment, no hell, no punishment – only love exists.
Jean Louis, 65-year-old retired teacher living in France
‘Those who talk openly and honestly about death tend to have a more peaceful, meaninful time at the end of their life’
Popular media images of death and dying often portray an image of inevitable suffering, as does frequent media coverage highlighting the inadequacies of health and social services in providing good end of life care and support. As a result, many people live in fear of death and the dying process and ultimately do not have the death they would have preferred.
Problematic issues including misconceptions, unspoken anxiety, lack of control, or the loved ones of a dying person perceiving the dying process as a ‘bad death’ can all contribute towards problematic grief. My own observations of dying people and bereaved relatives are that those who have talked openly and honestly about death and dying – and who have planned for what they would like to happen when the time comes – tend to have a more peaceful, meaningful time at the end of their life.
Katie Shepherd, 43-year-old clinical nurse specialist in palliative care, and permaculture designer living in Spain and Yorkshire
A skull on a turntable.
‘I dealt with the deaths of those close to me quite badly. It’s why I’m an undertaker’
Death has shaped my entire life, literally. I became an undertaker, something for which you need no professional qualifications almost 17 years ago after seeing Nicholas Albery of The Natural Death Centre talk about a different way of approaching funerals, environmentally, socially and religiously. I had a welter of family deaths as a child, most of whose funerals I didn’t go to. Now we do the opposite, encouraging as much family involvement as possible.
It is entirely understandable that people find it difficult to talk about death. The implications of our own extinction and that of the Earth’s are huge, particularly now we are at a stage when even the planet may die. I dealt with the deaths of those close to me quite badly. It’s why I’m an undertaker – do what I say, not what I do.
My father’s death two years ago was sudden and unexpected. The family gathered, and we supported one another. Tears, yes, but plenty of loving laughter – he had an offbeat personality in some ways with a great sense of humour, even around death: he’d always said (in jest) that when he goes he wanted to be stuffed and sat in a chair so he could be glowering at people!
Of course there is the awful reality of his loss in all our lives, the desperate sadness that he’s not here in the physical. He genuinely hadn’t an enemy in the world, and family, friends and colleagues past and present, travelled from far and wide to be at his funeral.
I know that he’s still present though, with countless confirmations of that, so we still go on walks together (a shared love of nature) and we ‘chat’ daily. It’s the next best thing to being in the same physical universe.
Angela, 55-year-old artist and writer living in Ireland
‘It is far easier to grieve among family and friends’
My father died while I was working in Saudi Arabia in the 1980s. My brother sent a telegram, but my employers (who had my passport in a safe) did not pass the telegram to me. I found out a few weeks later via a letter from my mother which started from the premise that I knew already. From this experience I learned that it is far easier to grieve and move on if you do it among family and friends.
Dying is taboo among health and care professionals who sometimes prioritise medical initiatives over individuals and families
Don’t Leave Me Now, a play about early onset dementia, was performed at St Gemma’s hospice in Leeds to an audience of healthcare professionals.
[S]eth Goodburn seemed fit and well until two weeks before he was diagnosed with pancreatic cancer. He died just 33 days after diagnosis, spending much of that short time in hospital. In the emotional whirlwind of coping with the poor prognosis his wife, Lesley, felt their hopes for Seth’s end-of-life care were sidelined by medical professionals trying to do their job.
“The NHS focuses on the medicine and trying to fix people even when that’s not possible,” she says. “A lot of the conversations and decisions that we might have made were overshadowed by dealing with what was the next medical treatment and intervention.”
There is an ongoing conversation in the medical profession about how to care for terminally ill patients, given that the profession’s instinct is to preserve life. The issue is just one of many being address by Brian Daniels, a playwright commissioned by the National Council for Palliative Care (NCPC) to tell stories such as Goodburn’s through plays, and help educate healthcare professionals about patients and families’ experiences of end-of-life care.
Homeward Bound, a play based on a series of letters Lesley Goodburn wrote, in the months after her husband’s death, to medical professionals involved in his care, launched NCPC’s national conference this year to an audience of 300 healthcare workers.
In addition, Daniels’ plays on early onset dementia and palliative care for those with disabilities, have been performed in hospitals, hospices, care homes and to general audiences across the country. Daniels says: “[They] take people out of their professional role for a minute to look at the family and human side of the people they’re dealing with.”
For Goodburn, that human aspect is key. She could not fault the professionalism of those involved in caring for her husband, but says poor communication could leave the couple feeling worse. “There were just so many things where people weren’t cruel or unkind or deliberately unthinking, but just didn’t really think about what it was like to be me and Seth. He went from being well and living a normal life to suddenly being told that he was dying.” She says, for example, a physiotherapist asked Seth to march on the spot as part of an assessment to see if he was able to go home, as he had previously wished, seemingly unaware that his condition had deteriorated and he was dying.
An actor in Don’t Leave Me Now.
Claire Henry, chief executive of the NCPC, says plays such as Homeward Bound are designed to encourage medical professionals to reflect on the people going through this traumatic process. “We obviously work very closely with people who have experience and they tell us their stories. Some are good, some not so good. Healthcare professionals don’t go to work to do a bad job, but sometimes they don’t think of things that affect people in a broader sense.”
What impact does a play have that a lecture, for instance, cannot? Don’t Leave Me Now, another play by Daniels, about early onset dementia, was performed at St Gemma’s hospice in Leeds to an audience including nurses, housekeeping staff and workers from other local hospices. Dr Mike Stockton, its director of medicine and consultant in palliative medicine, says the play enabled them to see some of families’ and patients’ challenges through a different lens. “It’s sometimes hard to have a full understanding … of what people may be going through and the reasons behind their actions or the emotional challenges, adjustments or the resilience that people need.”
Lynn Cawley agrees. There was barely a dry eye at a performance at Morley Arts Festival in October of Bounce Back Boy, the powerful dramatisation of her adopted son, Josh’s, story. Josh was severely disabled following a serious head injury as a baby, and later adopted by Cawley. Despite pioneering medical treatment throughout Josh’s life, Cawley says he was denied admission as an inpatient to a local hospice because his needs were too complex, and died a difficult death at home. She is fighting to end what she describes as end of life discrimination against those with disabilities.
Cawley thinks a play is an effective way of communicating that message, and for getting people to think about palliative care more broadly. She says: “When it’s someone’s real life story, people put themselves in it [and] they might think of a patient that they know. We hope that it will change policy but also people’s attitudes.”
For Stockton, working in a hospice, the wider issue of how treatment is balanced with patient comfort is a daily consideration. He says the two can often be done together: “It is about having early, thorough, open, honest, transparent conversations with people about what they want.”
For Cawley, as a carer and mother who went through the palliative process, those open conversations about dying are key. “We even find it hard to say the word,” she says. “When we’re watching Casualty on a Saturday night and they’re trying to tell a relative that somebody is dying, but they won’t say the word dying or death, we’re just like – say death!”
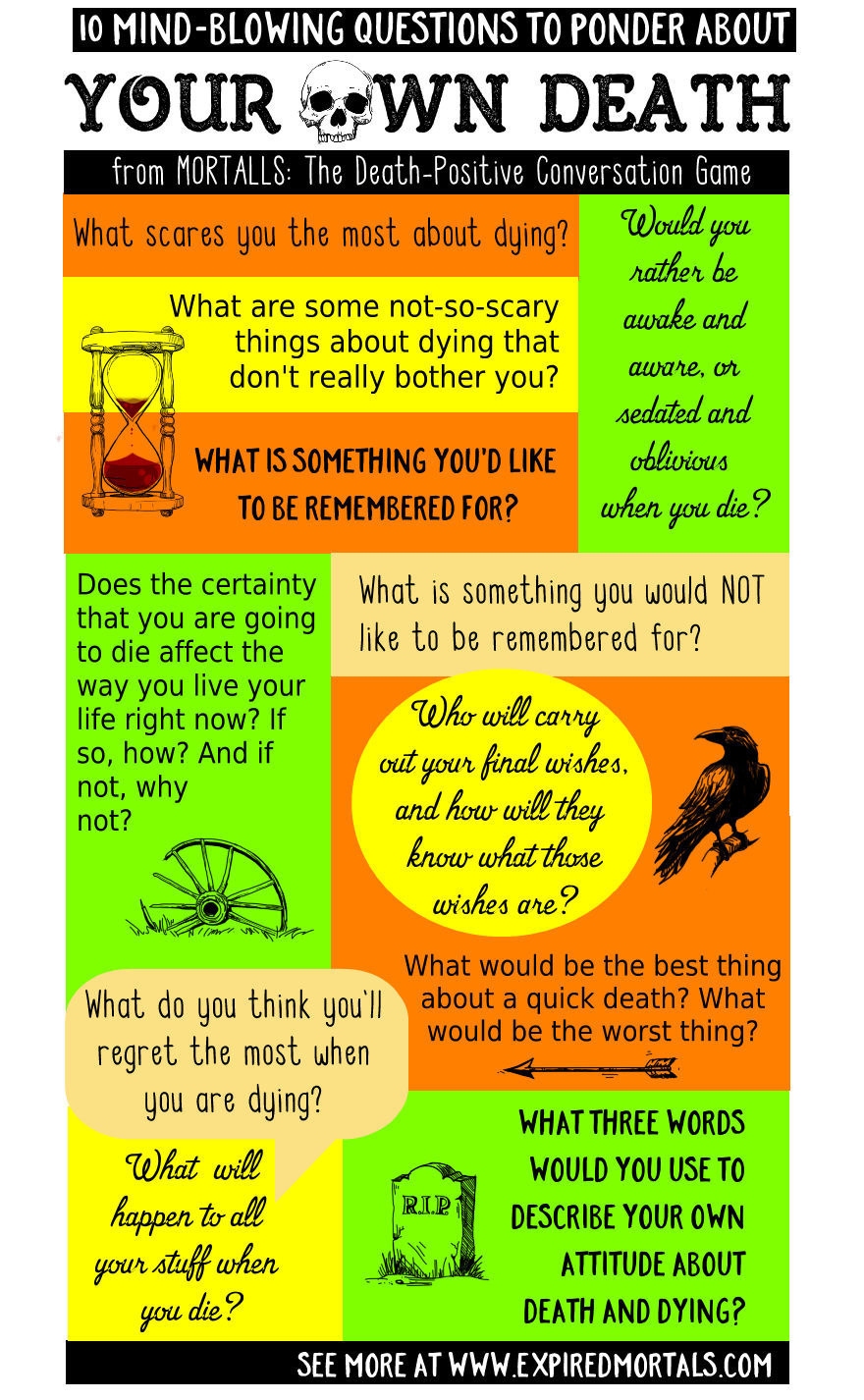
Traditionally, the “Day of the Dead” is a time when family and friends gather to remember friends and family members who have died. But it’s also a perfect time to think about your own death – if you dare.
Care to face your own mortality? Here are 10 Mind-Blowing questions to ponder about your own death.
Most people won’t go there because it’s either too scary, too painful, or we just pretend it will never happen to us. But ready or not, there’s a 100% certainty death will eventually get up close and personal with every one of us. Here, from MORTALLS – The Death-Positive Conversation Game, are 10 mind-blowing but worthwhile questions to ponder about your own death… if you are willing to do so:
What scares you the most about dying?
What are some not-so-scary things about dying that don’t really bother you?
When you die, would you rather be awake and aware, or sedated and oblivious? Why?
What would be the best thing about a quick death? The worst thing?
What do you think you will regret the most when you are dying?
What is something you want to be remembered for?
What is something you do not want to be remembered for?
Who will carry out your final wishes when you die? How will they know what those wishes are?
Does the certainty that you are going to die affect the way you live your life right now? If so, how? And if not, why not?
What three words would you use to describe your own attitude about death and dying?