[W]hen I started medical school, I fully expected to learn how the nervous system works, why heart attacks happen and what to do to stop them, and how the immune system sometimes turns against the body and causes autoimmune diseases. One of the things I needed to learn but didn’t was how to talk with people about death and dying.
To fill that gap, I enrolled in a course at Harvard Medical School on communication strategies during end-of-life care. It was designed to help budding physicians understand how spirituality, end-of-life care, and medicine interact. What I learned surprised me.
I found out that I wasn’t alone in feeling that I was ill-prepared for having effective end-of-life conversations. Physicians in general tend to be particularly limited in their ability to discuss issues such as how long patients will survive, what dying is like, or whether spirituality plays a role in their patients’ last moments.
At first glance, physicians’ poor understanding of death and the process of dying is baffling, since they are supposed to be custodians of health across the lifespan. Look deeper, though, and it may reflect less the attitudes of physicians themselves and more the system that nurtures them. After all, we train vigorously on how to delay the onset of death, and are judged on how well we do that, but many of us get little training on how to confront death.
At one of the seminars that are part of the course, a young man was asked about how he felt during the final days of his mother’s struggle with cancer. “Pain is not suffering if it has a meaning; if it doesn’t, pain and suffering are the same thing,” he said.
That juxtaposition of pain and suffering struck me as an important reminder of the vital role physician communication plays from a patient’s point of view. I realized that a transparent communication strategy can ease suffering and make pain more bearable.
In the process of my coursework, I also realized that significant communication barriers exist between physicians and patients to discussing end-of-life care. When physicians aren’t trained about how to approach patients and their families regarding end-of-life decisions, it’s difficult, if not impossible, to provide the care they want and need.
In one survey, nearly half of the medical students and residents who responded reported being underprepared to address patient concerns and fears at the end of life. About the same percentage said that “dying patients were not considered good teaching cases.” In other words, patients on palliative care with no need of further interventions were seen as offering little in the way of imparting clinical knowledge — even though they might have been wonderful cases for learning more about death and dying.
It’s still unclear whether such limitations arise from personal difficulty talking about this sensitive topic, an inadequate medical curriculum, or a lack of training during residency on how to communicate with terminally ill patients.
When a robust rapport between patient and physician is lacking, or when a physician hasn’t taken enough time to lay out all the options, hospitals tend to follow the “standard” protocol: patients — often at the insistence of family members — are connected to several intravenous lines and an intubation tube, or put on life-support machines, all because the patient or the family never had a clear conversation with the medical team about the severity of the disease and its progression.
That’s not how physicians prefer to die. In a famous essay, an experienced physician wrote that most doctors would prefer to die at home, with less aggressive care than most people receive at the ends of their lives. They understand that such efforts are often futile and take away from the precious time that could be spent in the company of family and friends.
Intensive management of patients with poor prognosis can result in severe emotional damage to patients and their family members. They also have significant policy implications: On average, 25 percent of Medicare payments go to patients in the last year of life, with one-third of that spent in the last month, often on clinical services with negligible benefits.
Physicians certainly share some of the blame for these gaps in communication. But we need to be aware of the role health care systems play in shaping end-of-life interactions. Over-treatment is often encouraged, and with little guidance or feedback on how to navigate end-of-life care, physicians can feel vulnerable to malpractice lawsuits. Due to ever-changing regulations, most interns, residents, and attending physicians are forced to spend more and more time typing into their patients’ electronic health records and less time sitting with their patients, talking with them and understanding what they want and need at the ends of their lives. The issue of resource allocation may also play a role. Medical centers often suffer from a shortage of physicians, and struggle to balance comprehensive teaching with quality patient care.
NHS nurses offer advice on when to question doctors and how to deal with patients you don’t like
‘Good nurses are really tuned into their gut instinct and new nurses should learn to trust it.’
Don’t be afraid to question senior doctors
Never be scared to question a doctor, however senior they may be. We are our patients’ advocates and can protect them from potential mistakes. A good doctor will respect you for this. If you feel something isn’t right but are not confident enough to challenge a situation yourself, go to someone you know, trust and respect – watch how they deal with it and learn. Emma McLellan, staff nurse in the ICU, Manchester
Learn to trust your gut instinct
I believe good nurses are really tuned into their gut instinct and new nurses should learn to trust it. A nurse’s gut instinct is their deeply grounded knowledge base developed in practice, their critical awareness and what they have learned from previous situations plus an overall sense of knowing the patient well. You’ll just know something doesn’t add up, or you may convinced there’s something more going on, so make sure you go that extra mile to cover all bases. Maybe, for example, all of a patient’s baseline observations are normal, but you just sense that there is still that underlying thing you can’t put your finger on – monitor them really closely because you’ll often be right. Zoë Hartwright, community mental health nurse, Shropshire
Death is a part of nursing – talk about it with patients
Death is a regular part of nursing. Patients need someone to talk frankly about death. We plan births for nine months, but talking about death always seems awkward and hard. One of the best things you can do for a patient who is nearing the end of their life is to give them opportunities to talk about their death and how they would like it to be. Being able to give advice and support to help them get their affairs in order can relieve a lot of their pain and worry. It is possible to have a good death but the conversations have to be had.
When death is unexpected this is very hard to deal with. I worked in an accident and emergency department for 10 years and learned that life and death is unpredictable. I have seen many patients and nurses struggle with the last words that they said to that person, so I try to adopt the approach of being kind. Really think about what you say during emergency situations – it is likely that patient can hear you right to the end – even if the rest of their body is not responding. Use their name, talk calmly to them, explain everything you do as you are doing it. Speak to them as if they are awake. Christine Bushnell, advanced nurse practitioner, nurse partner in a GP surgery and trainer, Harrow
Be kind to patients’ relatives
It’s very hard not to take it personally when relatives are difficult with you. As a nurse in paediatrics, I found it tough at first as a newly qualified nurse without any children of my own. Now that I am older and I have my own children, it is different. When dealing with emotional or difficult relatives, try to put yourself in their position and understand that they do not have anything against you – they are just desperately worried about their child, for example, and you may be the nearest person to them and so they might take it out on you. It is important to listen without judging and, if treated with hostility, try to respond with kindness. Speak to your manager if certain behaviour from a family member is bothering you, but ultimately try to be understanding.
Don’t say, “I know how you feel” when you have never been in that situation. Instead you can say something like: “I can’t begin to imagine how worried you must be, but we are doing everything we can, if you have any questions please ask and if I can’t answer them I will find someone who can, etc”. Sally al-Habshi, paediatric emergency nurse, Leicester
Be nice to healthcare assistants
Always be nice to healthcare assistants, they’re amazing. Make lists of jobs you need to do – a good list helps everything. And always remember that when you’re having a bad day, your shift will come to an end and you can go home and eat pizza. Laura Thompson, ward manager, London
[C]olin Barber takes great comfort in the fact that his terminally ill wife, Valerie, was able to die peacefully in her own bed.
On Tuesday, September 1, 2015, ten days after she had been discharged from hospital, Valerie, who had bile duct cancer, took her last breath at home in their bedroom — ‘exactly as she had wanted, with her father and me on each side of her bed, gently holding her hands’, recalls Colin, 56, a business psychologist.
It was, he says, as serene a death as it could have been.
Yet it was nearly so very different. Instead of spending her last few days in peace at home, Valerie, like many patients, could have ended up being rushed to hospital and dying on an anonymous, noisy ward.
But she was one of the lucky ones: she was able to plan for her last days and ensure her wishes were adhered to, thanks to an award-winning new approach to end-of-life care known as soul midwifery.
The idea is that, just as a birth midwife helps to ease a baby’s entry into the world, a ‘soul midwife’ eases people’s dying days.
It is a cruel failure of modern medicine that while the vast majority of people — eight out of ten, according to the Office for National Statistics — want to die at home with their symptoms controlled and their loved ones around them, nearly half actually die in hospitals. Only one in five gets to die at home.
And just how ghastly dying in hospital can be was set out in a report by the British Medical Association published last March.
Based on interviews with more than 500 doctors and patients, it painted a grim picture of patients being given ‘entirely inappropriate invasive treatments’, and junior doctors often too fearful to provide adequate pain control.
Pressure on beds can mean dying patients are ‘shuffled between wards’, preventing continuity of care, while single rooms are prioritised for patients who pose an infection risk, so the dying rarely get privacy. The NHS failure to provide a dignified, peaceful death was highlighted this month by a study published in the BMJ’s Palliative and Supportive Care journal, which identified a postcode lottery in specialist palliative care.
As a result of this, patients are far more likely to be rushed to A&E at the end of their lives than to die pain-free, in peace, at home.
NURSES HAVE NO TIME TO CARE
The BMJ report followed a recent survey of almost 1,000 hospital nurses in which two thirds revealed they didn’t have enough time to care properly for dying patients.
Such is the concern that patients are being failed, that last week the National Institute for Health and Care Excellence (NICE) re-published guidance on end-of-life care first issued to doctors in 2015.
This restated four essentials: the need for doctors to draw up a care plan, provide individualised symptom control, monitor patients daily and ensure adequate hydration. Most people, says Professor Gillian Leng, deputy chief executive of NICE, receive good end-of-life care ‘but this isn’t always the case’.
End-of-life champion: Felicity Warner established soul midwifery in 2004
Good care involves asking people about their preferences as well as controlling pain, adds Sam Ahmedzai, a retired professor of palliative care who worked on the latest NICE guidance.
Yet a recent study showed that only one person in seven who could communicate their desires had those wishes documented.
This is far from a new problem. Ten years ago, a major report, the End of Life Care Strategy, featured an innovative plan to end the situation where ‘most people would prefer to die at home while only a minority manage to do so’, as then Health Secretary Alan Johnson put it.
Along with improved palliative care, the plan involved healthcare practitioners working harder to ‘identify people approaching the end of life and discuss with them their needs and preferences’.
DOCTORS CAGEY ABOUT THE TRUTH
Ten years on, although there has been a slight improvement (back then nearly six out of ten people were dying in hospital) there is still ‘a long way to go’, Claire Henry, chief executive of the National Council for Palliative Care, told Good Health this week.
So why is it still proving so difficult to get things right?
‘Some deaths happen suddenly, out of the blue, while with some patients it’s difficult to be sure whether they are dying or will recover,’ says Professor Ahmedzai.
‘That’s why we say that every patient in the last days of life should be monitored daily in case there have been changes and there is a chance of recovery.’
Research shows that, in fact, in four out of five cases GPs can predict which of their patients will die within the next 12 months. And three out of four deaths are anticipated by medical teams, according to NICE.
Professor Ahmedzai says: ‘We should be asking anyone admitted to hospital with a serious illness about their preferences for where and how they wish to die, should that look likely. But doctors often don’t because they are embarrassed or just too busy to handle that conversation. It can’t be an excuse. We must make time for the dying.’
Indeed, a major problem is that too often, dying patients simply are not told what their doctors know. Sometimes this is because doctors are unwilling to discharge patients so they can die at home because effectively ‘such a decision can be seen as an acceptance of failure’, the recent BMA report noted.
Research shows that in four out of five cases GPs can predict which of their patients will die within the next 12 months
Certainly, no one told Valerie or Colin that she was dying.
The banking relationship manager from Brentwood, Essex, had cancer diagnosed in 2013, two weeks after her 50th birthday, after noticing that the whites of her eyes were yellow.
Her GP referred her for an MRI scan, which revealed a large tumour wrapped around her bile duct.
She had surgery to remove part of her liver along with the gall bladder and bile duct, followed by three months of chemotherapy.
‘After the treatment we began to be optimistic that she was recovering,’ says Colin. But in October 2014 a scan identified nodules of cancer in the liver, too scattered to be removed surgically. In August 2015, Valerie took a sudden turn for the worse and had to be admitted to hospital.
‘We’d just come back from holiday, when she’d canoed 15 miles down the River Severn,’ recalls Colin. ‘Then one day she woke up so weak she could barely stand.’
Even so, ‘it didn’t occur to me that she was gravely ill,’ he recalls. ‘No one at the hospital mentioned the word ‘dying’.’
Valerie’s discharge from hospital three days later depended only on a physiotherapist checking that she could walk upstairs, which the couple took to mean she was on the mend.
‘But looking back on it, her doctors must have been aware that she was dying,’ says Colin. Not least because the next day, after an appointment with the cancer specialist, she was referred to hospice care.
It was not her doctors but Valerie herself who first put what was imminent into words. ‘Back at home, Valerie told me she was dying and I had to accept it,’ recalls Colin. That was when she asked him to be her soul midwife, ensuring her dying days were as she wanted them.
CARERS TO EASE THE LAST DAYS
Soul midwifery is a unique approach to end-of-life care.
In the words of Felicity Warner, the woman who founded it, ‘just as a birth midwife ensures a safe delivery into this world, the soul midwife’s role is to do the same for the dying, to make a good death possible, a dignified, peaceful and even enriching experience’.
This means ‘providing comfort, continuous support and reassurance’ — in practice, after a terminal diagnosis, this involves helping to support the patient as they make an end-of-life plan.
In the final stages the soul midwife might sit by the dying person, holding their hand, playing soothing music and burning appropriate oils. Krista Hughes, a soul midwife based in Chertsey, Surrey, works privately in people’s homes but is often called to a hospice, she says, to work with those with ‘terminal agitation’.
It is a term recognised by clinicians and often managed with sedatives, but as a soul midwife, she prefers gentle breathing, maintaining eye contact and softly repeating the person’s name.
The work of soul midwives was recognised when Felicity Warner was named 2017 End of Life Care Champion by the National Council for Palliative Care and the Royal College of Nursing. The seed for soul midwifery was planted more than 20 years ago when Felicity, now 58, was working as a journalist and interviewed several women dying of breast cancer.
The women told ‘how lonely it felt to be dying despite their medical care and their families around them’.
Not only were their doctors and nurses too busy to talk about death and dying but, surprisingly, Felicity found the women were becoming increasingly distant from friends and family who couldn’t cope with the reality and masked it with platitudes such as: ‘You’ll be feeling better soon.’
Researching how people died before the rise of modern ‘curative’ Western medicine, Felicity found a range of practices ‘that had in common the fact that they respected the act of dying as a sacred time’.
She established soul midwifery in 2004, and has since trained 600 soul midwives — many already have a health practitioner qualification — with an initial three-day course, followed by an apprenticeship lasting around a year.
Qualified soul midwives’ costs are in line with local rates for services such as counselling, though many also work as volunteers at hospices or use the qualification to help care for a terminally ill relative.
Valerie herself had attended a three-day soul midwives’ course shortly after recovering from the cancer surgery in August 2014.
‘It was something she thought she would like to do one day when she was stronger,’ recalls Colin.
So when Valerie told him she thought death might be near, he asked if she wanted him to contact the organisation to arrange for a soul midwife to visit.
Instead, she told him to read her copy of the soul midwives’ handbook so he could take on the role.
For Colin, this meant as well as ensuring Valerie’s comfort, he was her gatekeeper.
While many people want strong intravenous pain control in their last days, Valerie didn’t — ‘she wasn’t in much pain and wanted clarity of thought to the end, yet it took time and effort to stop the palliative care team administering the sedatives,’ says Colin.
‘I had to contact Valerie’s GP and get him to approve her decision, then inform the hospice nurses.’
Three days before she died, the couple celebrated their 17th wedding anniversary. ‘We wrote cards for each other and exchanged presents. The next morning, Valerie told me she had stayed for our anniversary and now she was ready to go. It was her time to die.
‘She had told me she wanted to imagine she was floating away on a boat and asked me to play soothing background music. I lit candles and used essential oils.
‘She had also warned me that the last sense to go would be her hearing, so I read prayers and spiritual affirmations.’
Soul midwifery will not be for everyone. But Colin is in no doubt that it helped Valerie to a comfortable and tranquil death.
‘Of course I longed for a last-minute reprise, a miracle recovery that would keep her with me. But I recognised that Valerie knew what her body was telling her, and did my best to concentrate on our time well spent together. I’m certain she knew that, and appreciated it.’
Effigies in Scotland from the 17th century, when death was simpler.
By Haider Javed Warraich
[E]very Thursday morning on the heart transplant service, our medical team would get a front-row seat to witness an epic battle raging under a microscope. Tiny pieces of heart tissue taken from patients with newly transplanted hearts would be broadcast onto a gigantic screen, showing static images of pink heart cells being attacked by varying amounts of blue immune cells. The more blue cells there were, the more voraciously they were chomping away the pink cells, the more evidence that the patient’s inherently xenophobic immune system was rejecting the foreign, transplanted heart.
There was so much beauty to be found in the infinitesimal push and pull between life and death those slides depicted that I would fantasize about having them framed and put up in my house. Yet the more I studied those cells, the more I realized that they might have the answers to one of the most difficult subjects of our time.
Throughout our history, particularly recently, the human race has looked far and wide to answer a complex question — what is a good death? With so many life-sustaining technologies now able to keep us alive almost indefinitely, many believe that a “natural” death is a good one. With technology now invading almost every aspect of our lives, the desire for a natural death experience mirrors trends noted in how we wish to experience birth, travel and food these days.
When we picture a natural death, we conjure a man or woman lying in bed at home surrounded by loved ones. Taking one’s last breath in one’s own bed, a sight ubiquitous in literature, was the modus operandi for death in ancient times. In the book “Western Attitudes Toward Death,” Philippe Ariès wrote that the deathbed scene was “organized by the dying person himself, who presided over it and knew its protocol” and that it was a public ceremony at which “it was essential that parents, friends and neighbors be present.” While such resplendent representations of death continue to be pervasive in both modern literature and pop culture, they are mostly fiction at best.
This vision of a natural death, however, is limited since it represents how we used to die before the development of modern resuscitative technologies and is merely a reflection of the social and scientific context of the time that death took place in. The desire for “natural” in almost every aspect of modern life represents a revolt against technology — when people say they want a natural death, they are alluding to the end’s being as technology-free as possible. Physicians too use this vocabulary, and frequently when they want to intimate to a family that more medical treatment may be futile, they encourage families to “let nature take its course.”
Yet, defining death by how medically involved it is might be shortsighted. The reason there are no life-sustaining devices in our romantic musings of death is that there just weren’t any available. Furthermore, our narratives of medical technology are derived largely from the outcomes they achieve. When death is unexpectedly averted through the use of drugs, devices or procedures, technology is considered miraculous; when death occurs regardless, its application is considered undignified. Therefore, defining a natural death is important because it forms the basis of what most people will thus consider a good death.
Perhaps we need to observe something even more elemental to understand what death is like when it is stripped bare of social context. Perhaps the answer to what can be considered a truly natural death can be found in the very cells that form the building blocks of all living things, humans included.
Though we have known for more than a century how cells are created, it is only recently that we have discovered how they die. Cells die via three main mechanisms. The ugliest and least elegant form of cell death is necrosis, in which because of either a lack of food or some other toxic injury, cells burst open, releasing their contents into the serums. Necrosis, which occurs in a transplanted heart undergoing rejection, causes a very powerful activation of the body’s immune system. Necrosis, then, is the cellular version of a “bad death.”
The second form of cell death is autophagy, in which the cell turns on itself, changing its defective or redundant components into nutrients, which can be used by other cells. This form of cell death occurs when food supply is limited but not entirely cut off, such as in heart failure.
The most sophisticated form of cell death, however, is unlike the other two types. Apoptosis, a Greek word used to describe falling leaves, is a programmed form of cell death. When a cell becomes old or disrepair sets in, it is nudged, usually by signaling molecules, to undergo a form of controlled self-demolition. Unlike in necrosis, the cell doesn’t burst, doesn’t tax the immune system, but quietly dissolves. Apoptosis is the reason our bone marrow doesn’t weigh two tons or our intestines don’t grow indefinitely.
As important as apoptosis is to death, it is essential for life. While as humans, we often consciously or unconsciously hope to achieve immortality, immortality has a very real existence in the cellular world — it’s called cancer. In fact, most cancers occur because of defects in apoptosis, and most novel cancer therapies are designed to allow cell death to occur as it normally would.
In many ways, therefore, life and death at a cellular level are much more socially conscious than how we interface with these phenomena at a human level. For cells, what is good for the organism is best for the cell. Even though cells are designed entirely to survive, an appropriate death is central to the survival of the organism, which itself has to die in a similar fashion for the sake of the society and ecosystem it inhabits.
We humans spend much of our lives denying death. Death, however, is not the enemy. If there is an enemy, it is the fear that death arouses. The fear of death often induces us to make choices that defy the biological constraints of our existence. Such choices often lead us to a fate that more closely resembles necrosis, involving the futile activation of innumerable resources eventually resulting in a cataclysmic outcome, rather than apoptosis. Furthermore, even as we hope to defy our mortality, our cells show the devastation that can occur for the organism if even one cell among billions achieves immortality.
When I asked Robert Horvitz, the Nobel Prize-winning biologist at the Massachusetts Institute of Technology who was part of the group that discovered apoptosis, what lessons we could learn from cell death, his answer demonstrated exactly why we have failed to understand death in the context of our lives: “Only once before has someone approached me to discuss the existential questions that might relate what is known about cell death to human existence.”
The question for us, then, is: What is the human equivalent of apoptosis in the context of our society? One way to approach that question is to look at what the human equivalent of necrosis is. To me, if a human being is in the hospital with intensive, life-sustaining therapies such as artificial respiration, nutrition or dialysis sustaining them with little hope of recovering reasonable brain function, such a state could be considered necrosis. Almost any other alternative, whether one dies in the hospital having rescinded resuscitation or intubation (DNR/DNI), at home with hospice services or with the aid of a physician’s prescription, has much more in common with apoptosis.
We have striven endlessly to answer some of our most crucial questions, yet somehow we haven’t tried to find them in the basic machinery of our biology. Apoptosis represents a pure vision of death as it occurs in nature, and that vision is something we might aspire to in our own deaths: A cell never dies in isolation, but in clear view of its peers; it rarely dies of its own volition; a greater force that is in touch with the larger organism understands when a cell is more likely to harm itself and those around it by carrying on. Apoptosis represents the ultimate paradox — for the organism to survive, the cells must die, and they must die well. “There are many disorders in which there is too little apoptotic death,” Dr. Horvitz said, “and in those cases it is activating apoptosis that could increase longevity.”
And finally, a cell also understands better than we humans do the consequences of outlasting one’s welcome. For though humanity aspires to achieve immortality, our cells teach us that a life without death is the most unnatural fate of all.
[W]hen my mum Joan died of oesophageal cancer in 2014, she was in the place she wanted to spend her last days – the spare bedroom at home – with me and my dad, Cliff, by her side.
I’d spent the last week in a camp bed next to Mum, wiping her lips and mopping her forehead as we shared memories.
On the night she died, she put her arm around me and said “Adrienne, I have to thank you for being the most wonderful daughter.” Afterwards, our district nurse made my dad a whisky and me a cup of tea as we said our final goodbyes.
Not without serious difficulty
Mum had a ‘good death’, but not without serious difficulties at times. I can’t help thinking it was my background as a district nurse that allowed her to die at home with her family. My experience meant I was listened to, and I pushed for her to get what she needed, such as acupuncture at the local hospice to relieve her crippling pain from arthritis. I knew what to expect and what conversations to have. We had early discussions about how she wanted to die (at home, not in hospital) and where (not next to Dad in their bed), which we call Advance Care Planning in the medical profession. At Macmillan, we believe that more needs to be done to ensure people are planning for their deaths, so their wishes – such as where they die – can be met.
Sadly, a death like my mum’s is denied to so many in this country. And I believe it would have been impossible for her too, had she not happened to have a nurse for a daughter. I had to fight to get her the care she desperately needed. Services are depleted, especially out of hours. You can’t choose when advanced cancer will cause you pain, but getting pain-relief at night or on weekends can be impossible. In her final days, there was no availability for a night sitter. Thankfully, I could be by her bedside, but had I not been, I’m convinced she would have died in hospital against her wishes.
Findings published in the British Medical Journal last week help explain why some people aren’t getting enough support when they are dying. Care for dying people varies hugely across different regions, both in how much money services are allocated and what care they offer. Figures suggested that, in most parts of the country, there are no specialist pain control teams, and, where they are in place, most operate only in normal working hours with no cover overnight. Until you’ve had a loved one in pain, with no way of providing them relief, it’s hard to appreciate the urgency of this situation.
Having a choice
Pain relief is the very least we should expect at the end of our lives. But it’s also important that, where possible, patients can die in a place of their choosing. We know that most people with advanced cancer would prefer to die at home, but not many of them actually do. Without round-the-clock community nursing, it’s hard to see how this will improve.
My days as a district nurse taught me that getting things right for people at the end of their life takes time. Decisions made about treatment affect how that person will spend their last months, weeks, hours, in this world. But time is something our overstretched workforce doesn’t have. Last month came another heart-breaking revelation – that over two thirds of nurses ‘don’t have time’ to care for dying patients. Is this really what we’ve come to? Something has to change.
Painless death must be priority
I know what a good death looks like, and that it is achievable. But to give everyone a chance to die without pain, and in the place they want to, care for dying people needs to be a priority across the country. As the NHS and local councils set out their plans to transform healthcare, it’s vitally important that they take into account how they will care for people at the end of their lives. At Macmillan, we’ll be monitoring these plans closely to make sure they do.
Those last few weeks with my mum were exhausting, but they were special and irreplaceable. Helping her in her final days with the people she loved, in the house she knew, was the most meaningful thing I’ve ever done. Caring how people die isn’t just about death, but about the value we place on life.
Sickness and early death in the white working class could be rooted in poor job prospects for less-educated young people as they first enter the labor market, a situation that compounds over time through family dysfunction, social isolation, addiction, obesity and other pathologies, according to a study published Thursday by two prominent economists.
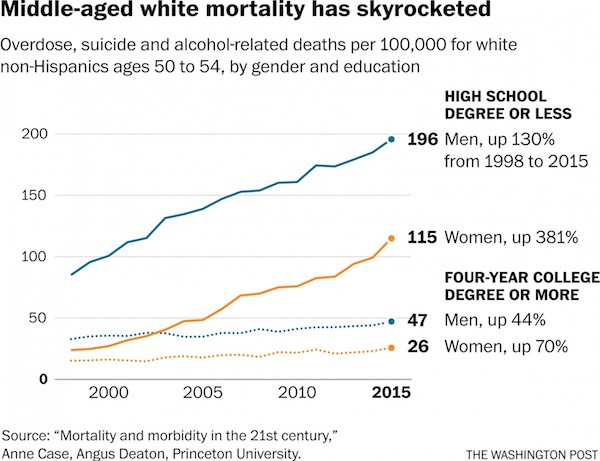
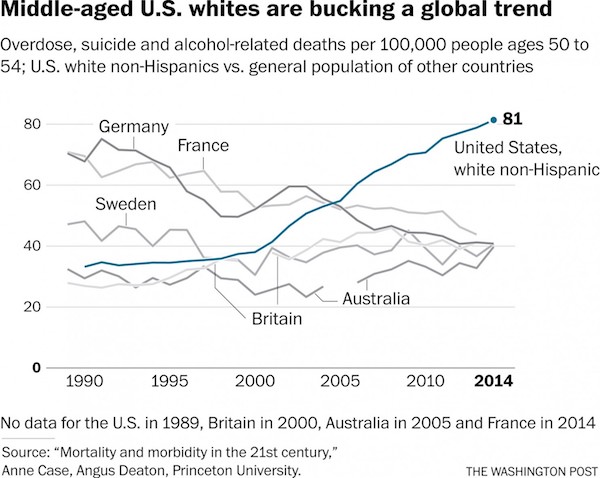
Anne Case and Angus Deaton garnered national headlines in 2015 when they reported that the death rate of midlife non-Hispanic white Americans had risen steadily since 1999 in contrast with the death rates of blacks, Hispanics and Europeans. Their new study extends the data by two years and shows that whatever is driving the mortality spike is not easing up.
The two Princeton professors say the trend affects whites of both sexes and is happening nearly everywhere in the country. Education level is significant: People with a college degree report better health and happiness than those with only some college, who in turn are doing much better than those who never went.
Offering what they call a tentative but “plausible” explanation, they write that less-educated white Americans who struggle in the job market in early adulthood are likely to experience a “cumulative disadvantage” over time, with health and personal problems that often lead to drug overdoses, alcohol-related liver disease and suicide.
“Ultimately, we see our story as about the collapse of the white, high-school-educated working class after its heyday in the early 1970s, and the pathologies that accompany that decline,” they conclude.
The study comes as Congress debates how to dismantle parts of the Affordable Care Act. Case and Deaton report that poor health is becoming more common for each new generation of middle-aged, less-educated white Americans. And they are going downhill faster.
In a teleconference with reporters this week, Case said the new research found a “sea of despair” across America. A striking feature is the rise in physical pain. The pattern does not follow short-term economic cycles but reflects a long-term disintegration of job prospects.
“You used to be able to get a really good job with a high school diploma. A job with on-the-job training, a job with benefits. You could expect to move up,” she said.
The nation’s obesity epidemic may be another sign of stress and physical pain, she continued: “People may want to soothe the beast. They may do that with alcohol, they may do that with drugs, they may do that with food.”
Similarly, Deaton cited suicide as an action that could be triggered not by a single event but by a cumulative series of disappointments: “Your family life has fallen apart, you don’t know your kids anymore, all the things you expected when you started out your life just haven’t happened at all.”
The economists say that there is no obvious solution but that a starting point would be limiting the overuse of opioids, which killed more than 30,000 Americans in 2015.
The two will present their study on Friday at the Brookings Institution.
“Their paper documents some facts. What is the story behind those facts is a matter of speculation,” said Adriana Lleras-Muney, a University of California at Los Angeles economics professor, who will also speak at Brookings.
She noted that less-educated white Americans tend to be strikingly pessimistic when interviewed about their prospects.
“It’s just a background of continuous decline. You’re worse off than your parents,” Lleras-Muney said. “Whereas for Hispanics, or immigrants like myself” — she is from Colombia — “or blacks, yes, circumstances are bad, but they’ve been getting better.”
David Cutler, an economics professor at Harvard who also will be discussing the paper at Brookings, said the declining health of white, working-class Americans suggests that Republican plans to replace the Affordable Care Act are akin to bleeding a sick patient. As he put it, “Treat the fever by causing an even bigger fever.”
Whites continue to have longer life expectancy than African Americans and lower death rates, but that gap has narrowed since the late 1990s. The picture may have shifted again around the Great Recession, however: Graphs accompanying the new paper suggest that death rates for blacks with only a high school education began rising around 2010 in many age groups, as if following the trend that began about a decade earlier among whites.
White men continue to die at higher rates than white women in every age group. But because women started with lower death rates, the recent mortality increase reflects a greater change in their likelihood of dying early. The numbers reported by Case and Deaton suggest that white men today are about twice as likely as they were in 1999 to die from one of the “diseases of despair,” while women are about four times as likely.
Case and Deaton play down geography as a factor in the epidemic. Yet they note that white mortality rates fell in the biggest cities, were constant in big-city suburbs and rose in all other areas. The Washington Post’s analysis published last year highlighted the same geographical signature, with a break in death rates between the two most urban classifications (big cities and big-city suburbs) and the four less urban classifications, which The Post described as an urban-rural divide.
Last week, the Centers for Disease Control and Prevention published a report on U.S. suicides by level of urbanization between 1999 and 2015, a period in which 600,000 Americans took their own lives. The report showed rising rates in each of the six urbanization classifications but found “a geographic disparity” in which rates increased as urbanization decreased. That urban-rural divide appears to have widened, particularly in recent years, the CDC reported.
Medical students do not learn how to talk about death. Junior doctors are forced to learn on the job – and that isn’t fair on patients or families
‘Death cafes aren’t a solution to lack of teaching, but all medical students should attend one.’
By Isabella Laws
[I]t is taboo in British culture to talk about death. We say someone has “passed away”, “kicked the bucket” or “left us” – anything to avoid even using the word. This has consequences. While 70% of people wish to die at home, half of us will actually die in hospital. Our reluctance to talk about death and make our wishes known is part of the reason for this.
So I didn’t expect to enjoy visiting a death cafe. As soon as I arrived, I knew I had made the right decision, however. The room hummed with a low level of chatter, and I felt prepared to practise talking about death and dying.
On that particular morning there were six of us in the cafe: two academic psychologists, a woman who had lost her husband in her early 30s, a grief counsellor and a man who had had a near-death experience. There was also a group leader, although the conversation was completely unstructured save for initial introductions – and the proviso that everything we discussed must be about death.
Death cafes were founded in the UK in 2011, inspired by a Swiss model, and the aim is simple: to increase awareness and openness about death with a view to helping people make the most of their (finite) lives. There are now more than 4,000 cafes held around the UK, Europe and north America.
After the death cafe, I couldn’t believe that I had spent two hours talking exclusively about dying. It was satisfying to talk to others who were honest about their experiences and fears. Nearly everyone regretted not speaking more frankly about it with their parents before they died. They also worried about raising the topic with their children: who should raise it? When is the right time? What if they shut the conversation down? One woman asked the group what kind of legacy we each wanted to leave behind. She worried that she had not been close to her family and they would not remember her in the way she wanted when she dies.
I was by far the youngest person there. This is unsurprising – people in their 20s don’t often think about death. I went because there is a fundamental lack of teaching at medical school to prepare you for the fact that this is something I will have to deal with every day as a doctor. In six years of study, I will have had just one small group session on “breaking bad news”. Yet as soon as I am qualified, I will be expected to talk about death and dying to patients and their loved ones on a daily basis. Last year, I saw a doctor only months out of medical school comfort a woman after her husband’s death. The same would be expected of me in just over a year’s time – and I was not ready.
In 2000, an average of 20 hours (pdf) were dedicated to palliative care teaching at medical school. I certainly haven’t experienced any increase on that figure, 17 years later.
I have witnessed good practice during my training, but there have also been times when I wished I wasn’t in the room. Last year, while sitting in on a neurology clinic, I watched as a patient was told they had motor neurone disease. Their face went blank and pale with shock, but the doctor seemed oblivious and launched into a monologue about the patient’s treatment options and prognosis. I sat in the corner of the room, powerless to intervene. Without teaching doctors effective communication skills as students, how can we be expected to fare any better?
A survey of junior doctors by the Royal College of Physicians of Edinburgh in 2013 found that only half felt prepared for communicating with dying patients and their families. This figure rose to 70% for their clinical trainers.
This lack of teaching lets down not just students, but patients too. A lack of guidance means junior doctors are forced to learn on the job. Undoubtedly, they will improve in time. The patients and families who experience unsatisfactory or even upsetting communication along the way are simply collateral damage.
Death cafes aren’t a solution to lack of teaching, but I think they make a good start. All medical students should attend one. It’s something all of us, without exception, will be affected by. Only through practising these skills can we hope to be effective and sensitive communicators when the time comes for us to break bad news.