

By David Marchese
A decade ago, Hadley Vlahos was lost. She was a young single mother, searching for meaning and struggling to make ends meet while she navigated nursing school. After earning her degree, working in immediate care, she made the switch to hospice nursing and changed the path of her life. Vlahos, who is 31, found herself drawn to the uncanny, intense and often unexplainable emotional, physical and intellectual gray zones that come along with caring for those at the end of their lives, areas of uncertainty that she calls “the in-between.” That’s also the title of her first book, which was published this summer. “The In-Between: Unforgettable Encounters During Life’s Final Moments” is structured around her experiences — tragic, graceful, earthy and, at times, apparently supernatural — with 11 of her hospice patients, as well as her mother-in-law, who was also dying. The book has so far spent 13 weeks on the New York Times best-seller list. “It’s all been very surprising,” says Vlahos, who despite her newfound success as an author and her two-million-plus followers on social media, still works as a hospice nurse outside New Orleans. “But I think that people are seeing their loved ones in these stories.”
What should more people know about death? I think they should know what they want. I’ve been in more situations than you could imagine where people just don’t know. Do they want to be in a nursing home at the end or at home? Organ donation? Do you want to be buried or cremated? The issue is a little deeper here: Someone gets diagnosed with a terminal illness, and we have a culture where you have to “fight.” That’s the terminology we use: “Fight against it.” So the family won’t say, “Do you want to be buried or cremated?” because those are not fighting words. I have had situations where someone has had terminal cancer for three years, and they die, and I say: “Do they want to be buried or cremated? Because I’ve told the funeral home I’d call.” And the family goes, “I don’t know what they wanted.” I’m like, We’ve known about this for three years! But no one wants to say: “You are going to die. What do you want us to do?” It’s against that culture of “You’re going to beat this.”
Is it hard to let go of other people’s sadness and grief at the end of a day at work? Yeah. There’s this moment, especially when I’ve taken care of someone for a while, where I’ll walk outside and I’ll go fill up my gas tank and it’s like: Wow, all these other people have no idea that we just lost someone great. The world lost somebody great, and they’re getting a sandwich. It is this strange feeling. I take some time, and mentally I say: “Thank you for allowing me to take care of you. I really enjoyed taking care of you.” Because I think that they can hear me.
The idea in your book of “the in-between” is applied so starkly: It’s the time in a person’s life when they’re alive, but death is right there. But we’re all living in the in-between every single moment of our lives. We are.
So how might people be able to hold on to appreciation for that reality, even if we’re not medically near the end? It’s hard. I think it’s important to remind ourselves of it. It’s like, you read a book and you highlight it, but you have to pick it back up. You have to keep reading it. You have to. Until it really becomes a habit to think about it and acknowledge it.
I was reading these articles recently about how scientists are pursuing breakthroughs that could extend the human life span to one hundred twenty.1
1
Examples of which could include devising drug cocktails that get rid of senescent cells and filtering old blood to remove molecules that inhibit healing.
There’s some part of people that thinks they can cheat death — and, of course, you can’t. But what do you think about the prospect of extending the human life span? I don’t want to live to be 120. I have spent enough time around people who are close to 100, over 100, to know that once you start burying your children, you’re ready. Personally, I’ve never met someone 100 or older who still wants to be alive. I have this analogy that I did a TikTok2
2
Vlahos has 1.7 million followers on TikTok, where she posts about her experience as a hospice nurse and often responds to questions about death and dying.
on. This is from having a conversation with someone over 100, and her feeling is that you start with your Earth room when you’re born: You have your parents, your grandparents, your siblings. As you get older, your Earth room starts to have more people: You start making friends and college roommates and relationships. Then you start having kids. And at some point, people start exiting and going to the next room: the afterlife. From what she told me, it’s like you get to a point when you’re older that you start looking at what that other room would be, the afterlife room,3
3
According to a 2021 Pew Research survey, 73 percent of American adults say they believe in heaven.
and being like, I miss those people. It’s not because you don’t love the people on Earth, but the people you built your life with are no longer here. I have been around so many people who are that age, and a majority of them — they’re ready to go see those people again.
“The In-Between” also has to do with the experience of being in between uncertainty and knowing. But how much uncertainty is there for you? Because in the book you write about things that you can’t explain, like people who are close to death telling you that they’re seeing their dead loved ones again. But then you write, “I do believe that our loved ones come to get us when we pass.”4
4
From Vlahos’s book: “I don’t think that we can explain everything that happens here on Earth, much less whatever comes after we physically leave our bodies. I do believe that our loved ones come to get us when we pass, and I don’t believe that’s the result of a chemical reaction in our brain in those final hours.”
So where is the uncertainty? The uncertainty I have is what after this life looks like. People ask me for those answers, and I don’t have them. No one does. I feel like there is something beyond, but I don’t know what it is. When people are having these in-between experiences of seeing deceased loved ones, sometimes it is OK to ask what they’re seeing. I find that they’ll say, “Oh, I’m going on a trip,” or they can’t seem to find the words to explain it. So the conclusion I’ve come to is whatever is next cannot be explained with the language and the knowledge that we have here on Earth.

Do these experiences feel religious to you? No, and that was one of the most convincing things for me. It does not matter what their background is — if they believe in nothing, if they are the most religious person, if they grew up in a different country, rich or poor. They all tell me the same things. And it’s not like a dream, which is what I think a lot of people think it is. Like, Oh, I went to sleep, and I had a dream. What it is instead is this overwhelming sense of peace. People feel this peace, and they will talk to me, just like you and I are talking, and then they will also talk to their deceased loved ones. I see that over and over again: They are not confused; there’s no change in their medications. Other hospice nurses, people who have been doing this longer than me, or physicians, we all believe in this.
Do you have a sense of whether emergency-room nurses5
5
Who, because of the nature of their jobs, are more likely than hospice nurses to see violent, painful deaths.
report similar things? I interned in the E.R., and the nurse I was shadowing said that no one who works in the E.R. believes in an afterlife. I asked myself: Well, how do I know who’s correct? How am I supposed to know? Are the people in the church that I was raised with6
6
Vlahos was raised in an Episcopalian family. She now refers to herself, as so many do, as spiritual rather than religious
more correct than all these people? How are you supposed to know what’s right and what’s not?
But you’ve made a choice about what you believe. So what makes you believe it? I totally get it: People are like, I don’t know what you’re talking about. So, OK, medically someone’s at the end of their life. Many times — not all the time — there will be up to a minute between breaths. That can go on for hours. A lot of times there will be family there, and you’re pretty much just staring at someone being like, When is the last breath going to come? It’s stressful. What is so interesting to me is that almost everyone will know exactly when it is someone’s last breath. That moment. Not one minute later. We are somehow aware that a certain energy is not there. I’ve looked for different explanations, and a lot of the explanations do not match my experiences.
That reminds me of how people say someone just gives off a bad vibe. Oh, I totally believe in bad vibes.
But I think there must be subconscious cues that we’re picking up that we don’t know how to measure scientifically. That’s different from saying it’s supernatural. We might not know why, but there’s nothing magic going on. You don’t have any kind of doubts?
None. Really? That’s so interesting. You know, I read your article with the atheist.7
7
“How to Live a Happy Life, From a Leading Atheist,” an interview with the philosopher Daniel C. Dennett, published in August.
I feel like you pushed back on him.
There are so many things in our lives, both on the small and the big scale, that we don’t understand. But I don’t think that means they’re beyond understanding. OK, you know what you would like? Because I know that you’re like, “I believe this,” but you seem to me very interested; you’re not just set in your ways. Have you ever heard that little story about two twins in a womb?8
8
Known as the parable of the twins, this story was popularized by the self-help author Dr. Wayne W. Dyer in his 1995 book “Your Sacred Self: Making the Decision to Be Free.”
I’m going to totally butcher it, but essentially it’s two twins who can talk in the womb. One twin is like, “I don’t think that there is any life after birth.” And the other is like, “I don’t know; I believe that there is something after we’re born.” “Well, no one’s ever come back after birth to tell us that there is.” “I think that there’s going to be a world where we can live without the umbilical cord and there’s light.” “What are you talking about? You’re crazy.” I think about it a lot. Do we just not have enough perspective here to see what could come next? I think you’ll like that story.
For the dying people who don’t experience what you describe — and especially their loved ones — is your book maybe setting them up to think, like: Did I do something wrong? Was my faith not strong enough? When I’m in the home, I will always prepare people for the worst-case scenario, which is that sometimes it looks like people might be close to going into a coma, and they haven’t seen anyone, and the family is extremely religious. I will talk to them and say, “In my own experience, only 30 percent of people can even communicate to us that they are seeing people.” So I try to be with my families and really prepare them for the worst-case scenario. But that is something I had to learn over time.
Have you thought about what a good death would be for you? I want to be at home. I want to have my immediate family come and go as they want, and I want a living funeral. I don’t want people to say, “This is my favorite memory of her,” when I’m gone. Come when I’m dying, and let’s talk about those memories together. There have been times when patients have shared with me that they just don’t think anyone cares about them. Then I’ll go to their funeral and listen to the most beautiful eulogies. I believe they can still hear it and are aware of it, but I’m also like, Gosh, I wish that before they died, they heard you say these things. That’s what I want.
You know, I have a really hard time with the supernatural aspects, but I think the work that you do is noble and valuable. There’s so much stuff we spend time thinking about and talking about that is less meaningful than what it means for those close to us to die. I have had so many people reach out to me who are just like you: “I don’t believe in the supernatural, but my grandfather went through this, and I appreciate getting more of an understanding. I feel like I’m not alone.” Even if they’re also like, “This is crazy,” people being able to feel not alone is valuable.
This interview has been edited and condensed for clarity from two conversations.
Complete Article ↪HERE↩!
My Husband Is Dying
— Advice from the Cancer Wars
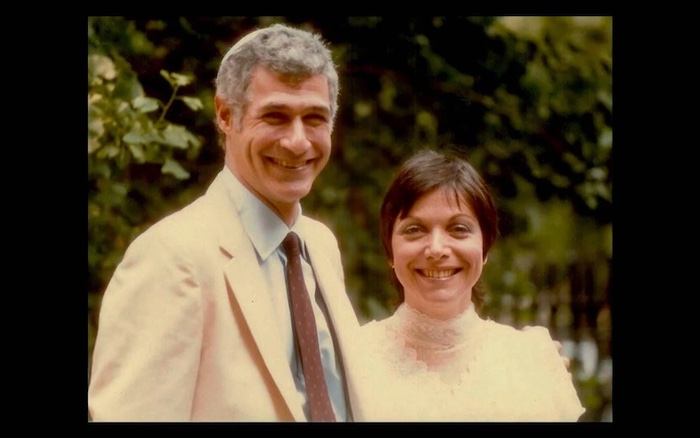
The emotional and physical toll on both of us during our last year together
By Leida Snow
Everybody has a sell-by date, but some folks know theirs in advance. About a year ago, my husband and I had a meeting with a doctor who was new to us. Nice looking man with an open face. He saw our expectant looks and stopped mid-sentence. Looking at Lou he said, “Has no one mentioned that you have stage 4 cancer?”
No one had. We knew there was an issue. Lou has one kidney from birth, and at his yearly checkup, the kidney specialist said to talk to a cancer doctor. But he didn’t seem overly anxious.
I was grateful that finally someone was speaking truth. The hardest to hear was that Lou had, probably, about a year to live. It was as though someone had taken a very sharp knife and plunged it into my stomach.
The oncologist explained that Lou had cancer cells in his liver, but they were not those expected to be there. They were squamish cells, usually associated with other locations. That meant they had spread (metastasized) from somewhere else. But they didn’t know where they had come from.
A Rare Form of Cancer
Lou has cancer with unknown primary (CUP). It affects 2% to 5% of diagnosed cancers. The doctor’s next words tore at my gut: Because the primary source is unknown, there are no data-based, targeted treatments. In other words, for those with CUP, treatment is a guessing game.
I was grateful that finally someone was speaking truth. The hardest to hear was that Lou had, probably, about a year to live.
We had gotten the news at NYU Langone, a top-flight institution where we see our specialists. The overwhelming advice was to go to Memorial Sloan Kettering (MSK) in New York, the Gold Standard, we were told.
Given the restricted time frame, we expected MSK to build on NYU’s findings. But they had to re-do tests, to validate the results. Over the following months, I swallowed my anger and frustration, as the days filled with tests, biopsies, CT scans, MRIs, x-rays and hours spent waiting. The immunotherapy and chemotherapy had zero effect on killing any disease. I hugged Lou close as he comforted me when I couldn’t control the tears.
Lou suffered all the side effects — extreme fatigue, drug induced lung infection, steroids to deal with that, removal of huge amounts of fluid from his lungs, and, best/worst of all, the loss of over 30 pounds. Lou has never been fat. Now he is emaciated. I try not to show him how scared I am.
Not long ago, I heard a crash in the bedroom to find my 6’2″ formerly strong darling dazed on the floor.
There was the offer of one clinical trial. A hope glimmer. But it had mind-blowing side effects and wasn’t aimed at cancer with unknown primary. Lou decided to pass. I steeled myself to be strong for him.
So now we’ve enrolled in what’s called Home Hospice. It’s basically a space where there is no treatment, but you still hope for a magic bullet. Where I watch my husband become less every day.
Not long ago, I heard a crash in the bedroom to find my 6’2″ formerly strong darling dazed on the floor. Lou said he’d bent over to get his shoes and then started to fall without being able to control what was happening. The wall behind him was blood smeared. He had hit his head.
Feelings of Helplessness
Panic. Heart racing. Cloths to press on his head. An ice pack. The hospice said to do what I was doing. Asked if Lou wanted to go to the hospital. No. Didn’t know if I could get him up. But I did. The cut wasn’t deep, but I thought the bleeding would never stop. On his physician’s advice, Lou is no longer taking Eliquis, a blood thinner.
Last year I wrote an article for Next Avenue that flagged that falls can be the beginning of the end. Now it is shattering, personal knowledge.
I’ve cancelled almost everything. Since hospice, there’s minimal interaction with MSK and the long waits. We had to scrub our last session at MSK’s Center for Integrative Medicine. The acupuncture helped Lou to relax, but he was too exhausted to attempt to go.
A Lonely Road
It didn’t feel right to phone and cancel. I went to the appointment and spoke to the doctor. He counseled me to take care of myself. He asked me to keep in touch. His caring for Lou, and for us as a couple, is something I will always remember.
Lou doesn’t want to spend whatever is left of his life in a hospital, and I want to respect his wishes. My insides churn with helplessness.

My own NYU internist has scheduled a monthly video visit to check up on me, especially since I’ve lost more than 15 pounds unintentionally. And the local rabbi calls this agnostic at least once a week. Some friends have disappeared, but there are those who keep in touch. And, yes, I do have someone I can talk to. But it is a lonely road.
Over a year later, my 87-year-old husband has outlived his prognosis and is a shadow of what he was. But he is here. And I want him here.
Some people get inspired after a diagnosis. They reach for a goal or get everything in order. Lou is frustrated and bored, but he is too worn out to do much of anything. I want things however he wants them.
Mostly, he wants to sleep or read the newspaper or hug me. That’s what I cling to. That he’ll be there to cradle me in his arms me as long as possible. Sometimes we go to the sofa and lie with my head in his lap. Lou believes his job is to take care of me, and some of his distress is that he can’t anymore.
Sleep? Not so much. Exhausted. Deeply. What to do? Besides cry. Besides wish I could do more for this man who’s been my life for over 41 years. Because I can’t imagine my world without him. He’s my rock and my biggest fan, the one whose faith in me is stronger than my own. His all-embracing love is where I am home. Whatever I want to do, wherever I want to go, I want to share those experiences with Lou.
That’s the hardest part of Now. Because I’m with him in this no-man’s land, where we can only cling to each other and wait for the inevitable.
Of course, we would have tried anything, gone anywhere when we first heard Lou’s diagnosis and the medical predictions of our future. But if I’d known then what I know now, I would have encouraged Lou to make a different decision.
Regretting Endless Tests and Treatments
There are cancers that can be targeted. Cancer with unknown primary is not one of those. I hope anyone reading my words never faces what’s in front of us. But if you find yourself in this nightmare, here’s what I would say: Don’t spend whatever time you have going to doctors, submitting to endless tests and treatments, waiting in anonymous rooms filled with distracted, unhappy people. Sitting on uncomfortable chairs, being so vulnerable. Dealing with all-business staff that has all the time in the world, while your time is limited. And waiting. Waiting. Waiting.
If I had known then, what would I have done? I would have gone back to Paris with my husband, or we could have gone to the Broadway shows we missed.
If I had known then, what would I have done? I would have gone back to Paris with my husband, or we could have gone to the Broadway shows we missed. We would have reminded ourselves how lucky we were to be able to walk home from the theater. We could have taken in New York’s magisterial skyline from celebratory dining spots.
Now Lou is beyond tired. His legs give way and he falls, can’t get up. Sometimes I’m not strong enough, and we have to call for help. His MSK doctor says he’s fallen too many times and is not safe at home. Emotional overload. The doctor wants me to move him to an in-patient hospice. Lou knows not being home is a possibility. He is disconsolate.
No. I am not going to rush into anything. Moving furniture to make room for a hospital bed, even though Lou says he won’t use it. Never-ending efforts to schedule health aides. Medicare comes through with 15 – 20 hours a week. We now need 24/7. Trying not to think too far ahead.
Welcome to the third ring of hell. You may have read that because of COVID many health care workers died/changed careers/moved away. At the same time, more and more people need qualified help. Hours are spent trying to figure out what’s possible.
Recently my darling said, “What a terrible burden I’ve put on you.” I thought my heart would crack. “I don’t feel it as a burden,” I said, startled by my truth. What is breaking my heart is the fear that I won’t be able to help him, that I won’t know what the right thing is. Fortunately, the hospice physician and woman covering for him are knowledgable and compassionate.
So far, there is no pain. One blessing among the horrors. But he is suffering, and we are looking at a future of unknown — though not long — length.
Struggles of a Caregiver
As I’m writing this, Lou is visibly deteriorating. He can no longer turn himself easily in bed or rise to a sitting position without help. He can barely stand for a moment with assistance while he is moved from the bed to the wheelchair.
What is breaking my heart is the fear that I won’t be able to help him, that I won’t know what the right thing is.
I can’t imagine how people navigate this without a caring partner, but anyone taking on the caretaker role should know in advance: there is mighty little guidance. It’s learn-on-the-job. Case workers and nurses may or may not be thoughtful and compassionate, but you have to think of the questions to ask because too often no one volunteers information.
Are you willing to stay in because you don’t trust that the aide will keep your loved one safe? Or because the aide didn’t show up? Are you prepared to spend hours of your time trying to find coverage even though the agency assured you they would always be able to come through? Can you handle the blowback when you cancel what isn’t working? Can you deal with the additional cost? Are you prepared for the never-ending laundry? Can you function with catch-as-catch-can sleep, only a few hours each night?
My husband is dying. But he’s not gone yet. A few nights ago, he agreed to the hospital bed. He understood that if I don’t get some sleep, I won’t be able to be there for him. He hates the bed. Misses me at night. I miss him too.
Lou eats little, sleeps at odd hours, is restless at night. The aide has to wake me. Lou’s speech is now slurred. It’s hard to understand him. He is angry. He forgets. He wants the hospital bed and the strange people in the apartment gone. He wants me with him all the time. I am terrified.
Addendum: The Death of My Husband
In the daytime, he dozes, wakes, starts to read the newspaper, dozes, wakes, tries again to read. My plan was to write how I would put my arms around him, wanting him to know how much I love him. I was going to share how he would reach out to put his arms around me, wanting me to know how much he loves me.
On September 17th, Lou slept most of the day and night. He mumbled about wanting to go home. I held his hand, said he was home and I was with him. I used to call him my giant, and I told him that I would still choose him out of all the giants in the world. I said I would always be with him and he would be with me. He smiled, squeezed my hand and moved his lips to kiss me.
The next day, he woke and surprised me, wanting to brush his teeth, shave, shower. The aide helped him into the wheelchair and into the bathroom. Afterwards, I warmed some chicken soup. He reached for it and gulped down almost half a cup. Then he lay back to rest. Suddenly he was gasping for breath. And then he was gone.
I am numb. The aide gently repeats that Lou is not breathing. A convulsion of tears. I thought there were none left. Touching him. Taking his hand. Stroking his forehead. Kissing him. What do I do now? I am lost.
Call the hospice. They will send a nurse to sign the time of death. Call the funeral home. They will come. Then what? Vast emptiness. The rabbi calls and says I have to embrace life. Says that’s what Lou would want. Rationally I know he is right. Somehow, I will find a way. I just can’t imagine how.
This year, for our anniversary, June 27th, we had to cancel reservations at a restaurant with spectacular Manhattan views. Lou said it made no sense to go when he couldn’t eat much. He was devastated to disappoint me.
I said: “We’ll always have Paris.”
Complete Article ↪HERE↩!
Solo Aging
— Who Will Take Care of Me When I’m Dying?

By Joy Loverde
Who will take care of me when I’m old? is the unsettling question that is on the minds of millions of people who are and will be aging alone — the never-married, separated, widowed, and divorced population. Rarely do solo agers, or anyone else for that matter, take this question any further. And they should.
At its core, clients will look to you, the professional, to engage them in open and honest conversations about one of their deepest fears about aging –- dying alone.
Bring Up the Past
As long as I can remember, people are divided into distinct mindsets about preparing for death. Some understand the immediacy of planning for the day they hope will never come, others conclude that having their legal and financial affairs in order is enough of a plan.
Family caregiving plays a significant role in the willingness to plan for death. The experience of caring for our elders, and helping them walk through death’s door, opens our eyes to a variety of end-of-life experiences.
Asking clients about their negative eldercare experiences may serve as an opportunity for you to open up the dialogue about planning for a good death. Former family caregivers are often determined never to let misfortunes happen to them.
Where You Die Matters
When asked about long-term care planning, many people express the desire to remain in their own home for as long as possible. This concept is referred to as “age-in-place”.
In terms of the quality of this long-term care plan, aging-in-place is a doable solution for solo home dwellers until they find out the hard way that it isn’t. Advertisements enticing residents to install grab bars and motorized stair chairs are not helping matters with their simplistic messaging.
Solo agers may not have the wherewithal to give the age-in-place concept the forethought and planning it requires. For this reason, clients may look to you as a one-stop shop for obtaining trusted referrals. Consider the following resources:
- Aging Life Care Professional: Care managers assist in creating long-term care plans and finding eldercare services. Website: www.aginglifecare.org.
- Independent Board-Certified Patient Advocate: Helps with medical transactions, early discharge, medical interpretations, medical billing, insurance, and complaints about care. This professional acts as a liaison between patients and the health-care team. Website: www.npaf.org.
- Medicare Advisor: Helps understand Medicare and Medicaid, including paying for hospice and palliative care. They also organize medical bills and negotiate coverage for medical services before and after receiving care. Type “Medicare consultant” in the Internet search engine.
- Veteran’s Benefits Consultant: Offers assistance in qualifying for benefits and helps complete digital forms to submit to the Veteran’s benefits office. Type “veteran’s benefits advisor” in the Internet search engine.
Early-Onset Alzheimer’s: The Value of Knowing
Dementia is designated “early onset” when it affects people of working age, usually between 30 and 65 years old. If your client is diagnosed with early-onset dementia, there are specific resources to lead them to in order to die a good death:
- National Council of Certified Dementia Practitioners: nccdp.org
- Alzheimer’s Association: alz.org
- The Alzheimer’s Society: alzheimers.org.uk
- To Whom I May Concern®: http://towhomimayconcern.org
- Memory Cafes – are gathering places that offer people a place to laugh and relax. Do an Internet keyword search: Memory café, Alzheimer’s café.
No One Dies Alone
No one is born into this world alone, and in the best of circumstances, no one dies alone. With people living longer than ever before, however, outliving family and friends is a modern-day reality.
Solo agers have the opportunity now to establish relationships with professionals who specialize in death and dying. A comprehensive list of specialists is offered in my book, Who Will Take Care of Me When I’m Old?
One resource in particular is worth a special mention — death midwife, also known as death doula and end-of-life guide. These professionals work in concert with doctors, nurses, and other health-care professionals, but do not replace them. They perform specific tasks — sort medical bills, legal paperwork, manage advance directives — as well as provide spiritual and emotional support at the end of life. They can step in early in the process, helping both the healthy and the terminally ill. Services and fees vary widely. To locate resources, type “death midwife” into your Internet search engine or contact the International End of Life Doula Association (www.inelda.org).
In conclusion, the world is in a dramatically different place than it was a decade ago. And yet, I am hopeful that you will meet the challenges that lie ahead. Partnerships with other professionals will help get you there.
Not only does collaborating with other advisors enhance your business credibility, joining forces is what will ultimately make a real difference in the lives of solo agers everywhere.
(Joy Loverde is a best-selling author and popular public speaker, specializing in keynotes and workshops for family members and professionals in the eldercare industry.)
Complete Article ↪HERE↩!
Dying is a selfish business
Whether you are the dying person or the caregiver, living life to the fullest remains your goal, but somedays it’s just too darn hard. When you are so busy that it doesn’t seem you have time to take a breath, where does living life to the fullest fit into your day? It may just get a minute or two of your time but knowing that your life can change in a nanosecond may help you try just a little harder to fit life into your life.
Hug your child longer, spend a moment with a sunrise or a sunset, say “I love you.” Listen to the last notes of your favorite music on the radio before turning off the car, get out for a walk, or just water your plants and take a walk outside. All will help you seize the moments as they arrive. They are fleeting, so you need to pay attention. Living in the moment takes hard work and practice.
There are many challenges for the dying patient. Some are substantial and overwhelming. A caring physician trained in treating the dying patient may be the source for the best care for the patient. Many physicians are not trained in coping with the dying patient, and this can lead to many miscommunications and discomfort for both the patient and the doctor.
An understanding of the dying patient’s experience should help the physician improve their care of the terminally ill. These physicians are often known as palliative care doctors. The doctors specialize in medical care for people living with a serious illness. This care is focused on providing relief from the symptoms and stress of the illness. The goal being to improve the quality of life for the patient and the family. They can assist with the following six challenges that are common to the dying patient:
1. Pain. Pain and the fear of pain often make the patient’s behavior change at the end of life. Cancer patients rank “freedom from pain” as one of their goals for care. Even though the fear of pain is there, the elderly are often unwilling to report their pain because they believe it is a normal symptom of aging and that their pain is directly associated with the worsening of their illness.
2. Depression. The presence and severity of clinical depression often correlates with the severity of physical illness and, in some, a progressive inability to get out of bed. A decreased appetite may also suggest major depression. Anxiety commonly co-exists with depression, and it may be driven by fears of helplessness, a loss of control, abandonment, or pain.
3. Coping. Patients with advanced illness face the challenge of coping with their disease daily. While some patients demonstrate optimism, practicality, resourcefulness, awareness, and flexibility, others present with a variety of defensive styles in response to their diagnosis. These defenses can be denial and non-compliance, which can lead to a delay in treatment.
4. Dignity. For dying patients, maintaining dignity is foremost in their care, broadly defined in terms of being worthy of honor, respect, and esteem. For many patients, dignity is directly related to the level of independence retained through the course of illness.
5. The need for control. For some terminally ill patients, maintaining a sense of control is a central task of the dying process. This need for control is prominent among patients who request physician-assisted suicide (PAS) in Oregon. These patients were universally described as having strong personalities; they were determined and inflexible, and they wanted to control both the timing and the manner of their deaths.
6. Other aspects of the dying process. Dying patients and their families often must deal with complicated “practical” issues, such as financial problems and legal issues. These seemingly mundane concerns can cause a great deal of distress for dying patients and their families. It’s a good idea to take care of the difficult things while the dying person can make decisions. Wills, trusts, burial requests, and choosing a grave site can be taken care of while the person is well, so the decisions are not made after the death.
While nature is selfish, you don’t need to be. You might find that your best friend is yourself. You know when you need a hug or when it’s time to rest or try to appreciate the moment you are in. You also know when you are at the end of your rope and need to walk away, so things don’t blow up and get out of proportion.
There are five regrets the dying person often have when it is too late to do anything to change them. There is still time, if you can try and make some small changes now, so your regrets are fewer in the end.
1. I wish I’d had the courage to live a life true to myself, not the life others expected of me. This seems to be a very common regret when people realize that their life is almost over and look back on it. Many dreams when unfulfilled due to choices they made or did not make. When we are healthy, it’s hard to realize that a decision now, which we may only be allowed to make once, can change our life forever. Time may run short, and the chance won’t come up again.
2. I wish I hadn’t worked so hard. This regret is more common with men than women. Or it used to be. Since men are often the primary source of income, they regret what they missed while working. Time with children and spouse being the main regret. This is changing now that women are a strong force in the workplace. The working mother who has a child and goes back to work right away may eventually regret the lost time with the child as an infant.
3. I wish I’d had the courage to express my feelings. Suppressing one’s feeling to keep peace with others may result in a mediocre existence and prevent the person from becoming the person they were truly capable of being. Illnesses can result from this, and one may never realize the cause. Mental health is as important as physical health. Bottling up emotions and thoughts is hard on one’s psyche.
4. I wish I had stayed in touch with my friends. There are many deep regrets over lost friendships. Getting caught up in one’s day-to-day life makes it easy to let friends slip away. Waiting until the end of life is way too late to try and track old friends down.
5. I wish that I had let myself be happier. Many people do not realize that happiness is a choice. We get comfortable in the way we live our lives and don’t realize that happiness is easy to come by if we just work at it a little and let it in the front door. Fear of change makes people pretend they are happy, but truly they are not. A good laugh and some silliness won’t hurt anyone.
Complete Article ↪HERE↩!
How Advance Care Planning Neglects Black Americans
— Researchers are rethinking living wills and other ACP documents to ensure seriously ill patients get the care they want.

When Kevin E. Taylor became a pastor 22 years ago, he never expected how often he’d have to help families make gut-wrenching decisions for a loved one who was very ill or about to die. The families in his predominantly Black church in New Jersey often didn’t have any written instructions, or conversations to recall, to help them know if their relative wanted — or didn’t want — certain types of medical treatment.
So Taylor started encouraging church members to ask their elders questions, such as if they would want to be kept on life support if they became sick and were unable to make decisions for themselves.
“Each time you have the conversation, you destigmatize it,” said Taylor, now the senior pastor at Unity Fellowship Church NewArk, a Christian church with about 120 regular members.
Taylor is part of an initiative led by Compassion & Choices, a nonprofit advocacy group that attempts to encourage more Black Americans to consider and document their medical wishes for the end of their lives.
End-of-life planning — also known as advance care planning, or ACP — usually requires a person to fill out legal documents that indicate the care they would want if they became unable to speak for themselves because of injury or illness. There are options to specify whether they would want life-sustaining care, even if it were unlikely to cure or improve their condition, or comfort care to manage pain, even if it hastened death. Medical groups have widely endorsed ACP, and public awareness campaigns have promoted the practice.
Yet research has found that many Americans — particularly Black Americans — have not bought into the promise of ACP. Advocates say such plans are especially important for Black Americans, who are more likely to experience racial discrimination and lower quality care throughout the health care system. Advance care planning, they say, could help patients understand their options and document their wishes, as well as reduce anxiety for family members.
However, the practice has also come under scrutiny in recent years as studies reveal that it might not actually help patients get the kind of care that they want at the end of life. It’s unclear whether those results are due to a failure of ACP itself, or due to research methods: Comparing the care that individuals said they want in the future with the care they actually received while dying is exceedingly difficult. And many studies that show the shortcomings of ACP look at predominantly White patients.
Still, researchers maintain that encouraging discussions about end-of-life care is important, while also acknowledging that ACP either needs improvement or an overhaul. “We should be looking for, OK, what else can we do other than advance care planning?” said Karen Bullock, a professor of social work at Boston College, who researches decision making and acceptance around ACP in Black communities. “Or can we do something different with advance care planning?”
Advanced care planning was first proposed in the U.S. in 1967 when the now-defunct Euthanasia Society of America advocated for the idea of a living will — a document that would allow a person to indicate that they wouldn’t want to be kept alive artificially if there were no reasonable chance of recovery. By 1985, most states had adopted living will laws that established standardized documents for patients, as well as protections for physicians who complied with patients’ wishes.
Over the last four decades, ACP has expanded to include a range of legal documents, called advance directives, for detailing one’s wishes for end-of-life care. In addition to do-not-resuscitate, or DNR, orders, patients can list treatments they would want and under which scenarios, as well as appoint a surrogate to make health care decisions for them. Health care facilities that receive Medicare or Medicaid reimbursement are required to ask patients about advance directives and provide relevant information. And in most states, doctors can record a patient’s end-of-life wishes in a form called a physician order for life-sustaining treatment. These documents require that patients talk with their physician about their wishes, which are then added to the patient chart, unlike advance directives, which usually consist of the patient filling out forms themselves without discussing them directly with their doctor.
Many people simply aren’t aware of ACP, or don’t fully understand it. And for Black individuals, that knowledge may be especially hard to come by.
But as far as who makes those plans, studies have shown a racial disparity: In a 2016 study of more than 2,000 adults, all of whom were over the age of 50, 44 percent of White participants had completed an advance directive compared with 24 percent of Black participants. Meanwhile, a 2021 analysis of nearly 10,000 older adults from a national survey on aging found that Black Americans were 57 percent less likely than White Americans to have a health care surrogate.
Many people simply aren’t aware of ACP, or don’t fully understand it. And for Black individuals, that knowledge may be especially hard to come by: Several studies have found that clinicians tend to avoid discussions with Black and other non-White patients about the care they want at the end of life because they feel uncomfortable broaching these conversations or unsure whether patients want to have them.
Other research has found Black Americans may be more hesitant to fill out documents because of a mistrust of the health care system — rooted in a long history of racist treatment. “It’s a direct, in my opinion, outcome from segregated health care systems,” said Bullock. “When we forced integration, integration didn’t mean equitable care.”
Religion can also be a major barrier to ACP. A large proportion of Black Americans are religious, and some say they are hesitant to engage in ACP because of the belief that God, rather than clinicians, will decide their fate. That’s one reason why programs like Compassion and Choices have looked to churches to make ACP more accessible. Numerous studies support the effectiveness of sharing health messages in church — from smoking cessation to heart health. “Black people tend to trust their faith leaders, and so if the church is saying this is a good thing to do, then we will be willing to try it,” Bullock said.
But in 2021, an article by palliative care doctors laid bare the growing evidence that ACP may be failing to deliver on the promise to get patients the end-of-life care they want, also known as goal-concordant care. The paper summarized the findings of numerous studies investigating the effectiveness of the practice and concluded that “despite the intrinsic logic of ACP, the evidence suggests it does not have the desired effect.”
For example, while some studies identified benefits such as increasing the likelihood of a patient dying in the place they desired and avoiding unwanted resuscitation, many found the opposite. One study found that seriously ill patients who prioritized comfort care in their advance directives spent just as many days in the hospital as patients who prioritized life-extending experiences. The authors of the 2021 summary paper suggested several reasons that goal-concordant care might not occur: Patients may request treatments that are not available, clinicians may not have access to the documentation, surrogates may override patients’ requests.
A pair of older studies suggested these issues might be especially pronounced for Black patients. They found that Black patients with cancer who had signed DNR orders were more likely to be resuscitated, for example. These studies have been held up as evidence that Black Americans receive less goal-concordant care. But Holly Prigerson, a researcher at Cornell University who oversaw the studies, noted that they investigated the care of Black participants who were resuscitated against their wishes, and in those cases, clinicians did not have access to their records.
In fact, one issue facing research on advance care planning is the fact that so many studies have focused on White patients, giving little insight into whether ACP helps Black patients. For example, in two recent studies on the subject, more than 90 percent of patients were White.
“It’s a direct, in my opinion, outcome from segregated health care systems,” said Bullock. “When we forced integration, integration didn’t mean equitable care.”
Many experts, including Prigerson, agree that it’s important to devise new approaches to assess goal-concordant care, which generally relies on what patients indicated in advance directives or what they told family members months or years before dying. But patients change their minds, and relatives may not understand or accept those wishes.
“It’s a very problematic thing to assess,” said Prigerson. “It’s not impossible, but there are so many issues with it.”
As for whether ACP can manage to improve end-of-life care specifically in areas where Black patients receive worse care — such as inferior pain management — experts, such as Bullock, note that studies have not really explored that question. But addressing other racial disparities is likely more critical than expanding ACP, including correcting physicians’ false beliefs about Black patients being less sensitive to pain, improving how physicians communicate with Black patients, and strengthening social supports for patients who want to enroll in hospice.
ACP “may be part of the solution, but it is not going to be sufficient,” said Robert M. Arnold, a University of Pittsburgh professor on palliative care and medical ethics, and one of the authors of the 2021 article that questioned the benefits of ACP.
Many of the shortcomings of ACP — from the low engagement rate to the unclear benefits — have prompted researchers and clinicians to think about how to overhaul the practice.
Efforts to make the practice more accessible have spanned creating easy-to-read versions, absent any legalese, and short, simple videos. A 2023 study found that one program that incorporated these elements, called PREPARE For Your Care, helped both White and Black adults with chronic medical conditions get goal-concordant care. The study stood out because it asked patients who were still able to communicate if they were getting the medical care they wanted in-the-moment, rather than waiting until after they died to evaluate goal-concordant care.
“That to me is incredibly important,” said Rebecca Sudore, a geriatrician and researcher at the University of California, San Francisco, who was the senior author of the study and helped develop PREPARE For Your Care. Sudore and her colleagues have proposed “real-time assessment from patients and their caregivers” to more accurately measure goal-concordant care .
“Sometimes it’s awkward,” Taylor said. “But it’s now awkward and informed.”
In the last few years, clinicians have become more aware that ACP should involve ongoing conversations and shared decision making between patients, clinicians, and surrogates, rather than just legal documents, said Ramona Rhodes, a geriatrician affiliated with the University of Arkansas for Medical Sciences.
Rhodes and her colleagues are leading a study to address whether certain types of ACP can promote engagement and improve care for Black patients. A group of older patients — half are Black and half are White — with serious illnesses at clinics across the South are receiving materials either for Respecting Choices, an ACP guide that focuses on conversations with patients and families, or Five Wishes, a short patient questionnaire and the most widely used advance directive in the U.S. The team hypothesizes that Respecting Choices will lead to greater participation among Black patients — and possibly more goal-concordant care, if it prepares patients and families to talk with clinicians about their wishes, Rhodes said.
When Taylor talks with church members about planning for end-of-life care, he said they often see the importance of it for the first time. And it usually convinces them to take action. “Sometimes it’s awkward,” he said. “But it’s now awkward and informed.”
Complete Article ↪HERE↩!
Study Finds Gap Between What Rural Residents Want for End-of-Life Care and What They Receive
— Lack of conversations among the family members, and a more difficult access to healthcare are among the reasons responsible for the discrepancy.

By Liz Carey
When it comes to end-of-life wishes, a new study has found that while most people have end-of-life wishes, only a little over a third of them actually get them fulfilled. That is even more true with rural residents, researchers said.
Lula Reese said she didn’t have to ask her mother what she wanted as she neared the end of her life – she just knew.
“She told us she didn’t want to live with any of her children,” Reese said of her mother, Lula Simms. “She didn’t want to be a burden on any of us. We never talked about what she wanted. We just knew.”
Lula Simms lived in rural Bastrop, Texas , population 10,434, all her life and turned 100 in November, 2022. For the last two years of her life, her eight children cared for her in her own home with the help of hospice.
“She was in hospice for two years,” Reese said. “One day, she was different – she had stopped eating and she wasn’t the same. We took her to the hospital, and they told us she was transitioning.”
Simms died in February 2023, just a few days after her children rushed her to the hospital. For Reese, making sure that her mother’s wishes regarding the end of her life was never something that was written down. It was just something the family knew – her mother wanted to stay in her own home as long as he could. With the help of hospice, her family was able to make sure those wishes were met.
A new study from St. David’s Foundation in Texas has found that when it comes to end-of-life care, most Texans want to die at home (76%), and to not be a burden to their family (77%). But only one in three people surveyed said their loved one’s wishes were honored. Of those who are least likely to have their end-of-life wishes followed are rural residents, the study found.
Only 37% of the survey respondents said their loved ones died at home. Close to half of them (47%) said their loved one faced challenges related to their care – from problems with insurance coverage to facing cultural or language barriers.
Andrew Levack, senior program director with St. David’s Foundation, said there are a number of reasons why ensuring a rural loved one’s wishes are met may be difficult. Key among them is that conversations about the end of life just don’t take place.
“I think a big part of it is that those conversations and that planning around how to make (end-of-life wishes) happen don’t necessarily take place,” he said in an interview with the Daily Yonder. “One of the interesting things the study found was how few conversations respondents had with their doctors around plans for end of life. I think people have an idea of what they would like, but it takes some active planning and advocacy to make that happen. In the absence of that, I think people don’t realize what their ideal scenario would be.”
Dr. Kate Tindell, medical director for Austin Palliative Care and Hospice, said most of the hospice referrals her program has come from hospitalizations. That presents a problem for rural residents who are further away from hospitals and more isolated, she said.
“The rural community I think tends to already have limited exposure to health care,” she said in an interview with the Daily Yonder. “I think (the Covid-19 pandemic) really compounded that for them. Rural communities were suffering from the closure of healthcare access. The strain on health care from Covid makes it feel like we’re seeing them have less and less access.”
Lack of access can lead to a less intimate relationship between patient and doctor who could discuss hospice with an elderly patient.
“People have really disjointed health care now,” she said. “We’ve sort of lost that sense that there is a captain of the medical ship who is aware of all the moving parts and is giving the patient that guidance. I think that really causes people to not have the kind of relationship that would allow them to have that kind of conversation (about end-of-life wishes) the way they would if they had seen the same provider every single time for 10 years.”
Sometimes, it falls to non-profit organizations to get information about making end-of-life decisions to older rural residents. Sumai Lokumbe, is one of Bastrop’s OWLs – or Old Wise Leaders. She works with the aging population in her area to make sure they get the care they need. Many people in her community are unaware of what hospice and palliative service is or have a misunderstanding about what end-of-life care entails.
“I explain to people exactly what hospice does and what it is,” she said in an interview with the Daily Yonder. “They come in to make sure you’re not in pain and make you comfortable and take some of the stress off the family members, plain and simple.”
In some instances, cultural differences create challenges to overcome. Many African Americans in her area face cultural beliefs that prevent them from having anyone but family care for loved ones as they age. Other African American community members may distrust a system that has previously not cared for them.
“In the African American community especially, there is a belief that you stay with your family,” she said. “But there’s also a lot of distrust of the system. They don’t have a lot of trust in things put in place for them by people who don’t look like them.”
For Lula Reese, hospice was a way for her family to care for her mother as she transitioned through the end of her life.
“We had heard of hospice, but we used to always think that hospice care meant that she was going to pass away in the next five or six days,” Lula Creek said. “But we learned that wasn’t the case… Hospice and helped us take care of her, like giving her baths and bringing her supplies when she ran out.”
Even without those final wishes in writing, the family was able to keep her in her home as long as possible, she said. Hospice helped them to care for their mother, as well as alleviate financial burdens they know she would have feared placing on them.
“We didn’t talk to her about hospice care, and you know, we didn’t talk to her about what she wanted to do in her last days, ” she said. “We didn’t find out about it until after we had her service. She had already written that her desire was just to live long enough to see her children be grown. Her youngest child is in their fifties, so she had everything she wished for. We never asked her if she wanted to go into a nursing home. We just knew that was not her desire.”
Complete Article ↪HERE↩!
My three-point turn toward personalizing good death in old age
By Marcel G.M. Olde Rikkert
It was New Year’s Eve, and my wife and I were visiting my father in his long-term care apartment. He had been cautiously wandering around, waiting for a visit, when we arrived, something he’d been doing since my mom had died a year ago. He looked frail. The “surprise question” occurred to me: Would I be surprised if he passed away in the next year?
No. I wouldn’t.
After we’d spent some time together, I asked his wishes for the coming year.
“I don’t know,” he replied. “I’m 101 years old. I was married nearly 70 years and have finished my life. Marcel, I am very much afraid of dying. Will you ensure that I don’t suffer and that dying won’t take too long?”
I promised him I would try.
The second week of January, I received a call that my father had fallen and was in pain. He had no fracture, but he insisted he did not want to get up anymore. I drove the 120 km to his home, thinking about all of the possible scenarios. My first thought was to get him on his feet again, with enough analgesics to overcome his fear of falling. As a geriatricianson, I had always tried to keep my parents active and felt proud that they had enjoyed so many years together this way.
But would such encouragement fit the situation my dad was in now? He’d asked me to make sure dying didn’t take too long. Was it already time to consider death by palliative sedation? I felt uncertain. To qualify, he needed a symptom that could not otherwise be helped, and death had to be expected within two weeks.
When I arrived at his bedside, he repeated, “I don’t want to get up anymore,” and again, he asked me to help alleviate his fear of dying. I had to honour his heartbreaking request for a peaceful death. With a leaden soul, I went to the doctor on call — luckily his own physician — and asked for his assistance in ensuring a peaceful death. We discussed all options, acknowledging my father’s increasing frailty, despair and anxiety, and we agreed to start acute palliative sedation with midazolam, adding morphine according to the Dutch national protocol. I watched as the doctor prepared the equipment, feeling reassured by his calm professional acts.
My father could not understand the plan himself, but after an hour or so he woke for a few seconds and, with a frail smile, said goodbye to my sisters and me. We made a schedule for staying with him and I took the first turn. I sat next to him for two hours, and just after his second dose of morphine, he stopped breathing and passed peacefully away, just as he had wished. Sadness and relief turned to warm gratitude in my heart. Life had given us a sensitive and wise physician who enabled us to overcome what my dad and I had feared most.
***
In December of the same year, my 86-year-old father-in-law asked me to come to Antwerp and talk to him about the options for assisted dying. He had metastatic prostate cancer and had not recovered over six weeks of hospital care. He was bedridden with a toe infection and painful pressure sores. My reflex, again, was to involve geriatricians and try to get him on his feet. However, my father-in-law, an engineer by profession, had decided it was time to turn off his engine after losing hope for sufficient recovery. My wife and I explained to him what medical assistance in dying and palliative sedation could look like, as both are allowed under certain conditions in Belgium.
Without hesitation, he chose medical assistance in dying. He was very satisfied with his life, having experienced war, liberation, marriage, births, retirement and nice family holidays. In line with his story of life, he did not want to deteriorate further and end his life in pain and misery. We kept silent while he wrote his last will, then thanked us for everything and suggested we should now watch the Belgium versus Morocco World Cup soccer match.
When the game ended, saying goodbye was hard. We looked into his eyes, still bright, and shook his hands, still strong. We knew it was the last time. But his calm smile wordlessly assured me it was time to turn off my own geriatrician’s inclination to pursue mobility and functional improvement. Death was made possible within a week, and after ensuring that all requirements were met and speaking to each family member, his oncologist carried out the procedure carefully in the presence of his children.
***
Just two weeks later, our Spanish water dog, Ticho, made me reflect again on what’s needed most at the end of a long life. For 16 years, Ticho had been my much-loved companion and daily running mate. I had begun to dream he might become the world’s oldest water dog. However, his sad eyes now showed me that his life’s end was close, also evidenced by having nearly all possible geriatric syndromes: slow gait, repeated falls, sarcopenia, cataract, dementia, intermittent incontinence and heart failure.
Still, he came with me on short walks until, one day, he became short of breath, started whimpering and did not want me to leave him alone. Patting calmed him a bit, but I realized we needed to help him die peacefully instead of trying to mobilize him again. Though not comparable to the last days of my dad and father-in-law, there were echoes.
Our three adult kids rightly arranged a family meeting, as Ticho was their sweet teddy bear. We agreed to consult a veterinarian and ask for help with a good farewell. Next morning, the vet agreed with assisting dying. She said Ticho was the oldest dog she had seen so far, and she reassured us that it was the best decision we could make. Again, I felt very thankful for this professional and compassionate help. Ticho died peacefully after sleep induction and, together, my son and I buried him in our garden.
***
Strangely, although death in old age is as natural as birth is for babies, pediatricians seem much more involved in deliveries than geriatricians are in dying. These three encounters with death in my life made me feel I had fallen short so far as a doctor, having undervalued assisting dying at old age. How to guide people to a better end of life was largely left out of my training as a geriatrician. Like pediatricians, geriatricians prefer to embrace life. In geriatric practice and research, we tend to reach for the holy grail of recovery by improving functional performance and autonomy to enhance well-being for frail older people, rather than focusing on facilitating their well-being over their last days. In this tradition, I practised hospital-based comprehensive geriatric assessment and integrated care management, as this had proven effective in giving older people a better chance of discharge to their own homes.
In my research, I had steered a straight line toward longevity and improving autonomy, in accordance with the dominant culture in society and medicine. I had excluded older people with short life expectancies from our intervention trials and did not adapt outcomes to this stage of life. Even for our recently updated Dutch handbook on geriatrics, we did not describe death or dying in any detail. I served many older people in their last days and hours, but did so with limited experience, few professional guidelines and little legal leeway.
Now, having been helped so compassionately with the deaths of three beings close to me, I realize how rewarding it can be to switch clinical gears from recovery-directed management to dying well, and to do so just in time. Older people can show and tell us when they arrive at this turning point and are ready for ending life. I hope other physicians will realize, as I have, how important it is to allow death into a conversation, even a care plan, and to be adequately trained to do so. Perhaps we also need our own turning points as physicians to get ready for the delicate responsibility of compassionate and professional assistance in personalizing good death in old age.
Complete Article ↪HERE↩!