But according to some health experts, one of the most critical health inequities among L.G.B.T.Q. adults often goes overlooked.
A mounting body of research shows that L.G.B.T.Q. adults are more likely to have worse heart health than their heterosexual peers. Lesbian, gay and bisexual adults were 36 percent less likely than heterosexual adults to have ideal cardiovascular health, the American Heart Association concluded in 2018, based on surveys of risk factors like smoking and blood glucose levels. In 2021, the organization released a statement on the high rates of heart disease among transgender and gender diverse individuals, linking these elevated rates in part with the stress that comes from discrimination and transphobia.
The data supports what clinicians, and those who research L.G.B.T.Q. health, have observed for decades — that the community faces particular, pervasive obstacles that take a toll on the brain and body.
Cardiovascular disease is the leading cause of death in the United States. The Centers for Disease Control and Prevention estimates that 80 percent of premature heart disease and strokes are preventable. But there are disparities in where this burden falls among the general population. We spoke to doctors and health researchers about why these inequities persist, and what steps L.G.B.T.Q. adults can take to bolster their heart health.
Stress directly impacts certain hormones that regulate your blood pressure and heart rate, said Billy Caceres, an assistant professor at the School of Nursing and the Center for Sexual and Gender Minority Health Research at Columbia University.
Hypervigilance — the sense of always being on edge, constantly scanning for the next threat — causes cortisol levels to surge, which can lead to long-term cardiovascular issues, said Dr. Carl Streed, an assistant professor at Boston University School of Medicine.
Plus, stress can lead to chronic inflammation, said Dr. Erin Michos, associate director of preventive cardiology at Johns Hopkins University School of Medicine, and it can raise your blood pressure and heart rate.
Researchers sometimes refer to the allostatic load, the cumulative toll that chronic stress takes on the brain and body, said Scott Bertani, the director of advocacy at HealthHIV, a nonprofit focused on advancing prevention and care for people at risk for H.I.V. “It only stands to reason that our bodies respond to these really complex and challenging life events and demands,” he said. For instance, he added, the act of coming out, and in some cases, coming out repeatedly, often comes with severe stress.
To cope with the constant threat of discrimination or harassment, many in the L.G.B.T.Q. community self-medicate with drugs like tobacco and alcohol, said Dr. Streed, who is also a researcher at the Center for Transgender Medicine and Surgery at Boston Medical Center. These industries have targeted the L.G.B.T.Q. community through advertising, he said, especially during Pride month. The Centers for Disease Control and Prevention reports that around 25 percent of lesbian, gay or bisexual adults used a commercial tobacco product in 2020, compared with 18.8 percent of heterosexual adults, a disparity the agency partially attributes to the tobacco industry’s long history of aggressive marketing campaigns.
Research has also identified a link between sleep and heart health, Dr. Caceres said. Mounting evidence shows that L.G.B.T.Q. adults experience more sleep issues and interruptions than the general population, which may also be tied to chronic stress.
Obstacles to seeking care
A 2017 survey of nearly 500 L.G.B.T.Q. adults by researchers at Harvard T.H. Chan School of Public Health and the Robert Wood Johnson Foundation found that more than one in six reported avoiding health care because they worried about discrimination. That hesitancy means that L.G.B.T.Q. adults are less likely to access potentially lifesaving preventive health care, said Dr. Michos. All adults should be screened at least once a year for cardiovascular risk factors, which is typically part of an annual physical, she said.
Finding medical providers that you feel comfortable and safe around can be key in preventing heart disease, experts said. Dr. Streed recommends that L.G.B.T.Q. adults seek out supportive medical practitioners. The Gay and Lesbian Medical Association offers a directory on its website that allows patients to find health professionals. The Human Rights Campaign creates an annual Healthcare Equality Index — a list of health care facilities that say they are inclusive of L.G.B.T.Q. patients.
What L.G.B.T.Q. adults should know about improving heart health
While gender-affirming hormones have been shown to positively impact mental health, Dr. Michos said, there is some evidence that high amounts of testosterone and estrogen can have cardiovascular risks. People who are taking these hormones should consult their doctors about how to maintain their heart health.
The American Heart Association recommends seven steps for optimal heart health: managing blood pressure, keeping cholesterol levels low, reducing blood sugar, exercising daily, eating a nutritious diet, maintaining a healthy body weight and not smoking. Dr. Michos also recommended minimizing consumption of processed foods, sugar-sweetened beverages and highly refined carbs, instead opting for whole grains, lean proteins, and plenty of fruits and vegetables. Adults should also aim for at least 30 minutes of moderate-intensity exercise each day, like brisk walking, jogging or cycling.
These are critical facets of preventing heart disease, she added, “but we can’t just preach ‘You need to live a healthy lifestyle’ if individuals are under significant psychological distress and discrimination.”
Social support can help buffer against the physical and psychological strain of stress, she said, and seeking out community can be particularly crucial for L.G.B.T.Q. health outcomes. Several organizations can help L.G.B.T.Q. people connect with one another: SAGE, a nonprofit focused on aiding older adults, matches volunteers with L.G.B.T.Q. people over the age of 55 for weekly phone calls. The Trevor Project, which provides crisis intervention and suicide prevention services to L.G.B.T.Q. young people, also offers an online community for those between 13 and 24. The Bisexual Resource Center, a nonprofit focused on bisexual issues, maintains a list of online and in-person support groups for bisexual people.
“L.G.B.T. health isn’t just about H.I.V. prevention,” Dr. Caceres said. “A lot of the time, it ends up being focused on that. Sexual health is not the only dimension of health that we as queer people should be thinking of.”
Despite tens of thousands of MAID deaths and concerns over expanding eligibility for medical assistance in dying, little has been said about how people die. Here’s what we know
Death by doctor-administered lethal injection is the primary form of delivery of assisted death in this country.
In the final moments before pushing the syringe, Dr. Chantal Perrot will pause and ask a final time: “The medications I’m going to give you will cause your death. Is this what you want?” The Toronto family doctor has been providing medical assistance in dying (MAID) since the act was decriminalized in Canada in 2016. Together, she and those colleagues across Canada willing to help end a life have presided over more than 21,000 deaths. Twenty-one thousand people who responded: “Yes. This is what I want.”
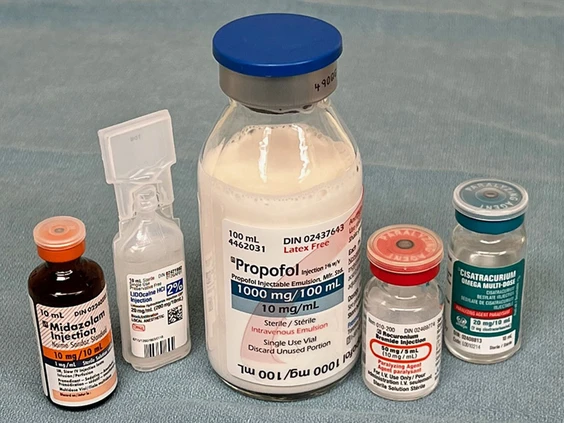
People fall asleep with the first sedative, Perrot said. Lidocaine comes next, to help numb the vein and prepare it for the third injection, propofol, which puts people into a deep coma. Propofol can sting as it flows through a vein. Lidocaine, what dentists use for freezing, can help reduce any burning sensation.
“When I’m providing the medications, I’m looking at their faces and I’m holding their hands,” Perrot said. She has a finger on their pulse. Soon, there is no movement, no response, she said. Many of the people who seek her help to die are weak and frail, and the doses of drugs so large that death occurs quickly, she said. Five minutes, eight minutes at most.“I have seen absolutely no suffering,” she said.
The medications I’m going to give you will cause your death. Is this what you want?
Dr. Mark Bonta’s medical assistance in dying team has been involved in just over 200 MAID “interventions.” It is their collective experience as well, Bonta wrote in an email, that death by lethal injection is “one of a peaceful transition to the afterlife without any witnessed suffering.”
“Not once has a member of our care team approached me to discuss concerns they had around the patient’s comfort during the procedure,” said Bonta, an internal medicine specialist at Toronto General Hospital who oversees a team responsible for covering six sites across Toronto.
Peaceful, calm, serene, beautiful. Even elegant. All are words providers and family witnesses have used to describe MAID.But how can doctors be certain death is peaceful to the person dying?
Despite tens of thousands of MAID deaths, and concerns over the ever-expanding eligibility criteria, little has been said about how people die, including the drugs and heavy doses used to kill, the sequence in which they’re injected, and what they do to the body.
Canadian senators studying Canada’s new MAID law, Bill C-7, last year heard alarming testimony from Dr. Joel Zivot, an anesthesiologist and critical care doctor at Emory University School of Medicine in Atlanta, Ga., who was born in Winnipeg and went to medical school there and who forwarded the suggestion that death by MAID, he suspects, could feel like drowning.
Dr. Joel Zivot, an anesthesiologist and critical care doctor at Emory University School of Medicine in Atlanta, Ga.
Once the paralyzing drugs are used, the person can no longer move. “All bets are off,” Zivot said. “The outward appearance of calm and peacefulness is not really an evaluation as to what the interior experience of the person that is dying would necessarily have,” he told senators. “It doesn’t mean anything that outwardly it looks peaceful.”
“Canada has vaulted itself to the unenviable front of the line for this,” Zivot said in an interview with National Post. “I think my work is pretty close enough to what is happening in Canada that it warrants some circumspection, and that’s all I’m asking for.”
Zivot is a lifelong campaigner against capital punishment. His work involves studying autopsies of prisoners killed by lethal injection in the U.S. But these executions involve, except for one common sedative, different medications than those used in doctor-administered MAID in Canada. Bonta and other MAID providers say Zivot, who has never performed or witnessed MAID himself, is dead wrong, that his assumptions aren’t anchored in any published evidence and that it’s irresponsible to extrapolate findings from the autopsies of executed prisoners and claim they could be seen in the context of MAID.
In Canada, the law no longer restricts MAID to people whose death is reasonably foreseeable. As of next March, people whose sole underlying condition is a mental illness will also be eligible for assisted death. A joint parliamentary committee is studying whether MAID criteria should be further expanded still, to include mature minors and advance requests.The latest annual report on medically assisted deaths, which covers deaths in 2021, is due in July. As of the end of 2020, 21,589 MAID deaths had been reported in Canada. In 2020, there were 7,595 cases, accounting for 2.5 per cent of all deaths, and a 34 per cent increase over 2019.
Fewer than seven involved self-administered MAID, whereby the person swallows a doctor-prescribed lethal cocktail of drugs. The “oral protocol” isn’t legal in Quebec. Nova Scotia only recently made it available. It’s not popular for several reasons, including a higher rate of complications, longer, drawn-out deaths, and a higher failure rate. High-dose barbiturates are the drugs most used, compounded into a sweet liquid formulation that needs to be swallowed within a certain number of minutes so that it reaches peak levels. If people have trouble swallowing because of gut problems caused by disease, if they regurgitate, it can mean incomplete doses that fail to kill. Death can be prolonged, taking up to 10 hours. Even when properly absorbed, time-to-death can be highly unpredictable, according to a recent review. Most provinces require that a doctor or nurse practitioner be present with an IV back-up kit in case death doesn’t occur “within an agreed upon time.”
The vast majority will choose intravenous, because it’s faster and more predictable
Death by doctor-administered lethal injection is the primary form of delivery of assisted death in this country. “The vast majority will choose intravenous, because it’s faster and more predictable,” Perrot said.
When Bill C-14 came into effect, there was no consensus on how to perform euthanasia — which drugs to use, in what order. The law heralded a once unimaginable situation for doctors, a revolution in medicine that allowed doctors trained to support life to perform what was once forbidden.
MAID essentially involves administering an overdose of an anethestic used all the time in surgery, but unlike surgery, no one is supporting the breathing and the heart. Until MAID, doctors had never given doses this big.
Two years ago, the Canadian Association of MAID Assessors and Providers, CAMAP, published a paper on recommended drug protocols.The protocol recommends pre-filled syringes, inserting IV lines into as large a vein as possible and rapid injection of the drugs, in rapid succession, for a more rapid death. Once final consent is provided, the first injection is midazolam, a Valium-like sedative that makes people sleepy and calms their nerves and that has also been shown to block the formation of memories. Then lidocaine, followed by propofol, which is white and oily, milky looking, is given in a dose more than 10 times what would normally be used to put people under for surgery. Finally, a muscle relaxant, usually rocuronium, in a dose three to four times the normal amount. At that dose, rocuronium stops the muscles of the lungs from working, which stops the heart from working.
The sequence of death is coma, respiratory arrest (the person stops breathing) followed by cardiac arrest.Two IV lines are usually started, so that there’s a back-up if one gets “lost,” or slips out of the vein, causing the drugs to leak into surrounding tissue.
When doctors try to push large volumes of propofol through a peripheral vein, the vein sometimes bursts from the pressure. Some hospitals mandate a PICC line, a peripherally inserted central catheter that’s inserted by a radiologist or other expert. It’s a longer line that gets to a larger vein with higher blood flows, so there’s less chance of losing IV access.
Propofol makes people unconsciousness. It basically shuts down the brain. It depresses the central nervous system and, at high doses, decreases blood flow to the brain, and the rate of oxygen consumed by the brain, putting people into a deep coma.
Not once has a member of our care team approached me to discuss concerns they had around the patient’s comfort
The onset of action is roughly 40 seconds. “Often the mouth will fall open as the jaw muscles relax,” according to the MAID assessors and providers website. Some people snore. The large dose will also cause cardiovascular collapse. Blood pressure plummets, the heart rate slows. Often by the time he’s finished injecting the propofol, the heart itself has all but stopped pumping, said Dr. James Downar, a specialist in palliative and critical care at the University of Ottawa. “The dose of propofol we give is so high that by that point, there is usually little to no circulation. Because of the medication itself, and the loss of circulation, the person will be unconscious and stop breathing.
“In my practice, and I believe in most people’s practice, only after they see that the person isn’t making any respiratory efforts and is completely unresponsive, then you use rocuronium,” the muscle relaxant, Downar said.
Propofol can cause involuntary muscle movements including, more rarely, what looks like a very brief seizure. Rocuronium suppresses any movements, including what’s known as agonal reflexes. When people stop breathing and carbon dioxide builds up, acid builds up in the blood, which can cause spasms in the diaphragms. People can suddenly make gasping noises. “We don’t think they are signs of distress,” Downar said. “They’re just basic human reflexes, sort of primordial reflexes.” Vomiting can also happen when the diaphragm contracts, “which is not nice to see, so we give rocuronium to suppress that.”Monitors aren’t used. There are no monitors measuring brain waves or heart activity. Doctors say it would take away from the intimacy of the experience for the person and the family.
“In MAID, I just put my hand on their pulse,” said Dr. Bill Wong, program chief and medical director in the department of anesthesiology at Trillium Health Partners, and a member of the board of MAiDHouse, a non-profit that provides a home-like environment for those granted an assisted death.Wong said he senses respirations by watching or feeling the person’s chest, or measuring their pulse with his fingers on their neck or wrist. “With MAID, it’s often done at home. We want to make it a very non-clinical event for the patient and the family. So, we don’t bring in all these machines and do all this monitoring.”
“Sometimes I’ll shake the person’s shoulder. ‘Hello, John, are you awake there?’ And there’s no response, and from my practice, and knowing the medications and the doses we use, we know that the patients are not going to be aware and awake,” said Wong, who has performed, by his rough estimate, 200 to 250 MAID procedures. He knows Zivot personally. He trained with him back in Winnipeg, and later at Toronto’s Sunnybrook Hospital. “So, I do know Joel. But I can assure you clinically, and amongst all the providers, we find that the regimen we’re using is very good.”
“What we look for in terms of distress would be visible signs of grimacing or moving or something, and there is none of that,” said Perrot, chair of MAiDHouse’s board of directors.
What we look for in terms of distress would be visible signs of grimacing or moving or something, and there is none of that
“The only discomfort I have ever seen is sometimes from the (injection of) propofol, which is a very different thing than Zivot is talking about in his articles and allegations. I’ve heard him speak and I’ve read some of the things he’s written, and it makes absolutely no sense to me.”
Zivot did his residency in anesthesiology at the University of Toronto, and a fellowship in critical care medicine at the Cleveland Clinic in Cleveland, Ohio. He was once featured in an American Society of Anesthesiologist’s YouTube series, When Seconds Count, for the time he poured buckets of ice over a brain injured woman who was having a seizure, to prevent further brain damage. The hospital’s cooling blanket was broken. More recently, Zivot was the lone witness called by the defence in the murder trial of an Ohio doctor charged with killing 14 dying patients by authorizing large doses of fentanyl. Zivot testified that underlying health problems caused their deaths. In April, a jury found William Husel not guilty on all counts.
Five years ago, Zivot was handed a pile of autopsies from 43 executed American prisoners, and when he looked at the autopsies there was a common finding of lung injury, specifically, pulmonary edema, the accumulation of fluid in the lungs that can occur classically in heart failure and that, as an ICU doctor, he sees not infrequently. “It’s a very distressing kind of thing to happen,” he said. “You’re basically drowning in your own secretions.”His theory is that the drug pentobarbital used in capital punishment, when administered in the quantities injected, can have a toxic, noxious effect on tissue and “burn the lungs from the inside.” He’s been an expert witness against the use of lethal injections for executions in America. “Every time I did this, I lost every single time,” he said. “The court is not so much interested in private suffering.”
Pentobarbital is not used in MAID in Canada. “But I think propofol could do the same thing because of the way it’s configured,” Zivot said. His hypothesis is entirely unproven. “There’s no study that has looked at this specifically, because there is no therapeutic setting that would permit it,” he acknowledged. “There’s no animal study that, as far as I know has ever been done that looks at this very high dose of propofol, because it would be unethical.“My opinion is based on this: 100 mg of propofol, when it’s injected, it burns. It burns in the veins. People say so. If I gave them 10 times that amount, I would be concerned that burning sensation could be quickly transmitted through the body, and the lungs are particularly at risk for that kind of potential problem.”
“You’re right: I don’t know. My ask here would be to perform autopsies on people who have been given high dose propofol.”
When they say things to me like this is ‘beautiful,’ I know that we’re not any longer having a scientific conversation
None of the drugs used in euthanasia have a package insert that includes an indication or dosage to be used to kill, he said. He also questions why MAID patients are getting a paralyzing drug to keep them from moving if they’re already dead. He worries paralytics could mask an unpleasant death and has argued that their use in MAID should be ceased.
Is he opposed in principle to MAID? “I can’t know,” he said. “I have concerns, grave concerns, about MAID, as many others do. We don’t want to be killing people who are sad and lonely and poor. No one thinks that’s a good idea, and yet that’s happening.
“So, do I have concerns? Yeah, I have concerns. I also have concerns about how medicine is the handmaiden here. I have concerns with the fact that MAID (proponents) are being murky about how they think people are dying.”
He is not arguing that Canada’s MAID law should be repealed. “But when I talk to people who are doing MAID, they get very defensive, and when they say things to me like this is ‘beautiful,’ I know that we’re not any longer having a scientific conversation.”
Zivot wrote that MAID in Canada “may very likely provide a torturous death.” But even a sedating dose of propofol can render one “insensate,” unable to feel anything, one anesthesiologist wrote in the comments section. Even if pink, frothy fluid accumulated in the lungs, “you cannot make any judgement of comfort based on pathology samples,” Downar said. “That’s not how you assess comfort.”
Those seeking assisted death must be suffering “intolerable” or “unbearable” physical or psychological pain. “Please, please, please give me two minutes of ‘death by drowning’ (that I would most likely be cognitively unaware is happening) over days, weeks, months of agonizing pain from a metastatic cancer that I am not going to survive,” another reader commented.