There was nothing unusual, in the early 1970s, about a student hearing one of his professors preach during chapel.
But one sermon — “How Would You Like to Die?” — impressed the seminarian who would later become United Methodist Bishop Timothy Whitaker of Florida. Theologian Claude H. Thompson had terminal cancer and, a few months later, his funeral was held in the same sanctuary at the Candler School of Theology in Atlanta.
“What hit me was that he calmly preached on that subject — even while facing his own death,” Whitaker said. “It hit me that that, if death is one of the great mysteries of life, then that needs to be something that the church openly discusses. …
“Yes, we live in a culture that is reluctant to talk about death. But I decided that it’s important for us to hear from our elders who is facing this issue, head on.”
Thus, soon after doctors informed him that his own cancer is terminal, Whitaker wrote a lengthy online meditation, “Learning to Die.” The 74-year-old bishop is retired and receiving hospice care, while living in Keller, a small town near the Virginia coast.
“Being a pastor, I considered it a privilege and also an education to linger beside many deathbeds. I have tried to never forget that, unless I die abruptly in an accident or with a heart attack or stroke, sooner or later the subject of death will feel very personal to me,” he wrote. Now, “in the time that remains for me I have one more thing to learn in life, which is to die. … I had always hoped that I would be aware of the imminence of my death so that I could face it consciously, and I am grateful that I have the knowledge that I am going to die soon.”
Certainly, Whitaker noted, the Orthodox theologian Father Thomas Hopko was correct when he quipped, while facing a terminal disease: “This dying is interesting.”
Dying is also complicated — raising myriad theological questions about eternity, salvation and the mysteries of the life to come, he noted. The Bible, from cover to cover, is packed with relevant stories, passages and images. The same is true of the writings of early church leaders who preached eternal hope, even when suffering persecution and martyrdom. Over and over, the saints proclaimed their belief in the resurrection of Jesus.
Whitaker noted that Methodists can ponder this quote from their pioneer John Wesley: “But what is the essential part of heaven? Undoubtedly it is to see God, to know God, to love God. We shall then know both His nature, and His works of creation and providence, and of redemption. Even in paradise, in the intermediate state between death and resurrection, we shall learn more concerning these in an hour, than we could in an age, during our stay in the body.”
But what about the big questions that modern believers might struggle to ask? What about their fears of living with a terminal disease and the complicated questions surrounding death itself?
Early Methodists believed that preparing for death was simply part of life, and outsiders noted that “Methodists die well,” Whitaker said. The problem in churches today is that dying is often viewed as “a counseling issue,” or merely a “therapeutic challenge” for busy clergy.
For centuries, Christians developed rites linked to what they called the “good death,” or even the “happy death,” he noted. While millions now shudder at the thought of dying alone in a hospital, clergy should teach — especially in the age of hospice — how believers can plan to die surrounded by family and their fellow believers.
Yet many clergy are reluctant to discuss these subjects from the pulpit or in educational events addressing modern realities, as well as centuries of rituals and prayers.
“I can understand this reluctance — because they’re going to have many parishioners who will be alarmed or upset by any open discussions of these topics that our culture wants to ignore,” Whitaker said.
“But the church is supposed to help us prepare for death. And this isn’t just about someone receiving a terrible diagnosis. Death is something that can strike at any moment. … The church can’t be silent, in the face of death.”
— Dying patient denied assisted dying in Catholic-run hospital
Jane Morris says her friend, who had motor neurone disease, ‘had a terrible experience and she had to seek help outside of the hospital system’ in order to die via voluntary assisted dying.
Sally wanted to die on her own terms. But despite voluntary assisted dying being legal in Victoria, her advocates say a Catholic palliative care facility obstructed access
When 60-year-old Sally* told her neurologist that she wanted to choose when to die, she was dismissed. Diagnosed with motor neurone disease, Sally knew her condition was incurable and that her rapid decline could include respiratory failure, difficulty swallowing and cognitive decline.
She wanted to die on her own terms, before her symptoms became unbearable. But Sally was receiving treatment at a Catholic palliative care hospital.
Sally lived in Victoria, where legislation allows those with neurodegenerative conditions such as motor neurone disease access to voluntary assisted dying. But her advocates say none of the doctors who diagnosed and treated her would provide the necessary paperwork for her to access euthanasia, nor would they refer her to someone who would.
Sally’s calls and emails to the hospital, an institution that objected to euthanasia, elicited promises of a response at a later date that never came.
“She had a terrible experience and she had to seek help outside of the hospital system,” says Jane Morris, the vice-president of Dying with Dignity Victoria. “She was one of the most lovely people I’ve ever met and it was cruel she was ignored or met with empty platitudes.”
By the time Morris met Sally, she couldn’t write and was communicating with a sight board. “She kept asking me to write down her story and tell it one day for her,” Morris says. “She told me that she wants voluntary assisted dying to be discussed openly, to be destigmatised and not subject to the religious doctrine of faith-based health facilities.”
Doctors and legal experts who spoke to Guardian Australia have called for voluntary assisted dying laws, which differ between the states and territories, to be nationalised and made more humane so that institutional objection does not lead to delays in care, or to patients dying in places they do not feel comfortable.
Depending on where someone lives, the catchment area they fall into may mean that the only local palliative care service is run by a Catholic organisation, which all have different policies about how they treat euthanasia. Under Catholic Health Australia’s code of ethics, any action or omission that “causes death with the purpose of eliminating all suffering” is not permissible.
Sally’s condition declines
The months of delays by the hospital would prove devastating for Sally. Her pain increased as her condition progressed, making it difficult to eat, speak and swallow. It meant taking the euthanasia medication orally was no longer an option, even if she was approved.
Desperate, Sally went outside the hospital system to a GP and asked for help. She was referred to the Victorian Voluntary Assisted Dying Statewide Care Navigator service, who helped her find a specialist and get the paperwork she needed, and she was put in contact with a voluntary assisted dying doctor trained to deliver euthanasia intravenously.
The doctor was not comfortable administering the medication outside a hospital and by the time she was approved, Sally was no longer well enough to travel to a health facility.
Plus, she wanted to die in her home.
When specialist doctor and voluntary assisted dying provider Eleanor* heard about Sally’s plight, she offered to help without hesitation. Eleanor assisted in getting approvals, travelled to Sally’s home and administered euthanasia drugs to her intravenously.
“I was sad and angry that she was delayed from accessing a service she had a right to,” Eleanor tells Guardian Australia.
“No one would write the letter that gave her access to voluntary assisted dying. She deteriorated very quickly and she lost the window in which she was well enough to comfortably go through the process in terms of going to doctor’s visits to get the approvals. So she needed to find doctors willing to come to her home. Unfortunately, cases like this are not rare.”
Sally’s situation was further complicated by federal legislation that prevents anyone seeking information or advice about voluntary assisted dying from a health professional over an electronic carriage service, ruling out telehealth consults for assistance. It is one of the reasons experts say uniform national legislation is needed.
Eleanor believes public funding for hospitals and aged care homes should come with a responsibility to provide a full suite of health services, including voluntary assisted dying.
“The alternative is sometimes to watch someone slowly suffocate to death, or die of a bowel obstruction, or starve to death because they can’t access a more humane way of dying,” she says. “We need national legislation to make the process more humane by taking the best of the legislation in each state and adopting it everywhere.”
It can also be difficult to find a doctor to administer or approve euthanasia drugs, with a shortage of trained voluntary assisted dying doctors, which Eleanor says is partly due to stigma and confusing legislation.
“Most doctors agree with voluntary assisted dying, but feel it is too hard to become a practitioner themselves.”
‘A huge power imbalance’
Victoria was the first state to pass voluntary assisted dying laws in 2017 and since then the other states have followed. In December 2022, commonwealth laws that stopped Australian territories from making new laws on voluntary assisted dying were repealed.
Three states – Queensland, South Australia and New South Wales – include institutional objection provisions in their legislation. Ben White, a professor of end-of-life law at Queensland University of Technology, says it means in those states, people are able to access voluntary assisted dying if they are a resident of an aged care or palliative care facility, even if the facility objects, because it is considered the patient’s home.
While conscientious objection by individual health professionals is protected by the Victorian legislation, objections by institutions are governed by their own policies, which White says aren’t always transparent. The Victorian health department has guidelines for how institutions can manage objections, but this is not binding. Health professionals are also barred in Victoria from raising voluntary assisted dying with their patients – the patient must bring it up first.
“I think we should be able to explain to people all the options they have,” says a health professional who has worked in end-of-life care for decades and did not want to be named. “I just believe in people being able to make informed choices – we’re talking about competent … people who already have a terminal illness.”
White agrees: “I think the key issue here is there’s a huge power imbalance.
“You’ve got people who by definition are terminally ill, expected to die shortly, trying to navigate and access voluntary assisted dying in a situation where the institution holds all the cards.”
In a study published in March, White and his colleagues interviewed 32 family caregivers and one patient about their experience of seeking voluntary assisted dying, including experiences with institutional objection. The objections described generally occurred in Catholic facilities or palliative care settings, which meant some or all of the euthanasia process could not happen on site.
Most commonly, patients were not allowed to meet with a doctor to be assessed; were prevented from accepting delivery of the euthanasia medication from a pharmacy; or were barred from taking the medication or having it administered to them.
White says it can leave families scrambling to transfer their loved ones elsewhere to die, including patients with conditions that made transportation painful.
One of the study participants said: “It will always be a great sadness for me that the last few precious hours on Mum’s last day were mostly filled with stress and distress, having to scurry around moving her out of her so-called ‘home’.”
There is a strong argument to limit the power of institutions to object to voluntary assisted dying when it harms patients, White says.
What Catholic hospitals could do
Oncologist Dr Cam McLaren says a component of cancer medicine is “fighting a losing battle and sometimes all you can do is choose the terms in which you die”.
It is why he became a voluntary assisted dying provider soon after Victorian legislation was introduced. “I was, and still am, in high demand and I have been involved in the assessment of about 300 voluntary assisted dying cases,” he says.
McLaren works for a Catholic hospital and says the values of religious organisations have “allowed them to do some incredible work in palliative care out of a desire to help people”.
He has helped facilitate the transport of patients off site to administer their euthanasia medication. He says different institutions have different levels of comfort with assisted dying and support certain “tiers” of access only; some allow doctors to consult with patients about the topic, but aren’t comfortable with the death occurring on site, for example.
“I completely support the ability of religious hospitals to refuse to be involved in practitioner administration of the drugs on site – that’s completely against their codes and morals,” he says.
“But a lot of the other steps in the process don’t involve any action. It’s just a conversation with a patient or information. And a discussion should not have the capacity to violate religious boundaries.
“I think a good model is for the hospital to allow the assessment and the delivery of the medication to the patient and then give patients time to plan to go home to have the medication administered there.”
But McLaren says this isn’t enough to protect patients in an aged care facility, where the facility is already home.
“And we have seen barriers in aged care homes overtly or covertly with non-assistance and noncompliance, so we have patients asking for months or weeks to access voluntary assisted dying and by the time they’re referred to me, it’s too late because the process takes time, which they don’t have.”
In NSW, voluntary assisted dying legislation will come into effect on 28 November, but there are still unanswered questions about barriers to access for patients being treated in religious public organisations.
People wishing to end their life in the state must be assessed by two doctors as likely having less than six months to live. A document seen by Guardian Australia detailing the response of Catholic health services Calvary Health Care, St John of God and St Vincent’s Health Australia to voluntary assisted dying suggests that these organisations will not allow assessments to be undertaken on site, with patients having to be transported elsewhere for the assessment or referred on to another hospital for care.
If a person has been approved for euthanasia to be administered by a medical practitioner, the document also outlines that the patient will need to go to another health provider or be discharged home. Doctors are concerned that these transfers may unnecessarily increase pain and suffering for patients at the end of their lives.
The document says “we do not abandon our patients” – if a person is considering or actively pursuing euthanasia, “our hospitals do not change our commitments to their provision of care”.
A spokesperson for Catholic Health Australia said on behalf of all three hospitals: “Our hospitals don’t provide [voluntary assisted dying (VAD)].”
“However, we recognise that some patients may wish to explore the option of VAD while under our members’ care. In that event, our services will never block or impede a person’s access to VAD if that’s their choice. Our services will always respect patient choice.
“When it comes to end-of-life, our members choose to specialise in palliative care. Other hospital providers choose to maintain an expertise in VAD. Transferring patients to a specialist provider when a service is not available is standard practice in the public health system.”
Dr Eliana Close, a senior research fellow at the Australian Centre for Health Law Research, has analysed institutional objection to euthanasia and says it is difficult to get data on how prevalent it is.
“We need to now see research and monitoring around how legislation in different states is unfolding and working in practice and whether rights are being respected,” Close says.
“We have certainly found we need stronger national laws to address that power imbalance between institutions and individual rights.”
Close says she finds it “completely abhorrent that publicly funded institutions should be allowed to deny access to legally available healthcare”.
“Not only is that causing harm to the patients in terms of pain and suffering, it’s causing harm to their families who have to witness it – and that has lasting impacts on their bereavement.”
Celebrating a new year — as Jews the world over will do this week, when Rosh Hashana begins on Friday at sunset — is all about making changes. It’s a time for new beginnings, for wiping the slate clean and starting over from scratch. In that spirit, on Rosh Hashana Jews say prayers and listen to readings that celebrate the creation of the world and of human life.
But Rosh Hashana also strikes a different, seemingly discordant note. Unlike so many other New Year’s traditions, the Jewish holiday asks those who observe it to contemplate death. The liturgy includes the recitation of a poem, the Unetaneh Tokef, part of which is meant to remind Jews that their lives might not last as long as they’d hope or expect. “Who will live and who will die?” the poem asks. “Who will live out their allotted time and who will depart before their time?”
And we’re not talking about a gentle death at the end of a reasonably long life; we’re talking about misfortunes and tragedies that can cut any of our lives short. “Who shall perish by water and who by fire,” the poem continues, “Who by sword and who by wild beast / Who by famine and who by thirst / Who by earthquake and who by plague?”
This focus on death might seem misplaced, bringing gloom to the party. But as a research scientist who studies the psychological effects of spiritual practices, I believe there is a good reason for it: Contemplating death helps people make decisions about their future that bring them more happiness. This is an insight about human nature that the rites of Rosh Hashana capture especially well, but it’s one that people of any faith (or no faith at all) can benefit from.
When planning for the future, people typically focus on things that they think will make them happy. But there’s a problem: Most people don’t usually know what will truly make them happy — at least not until they are older. Across the globe, research shows, people’s happiness tends to follow a U-shaped pattern through life: Happiness starts decreasing in one’s 20s, hits its nadir around age 50 and then slowly rises through one’s 70s and 80s, until and unless significant health issues set in.
Why the turnaround at 50? That’s when people typically start to feel their mortality. Bones and joints begin to creak. Skin starts to sag. And visits to the doctor become more frequent and pressing. Death, hopefully, is still a good ways off, but it’s visible on the horizon.
You might think this morbid prospect would further decrease contentment, but it ends up having the opposite effect. Why? Because it forces us to focus on the things in life that actually bring us more happiness. Research by the Stanford psychologist Laura Carstensen has shown that as we age, we move from caring most about our careers, status and material possessions to caring most about connecting with those we love, finding meaning in life and performing service to others.
That’s a wise move. When people in the Western world want to be happier, research shows, they tend to focus on individual pursuits. But that same research confirms that this strategy doesn’t work well: Pursuing happiness through social connection and service to others is a more reliable route.
Of course, you don’t have to be old to confront death. During the SARS outbreak and the Covid pandemic, younger adults changed what they valued, research showed. When death suddenly seemed possible for anyone, even those in the prime of their lives, younger people’s opinions about how best to live suddenly began to look like those of seniors: They turned toward family and friends, finding purpose in social connection and helping others.
You don’t even need to face something as drastic as a pandemic to experience some version of these changes. Research shows that simply asking people to imagine that they have less time left, as congregants do on Rosh Hashana, is sufficient.
Rosh Hashana hardly has a monopoly on this insight. Christian thinkers such as Thomas à Kempis and St. Ignatius of Loyola urged people to contemplate death before making important choices. Stoics like Marcus Aurelius argued that meditating on mortality helped people find more joy in daily life.
But the particular brilliance of Rosh Hashana is that it combines thoughts of death with a new year’s focus on a fresh start. As work by the behavioral scientist Katy Milkman and her colleagues has shown, temporal landmarks like New Year’s Day offer an effective opportunity for a psychological reset. They allow us to separate ourselves from past failures and imperfections — a break that not only prods us to consider new directions in life but also helps us make any changes more effectively.
There is a lesson and an opportunity here for everyone. Contemplate death next Jan. 1 (or whenever you celebrate the start of a new year). Any brief moments of unease will be well worth the payoff.
Many Americans report that their relationships with loved ones continue past death in some way, according to a recent Pew Research Center survey.
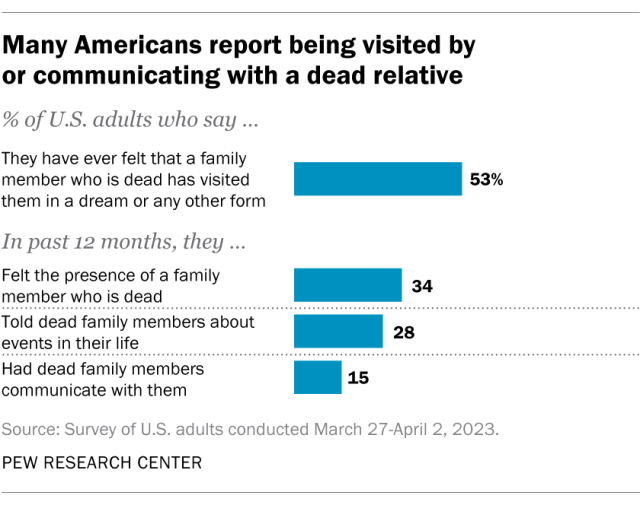
Around half of U.S. adults (53%) say they’ve ever been visited by a dead family member in a dream or some other form. And substantial shares say they’ve had interactions with dead relatives in the past 12 months:
34% have “felt the presence” of a dead relative
28% have told a dead relative about their life
15% have had a dead family member communicate with them
In total, 44% of Americans report having at least one of these three experiences in the past year.
Women are more likely than men to say they have had these kinds of interactions with dead family members. And people who are moderately religious are more likely than others – including those who are highly religious and those who are not religious – to have experienced these things.
The survey was conducted March 27-April 2, 2023, among 5,079 adults on the Center’s American Trends Panel. It included Americans of all religious backgrounds, including Jews, Muslims, Buddhists and Hindus. But there are not enough respondents from these smaller groups to report on their answers separately.
While the survey asked whether people have had interactions with dead relatives, it did not ask for explanations. We don’t know whether people view these experiences as mysterious or supernatural, or whether they see them as having natural or scientific causes, or some of both.
For example, the survey did not ask what respondents meant when they said they had been visited in a dream by a dead relative. Some might have meant that relatives were trying to send them messages or information from beyond the grave. Others might have had something more commonplace in mind, such as having dreamt about a favorite memory of a family member.
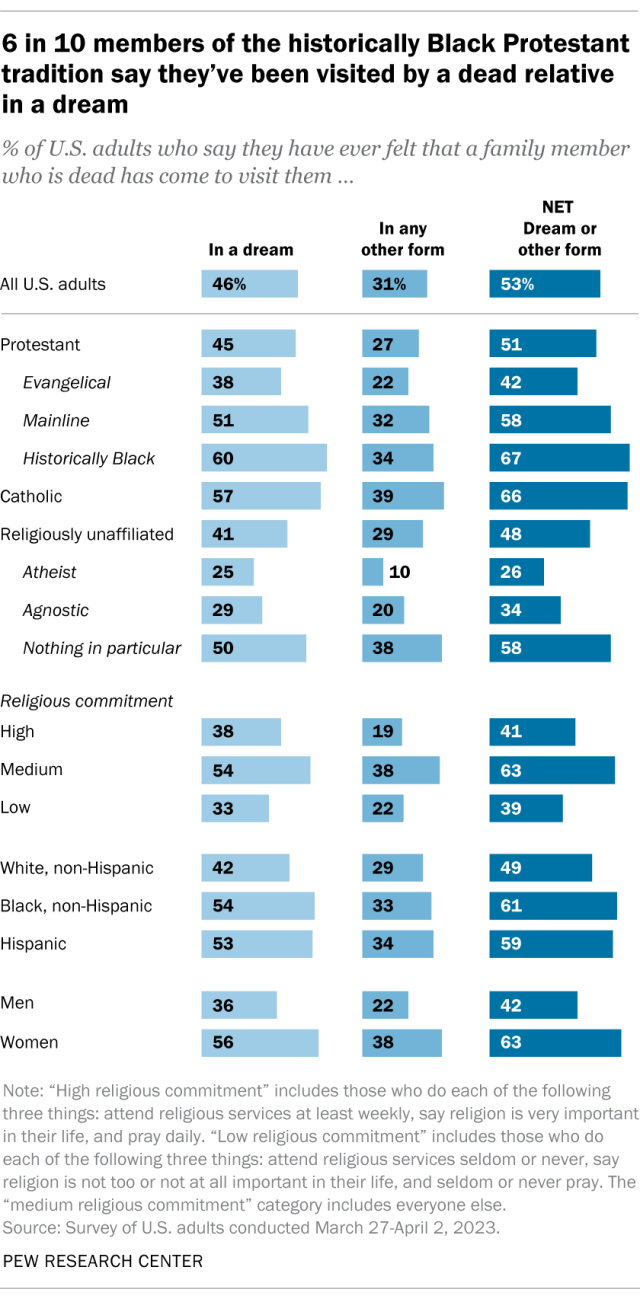
Experiences with being visited by a dead relative
Overall, 46% of Americans report that they’ve been visited by a dead family member in a dream, while 31% report having been visited by dead relatives in some other form.
Roughly two-thirds of Catholics (66%) and members of the historically Black Protestant tradition (67%) have ever experienced a visit from a deceased family member in some form. Evangelical Protestants are far less likely to say the same (42%).
Roughly half (48%) of Americans who are religiously unaffiliated – atheists, agnostics, and those who report their religion is “nothing in particular” – say they have ever been visited by a dead relative in a dream or other form. However, those who describe their religion as nothing in particular are much more likely to say they have ever been visited by a deceased loved one (58%) than are agnostics (34%) and atheists (26%).
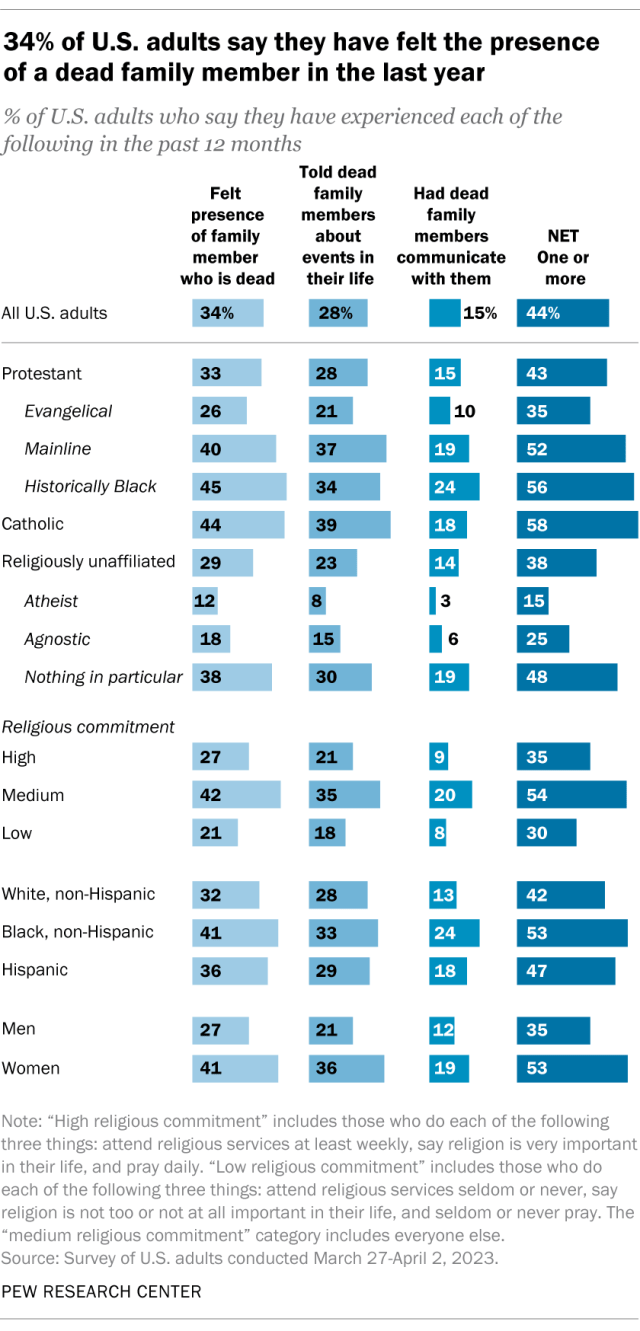
Recent contact with deceased relatives
When asked about recent experiences – things that have happened in the last 12 months – 34% of Americans say they have felt the presence of a dead family member and 28% say they have told dead family members about events in their life. Fewer respondents (15%) say a deceased family member has communicated with them in the past year.
Women are more likely than men to say they had at least one of these three experiences in the last year (53% vs. 35%). For example, women are more likely than men to say they recently have felt the presence of a dead family member (41% vs. 27%).
When it comes to religion, about half or more of Catholics (58%), members of the historically Black Protestant tradition (56%) and mainline Protestants (52%) say they have had at least one of these three experiences in the last year – significantly more than the 35% of evangelical Protestants who say the same.
Relatively few atheist (15%) or agnostic (25%) adults report any of these experiences over the last 12 months. In contrast, roughly half (48%) of those who say their religion is nothing in particular reported one of these experiences.
These experiences also differ by Americans’ religious commitment, as measured by a scale that includes indicators of religious service attendance, prayer frequency and self-assessments of religion’s importance in one’s life.
Americans with medium levels of religious commitment are more likely than those with either higher or lower levels of religious commitment to say they’ve felt the presence of a family member who is dead, told a dead family member about events in their life, and felt a dead relative communicate with them in the past year.
Summing up this pattern in another way: People who are moderately religious seem to be more likely than other Americans to have these experiences. This is partly because some of the most traditionally religious groups – such as evangelical Protestants – as well as some of the least religious parts of the population – such as atheists and agnostics – are less likely to report having interactions with deceased family members.
— Volunteers ensure dying patients don’t face death alone
In 2005, Trinity Health started No One Dies Alone, a program where volunteers visit patients who are nearing death, standing by their bedside as they approach death. Volunteers accompany patients by holding their hands, read to them, play music or talk about life, and death, with the patients. The program was on hiatus during the COVID pandemic, but rebooted this past September.
Trinity Health’s palliative care program ‘No One Dies Alone’ sends volunteers to be with patients in final hours, give families respite
Dying is a personal — and often difficult — thing to discuss.
From choosing hospice care and drafting wills to an entire continuum of end-of-life care, there are many views about what’s best.
But there’s one thing most people can agree on: no one wants to die alone.
And thanks to a group of volunteers through Trinity Health, no one has to.
In 2005, a team of people at the Catholic health care system started No One Dies Alone, a palliative care program that assigns volunteers to be present with patients who are nearing death, standing by their bedside when family and friends can’t be present.
“No One Dies Alone is a comfort companion program for those patients who don’t have family or whose family can’t be present at the bedside 24/7,” said Barbara Stephen, bereavement specialist in the volunteer department at Trinity Health Oakland and Trinity Health Livonia. “Whether family and friends are out of state, or can’t get in right away, or are in need of respite care, we provide volunteers who can be there if needed. We’re a friend who looks for any kind of distress and keeps them company.”
Lisa Marie Blanek, a No One Dies Alone volunteer, reads a book bedside of a patient. The No One Dies Alone program has volunteer read to terminally-ill patients, play music or just hold hands with people as they near death. The program ensures no patient at Trinity Health’s Livonia and Pontiac hospitals dies without anyone else in the room.
The program started after Trinity Health’s Palliative Care Program did a study on end-of-life care around the country, noting 50% of patients die in a hospital, and of those, about 10-12% die alone, without family and friends at their side.
Through No One Dies Alone, volunteers keep patients company in their final days, doing everything from reading to patients, holding their hand, or calling a nurse if a patient is in discomfort.
“We are there to be at the bedside,” Stephen told Detroit Catholic. “We do a lot of hand-holding. We don’t do nursing care, but what we do is a lot of talking, prayers if they want, and just being that second set of eyes. If we see some distressing signs, like pain or a need for medical care, we call the nurse. We get a wet washcloth if they are running a fever, or Chapstick when their lips are chapped. We’re there to be that friend by the bedside, keeping an eye on them, letting them know they are not alone.”
No One Dies Alone took a hiatus during the COVID-19 pandemic, when volunteers weren’t permitted in hospitals.
The program rebooted last September, operating out of Trinity Health’s Oakland (Pontiac) and Livonia locations, with 38 volunteers at Oakland and 29 in Livonia.
No One Dies Alone volunteers typically operate on three-hour shifts and receive a brief report about the patient, including a person’s family situation, interests and condition. Volunteers often build a rapport with the patient’s family, stepping in to allow family members to get a bite to eat or a change of clothes at home.
Susan Abentrod practices tucking a patient in at the Trinity Health Oakland Hospital in Pontiac. No One Dies Alone volunteers are there to fill in the gaps for family and friends who can’t be with patients nearing death 24/7 and for doctors and nurses who are managing multiple patients at a time.
“The volunteer who is coming in to (watch over) the person who is dying often is not able to talk to the patient, but they do talk with family, who are grateful they are there,” said Kelly Herron, visit coordinator for No One Dies Alone. “They appreciate that someone is stepping into the space for their family, knowing their loved one is being watched over.”
Volunteers are not meant to act as medical personnel or hospice workers. Their work is more a ministry of presence, Herron said.
“As a volunteer, our role is limited because we are there to hold a space,” Herron said. “It’s about showing up and being a companion, being willing to talk about the things they want to talk about. It’s about being a friend and putting them first, not being afraid to listen to them talk about what they are feeling as they near the end.”
Sometimes, volunteers can even fulfill special requests, such as having terminal patients see their pets one last time.
“A lot of patients have pets at home, and when we ask them if they have a wish, often they regret they’ll never see their dog or cat again, so we bring the pets in — as long as they are updated on their shots — so they can be with their owner,” Stephen said.
Sometimes, volunteers are a shoulder for family members struggling with the loss of their loved ones, Stephen added.
“We had a young mom who was dying, and she had a 7-year-old daughter, and the dad didn’t know how to tell the daughter,” Stephen said. “(The mother and daughter) shared a birthday, and we knew the mom wasn’t going to make it to the next birthday. We asked what they usually do for their birthday, and the dad said they always have a tea party. So we got the mom out of her hospital gown, had some nice pajamas for her, and got the daughter dressed up. My husband went to Costco to get balloons, and we had a tea party. We took pictures, not only for the daughter to remember, but for the mom to hang onto that memory. It’s not easy losing your mother at 7, but it was a lovely time.”
Barbara Stephen, bereavement specialist in the volunteer department at Trinity Health Oakland and Trinity Health Livonia, leads the No One Dies Alone program. She leads a team of volunteers who read to patients nearing death, get them an extra blanket if they need on, play their favorite music on the stereo and are just their for patients who are nearing death. The program is one of presence and accompaniment, Stephen said, just being there for those nearing the end of life.
Most visits are more low-key, but the idea is the same: being with people in their hour of need.
Herron recalls her own experience of being with her own mother when she died, adding it was a comfort to both of them to know she wasn’t alone. It was Herron’s time as a No One Dies Alone volunteer that prepared her for her mother’s death, she said.
“When my mom died, I was sitting there with her,” Herron said. “Everyone thought she probably would die soon. It was the middle of the night, everyone went to sleep, and I remember holding my mom’s hand, saying, ‘I’m going to go to sleep. You go to sleep too, and I’ll talk to you in the morning. But I’m right here.’ I was just pulling my hand back to demonstrate that I was falling asleep, but I didn’t close my eyes. I just looked at her, and she opened her eyes and look at me before she died.
“To me, that’s why we do this,” Herron added. “If at any point, someone is going to open their eyes or squeeze their hand, it’s so comforting that someone is there — that they are not forgotten, that they are not alone, and that it matters to someone as you are making that transition.”
Barbara Stephen, bereavement specialist in the volunteer department at Trinity Health Oakland and Trinity Health Livonia, poses for a photo with No One Dies Alone volunteers, Chuck Pokriefka, Lisa Marie Blanek, Susan Abentrod and Joe Fugitt.
While No One Dies Alone is a comfort to the dying and their families, it’s also an added benefit to hospital medical care staff, who appreciate having an extra set of eyes and ears in the room.
“Our nurses are so compassionate, and they just want to be there. They don’t want anybody to be alone when it is the end of someone’s life, but they have a patient load,” Stephen said. “So when they see us, they are so excited. When our volunteers come in, the nurses ask if they can get us a cup of coffee, or if we need anything. They take really good care of us, because they appreciate there is always someone there with their patients.”
A man from the home care agency calls on a Monday morning. “The caregivers are complaining. It’s too hard to transport Sara, to move her from the bed to the wheelchair and onto the stairlift. You need a lift or some other assistive device.”
A rush of sadness settles into my body. The end has arrived. “Sara is leaving on Friday,” I say, “Can we hold out till then?”
“Oh,” he says, and pauses, “I’m so sorry to hear this.”
My partner, Sara Flint Greenberg, was nearing the end of her nine-month journey through amyotrophic lateral sclerosis, more commonly known as ALS or Lou Gehrig’s disease, and she would take her life on Friday.
There is nothing more we could do. Her body has been ravaged by this devastating disease and she has been crystal clear, from the beginning, that she would leave when she can no longer take care of herself.
There are steps to the end of this journey.
Later that Monday morning, Sara speaks with a doctor, answering some required questions. Does she have less than six months to live? Is she mentally capable of making the decision to end her life? Can she self-administer the medication? Luckily, the session is short. Sara spends much of her day on a machine which helps her to breathe. Too much talking leaves her gasping.
On Wednesday morning Sara speaks with a second doctor who agrees that she qualifies to receive medications that assist in dying under the requirements of the California End of Life Option Act. The medication that will allow Sara to leave will be ready on Friday.
On Wednesday afternoon we celebrate our wedding. Sara and I marry in the late November light of our living room. I am not strongly attached to marriage, but as the day of Sara’s passing drew closer, I felt an overwhelming need to express the beauty of our love in ceremony.
The temporary chuppah is held over our heads by Sara’s sons Aaron and Jacob, our friend Audrey and a caregiver. We have found an independent rabbi to marry us because I am not Jewish. The rabbi is adorable in her Converse sneakers, covered with stars, as she takes us through this bittersweet ceremony. The ceremony is short because Sara is exhausted. It is her last gift to us, her family.
On Friday morning, our friend Margaret arrives from New York, kisses Sara on the cheek and tells her she loves her. It is all anyone can do. Audrey is in the kitchen. She has been with us for days, helping us through.
Later in the morning, a rabbi from our synagogue arrives to help us say goodbye to Sara. Margaret and Audrey go downstairs to wait. They sit, mostly silent and sometimes hold hands. The room feels heavy. They can hear Sara breathing above them, but they know she will not be there for long. It is one of the most reverent acts of love: to witness in silence the death of another.
At noon, Sara takes a pill to prevent nausea and vomiting when she takes the medication that will end her life. I sit beside her on the couch, Aaron is at her feet and Jacob is across from her. The rabbi is just beyond our circle as he begins to guide us through our final words. Everything is said on the edge of tears. We listen closely to hear our soft voices.
Sara regrets, deeply, that she will never see her grandchildren. She will not see her sons grow further into their lives or settle down with partners and start families. She gathers her breath and questions them closely because this is her last chance. She wants to know what their futures looks like because she will not be there.
There are apologies because anything left to be said has to be said. Death demands it. We make promises because who would say no? Sara would do anything for her sons and I promise to do the same. We celebrate Sara’s bravery. She left a longtime marriage, late in life, and jumped into love with me. And the bravery she shows today in making this choice.
The rabbi asks Sara where we can find her after she’s gone. “Walking in these hills,” she says, of the land surrounding our home where she once walked every day. She is now struggling to breathe and is silent. We are left with silence and the presence of love. We will carry this love everywhere we go.
It is almost an hour after Sara took the anti-nausea pill. She must take the medication now or wait for another day. The hospice nurse has not yet arrived. We call our hospice provider. They tell us to mix the medication with apple juice and give Sara sorbet because the taste can burn her throat. Sara reaches for the medication with both hands. She is ready to leave.
As the medication moves through her body, she prays in Hebrew: “HaShem Sheli, HaShem Sheli, ya’azor li” (“My God, my God, help me”). She recites the Shema, a centerpiece of prayer services in Judaism. As she draws closer to leaving, her last words are “Thank you, thank you,” a beautiful sentiment and a sign, I hope, that she is at peace.
Sara slides slowly down the couch, her cheek resting against the back of my hand. I feel life in her body, but after half an hour I am not sure. The hospice nurse has arrived. I ask him if she has passed. No, she is still here. Another half hour and I ask again. He checks her pulse. She has left.
Walking by a tree the other day, I noticed one brown leaf among the flourishing green. I wondered, “Why is it that this specific one died?”
By Rabbi Zach Shapiro
Dear all,
Walking by a tree the other day, I noticed one brown leaf among the flourishing green. I wondered, “Why is it that this specific one died?”
The question weighed heavily, as Ron and I are preparing to explain the death of a loved one to our toddler children. We know there will be many questions:
”Why?”
”Why now?”
”What does death mean?”
”Will something happen to you?”
”If so, who will take care of me?”
While the conversation will be difficult, we also know it needs to be straight-forward. When talking about death, it’s really important to keep the following in mind:
Don’t use euphemisms. (No one “passed away” or “went to sleep.” The person died.”)
It’s ok to express your own emotions and not hide them.
Make sure you answer the question the child is actually asking. Be brief and simple about it.
It’s ok to share: “a body stopped working” and: “it doesn’t move or eat or play anymore.” If the child asks if the body is like a toy that needs a new battery, explain that living things can’t get new batteries like toys do.
Your child may or may not ask questions. Some questions may unfold over time.
Also – remember this. Every death is different. Sharing the death of an older adult is very different experience than sharing the death of a young person. And different children will respond in different ways.
Mind you, it’s one thing to offer this advice in my moment in time. It’s another to sit and have the conversation with our children. We will rehearse it. We will prepare our answers. But we will also ensure that we are not so over-prepared that we come off as staged.