Everyone should have the right to high-quality palliative care when they have a terminal illness, regardless of their condition, where they live, or their personal circumstances. It’s commonly assumed that everyone with a terminal illness gets the care they need, however one in four people who need palliative care in Northern Ireland are not currently accessing it.
by Craig Harrison
Raising awareness of the issues
The problem can be particularly acute within the LGBT community, and last year, research commissioned by Marie Curie found that concerns around discrimination, stigma and invisibility can often cause LGBT people to access services late or not at all.
To explore these crucial issues, Marie Curie Northern Ireland held a policy seminar to raise awareness of the barriers faced by our LGBT community in accessing end of life care and what can be done to address them.
Held in Stormont, the home of the Northern Ireland Assembly, the event brought together a wide range of stakeholder groups, departmental officials, MLAs and health and social care representatives.
oan McEwan, Head of Policy and Public Affairs at Marie Curie Northern Ireland spoke about the need for LGBT people to be able to access care, free from discrimination.
Championing compassion and understanding
Guests heard from Joan McEwan, Head of Policy and Public Affairs at Marie Curie Northern Ireland, as well as John O’Doherty, Director of local LGBT organisation the Rainbow Project . John discussed the needs of older LGBT people in health and social care, and said:
“Accessing care as an older person is something many of us do not consider we will need until it is upon us – particularly end of life care. This is a difficult time for everyone, but for many LGBT people, fears of homophobia and invisibility exacerbate an already distressing and difficult time.
“Ensuring services are accessible, safe and considerate of the specific needs of LGBT people means understanding their experiences, particularly the impact of homophobia, transphobia and marginalisation throughout their life.
“Marie Curie’s work in end of life care for LGBT people is imperative to ensuring that everyone living with terminal illness in our society can access care and support that is underpinned by compassion and understanding.”
Dr Richard O’Leary spoke about the experiences of he and his partner, Mervyn, when Mervyn was in hospital toward the end of his life.
“The assumption that we were not a couple”
Guests also heard from Dr Richard O’Leary, a retired university lecturer who was a full-time carer for his late partner Mervyn. Richard said:
“When we came to access end of life care as a same sex couple we were fearful of what we might encounter from service providers.
“My civil partner Mervyn was admitted to hospital many times and the assumption that we were not a couple was made at least once during every hospital stay. In the public ward in hospitals I was wary of showing affection to Mervyn because it was unclear whether the hospitals had a protocol to protect us if anyone objected to us being affectionate.
“In hospitals and hospices much of the emotional care of the dying is offloaded to the chaplaincy service. This can be problematic – with one chaplain telling me that they were ‘struggling with the issue’ of same sex relationships.
“Mervyn and I enjoyed 25 years of a committed, loving relationship until he died on 2 August 2013. After Mervyn’s death, there were people in my family and in my faith community who explicitly withheld from me the expression of condolence.
“Service providers should be aware of the disenfranchised grief and reduced social support that may be experienced by LGBT persons during bereavement. I’d like to thank Marie Curie for their pioneering research and leadership in the area of end of life care for LGBT people.”
Making good practice more widespread
The presentations made clear that there are pockets of good practice in end of life care provision for the LGBT community. Service providers and HSC professionals must now work together to take these examples and make them universal – to ensure LGBT people receive high-quality, person-centred care that acknowledges and supports them during terminal illness.
Dr Richard O’Leary, Melanie Legg, Joan McEwan, Mark H Durkan and John O’Doherty at the event on 7 September 2017.
Biff Flanagan, an esophogeal cancer patient, stands with his wife Patricia at their home in Sa Diego, CA on Wednesday, August 30, 2017. Mr.Flanagan received an experimental immuotherapy cancer treatment for his cancer.
[A] new generation of immune-boosting therapies has been hailed as nothing short of revolutionary, shrinking tumors and extending lives. When late-stage cancer patients run out of other options, some doctors are increasingly nudging them to give immunotherapy a try.
But that advice is now coming with unintended consequences. Doctors who counsel immunotherapy, experts say, are postponing conversations about palliative care and end-of-life wishes with their patients — sometimes, until it’s too late.
“In the oncology community, there’s this concept of ‘no one should die without a dose of immunotherapy,’” said Dr. Eric Roeland, an oncologist and palliative care specialist at University of California, San Diego. “And it’s almost in lieu of having discussions about advance-care planning, so they’re kicking the can down the street.”
Palliative care and oncology teams have long been wary of each another. For many oncologists, palliative care teams are the specialists to call in only when curative treatments have been exhausted. For many palliative care specialists, oncologists are the doctors who prescribe treatments without regard to quality-of-life considerations.
But the new collision between immunotherapy and palliative care experts comes at an inopportune moment for health care providers, who have in recent years promoted palliative care as a way to increase patient satisfaction while reducing costs associated with hospitalizations and emergency room visits.
Dr. Cardinale Smith, an oncologist and palliative care specialist at Mount Sinai Hospital in New York, said she has seen a handful of patients who tried immunotherapy treatments after failing chemotherapy, and who were later admitted to the hospital in poor condition. Almost all of them died there, without having been asked about where, and under what conditions, they might prefer to die.
“These conversations are not occurring because of the hope that this will be the miracle treatment,” Smith said. “Unfortunately, on the part of the oncologist, treatments like immunotherapy have become our new Hail Mary.”
Immunotherapies work for only around 15 to 20 percent of cancer patients who receive them.
They have been approved by the Food and Drug Administration for Hodgkin lymphoma and certain cancers of the lung, skin, blood, kidney, bladder, and head and neck — but not for common cancers like prostates and most cancers of the colon and breast. A new type of immunotherapy, CAR-T, was approved earlier this week for leukemia.
But even for those cancers, oncologists and patients sometimes refuse to acknowledge clear signs that immunotherapies are failing, said Dr. Sandip Patel, a cancer specialist and immunotherapy researcher at the University of California, San Diego.
Patel said he now engages home-based palliative care specialists, who can provide supportive care while a patient’s health is relatively stable. “Then, at least when they transition to hospice, it’s not as much of a free fall out of the traditional health system, and if they’re one of the patients who respond to the therapy, great.”
He lamented the fact that patients who fail immunotherapy treatments spend more time in hospitals than with their families at home. “The flip side is, if I had a cancer with a 15 percent response rate, and if the benefit might be longer-term, I’d try it,” he said. “Who wouldn’t buy a ticket to a lottery of that importance?”
But not all patients have a clear idea of what that lottery ticket might cost them. Carrie Clemons’s father, Billy Clemons, who is 68 and is a former Texas state representative, last year stopped responding to chemotherapy for renal cell cancer that first struck him in 2002. His doctors recommended the immunotherapy Opdivo, which had recently been approved for his cancer.
At the time, he was symptom-free from his cancer, though scans showed it had spread to his lungs and some lymph nodes.
Two infusions of the drug, Clemons said, were followed by “eight months of hell,” during which her father became incontinent and had to use a wheelchair, lost his eyesight and most of his hearing and speech, and endured multiple weeks of intubation and care in the ICU. When his heart stopped beating, he needed to be resuscitated.
While immunotherapies trigger debilitating side effects much less frequently than chemotherapy, they can spur potentially life-threatening conditions, depending on the cancer type and the treatment approach. Fewer than 5 percent of patients overall face serious side effects, for instance, but more than one-third of melanoma patients who receive a combination of immunotherapy drugs can experience such conditions. The upside: Half of those melanoma patients will see their cancer shrink for at least two years.
Clemons’s doctors at Houston’s MD Anderson attributed the reaction to a runaway immune system that essentially attacked his central nervous system. To reverse it, he needed weeks of therapy to replace his plasma with that of donors, to clear away his blood’s overly active antibodies.
He slowly improved, though, to the point where only some slight vision impairment remains, and doctors recently declared his cancer in remission.
Although the family is thrilled at the outcome, Clemons said, they had little idea when they began that such side effects were possible, and doctors never engaged the palliative care team to either discuss side effects or help manage them.
She wouldn’t have known to ask about such care. “I always just equated palliative care with hospice,” she said.
Hospitals overall have made some headway in integrating oncology and palliative care specialists, with more oncologists referring patients to palliative specialists to help them ease side effects of treatments and achieve quality-of-life goals.But Roeland, the doctor at the University of California, and others say the integration is less smooth when it comes to cutting-edge cancer treatments.
Palliative care teams have not been able to keep abreast of the breakneck pace of cancer treatments, so they may not be offering up-to-date counsel to patients who ask about possibly life-changing therapies.
Meanwhile, most of the growth in palliative care medicine has happened among clinicians who work in hospitals, where they generally see only those who have done poorly on immunotherapies, for instance.
“They’re not seeing the super-responders,” Roeland said. “So their first reaction usually is, ‘Why would you do that?’”
Biff Flanagan, an esophogeal cancer patient, on a walk with his wife Patricia at their home in San Diego, CA on Wednesday, August 30, 2017. Mr.Flanagan received an experimental immuotherapy cancer treatment for his cancer.
Roeland understands more than most the seductive qualities of an eleventh-hour immunotherapy gambit. He had given up hope of curing Bernard “Biff” Flanagan, 78, of his esophageal cancer in late 2015, and referred Flanagan to hospice care to help him manage his extreme weight loss, fatigue, and the emotional distress he felt from not being able to swallow.
But Flanagan, who speaks with the gruff, seen-it-all humor one might expect from a career FBI agent in LA, wanted to keep seeking a cure.
Roeland said he knew that many hundreds of clinical trials were testing the therapies on other cancers, so he did some digging. A paper from a recent cancer conference showed that some people with squamous cell esophageal cancer responded to immunotherapy. He could arrange to get the drug through the Bristol Myers Squibb, for free.
He presented the idea to Flanagan and his wife, Patricia, with the caveats that it might not work, and could come with possibly significant side effects.
Flanagan jumped at the chance. Patricia, a former professional photographer, was less enthused.
“I ran into her later in the coffee shop,” Roeland said. “She looked at me like. ‘What the hell are we doing here? He doesn’t have a good quality of life.’ I’m feeling guilty now.”
Roughly six weeks into the treatment, Flanagan’s energy was returning, and he found himself at the fridge. “I grabbed a glass of OJ, knocked it down, swallowed it no problem,” he said. “And it was like a miracle. I had another one.”
Now Flanagan has no symptoms, and he experienced only the briefest side effect: a skin rash that abated with ointment. Patricia recently helped him dispose of the morphine and other medications the hospice team had given them.
“If he’d died in the hospital, I would’ve felt terrible,” she said. “If I were in his place at that point, I’d have tried to arrange to die at home at my own choosing, but Biff just didn’t have as strong feelings about that as I had.
“I had little hope that he was going to recover, but it’s just been amazing. He really is living the life he’s always lived.”
Roeland said that for the experience “is so immensely rewarding that it drives an oncology practice. It can be 1 in 100 that happens like that, and you say, well, is it worth it?”
Nora Harris, 64, a former librarian, signed an advance directive after her diagnosis to prevent her life from being prolonged when her disease got worse. Now, her husband said, she’s being kept alive with assisted eating and drinking against her stated wishes.
Bill Harris walks with his wife, Nora, at the Fern Gardens memory care center in Medford, Oregon. Nora Harris, 64, has late-stage Alzheimer’s disease. A former librarian and world traveler, she had signed an advance directive stipulating no care to prolong her life. Controversy has arisen over her husband’s claim that state law is forcing her to be spoon-fed against her stated wishes.
[B]ill Harris is blunt: For more than a year, he has been trying to help his wife die.
The 75-year-old retired tech worker says it’s his duty to Nora Harris, his spouse of nearly four decades, who was diagnosed with early-onset Alzheimer’s disease in 2009.
“Let me be honest: Yes. It’s what she wanted,” he said. “I want her to pass. I want her to end her suffering.”
Nora Harris, 64, a former librarian, signed an advance directive after her diagnosis to prevent her life from being prolonged when her disease got worse. Now, her husband said, she’s being kept alive with assisted eating and drinking against her stated wishes.
The onetime Virginia Woolf scholar and world traveler can no longer communicate, recognize family members or feed herself. She’s being spoon-fed at Fern Gardens, an assisted-living center in southern Oregon, after a local judge ruled against Bill Harris last summer, concluding that state law mandates that she continue to receive help.
“She did not want to be in a position where somebody had to totally take care of her,” Bill Harris said. “When nature, through the disease, basically said, ‘I can’t feed myself,’ Nora’s position was, that’s it. Let nature take its course.”
In recent weeks, Nora Harris has been gaining weight, climbing from less than 100 pounds to 102 or 103 — just enough to keep her stable. Bill Harris learned that, in addition to three state-required daily meals, staffers have been feeding Nora optional snacks, too.
Now he’s considering going back to court to try to stop the snacks in an effort to let Nora Harris lose enough weight to end her life. Twice before, in 2015 and 2016, she fell to 90 pounds and was enrolled in hospice, with six months or less to live, only to rebound, he said, when staffers coaxed her to eat.
“You’re denying Nora the right to die on her terms,” Bill Harris said. “It’s not a right-to-life issue, it’s a right-to-die issue.”
The southern Oregon case underscores the complexity surrounding the use of advance directives for people with Alzheimer’s disease and other dementias.
Bill and Nora Harris met at the San Francisco War Memorial Opera House in the early 1970s and launched a four-decade marriage that included world travel. Nora Harris was a librarian and a Virginia Woolf scholar who told family and friends she never wanted to be utterly dependent on others for care.
Advance directives are legal documents that spell out a person’s end-of-life wishes if they are unable to make their own decisions.
These directives generally allow named agents the power to withdraw artificial hydration and nutrition in the form of feeding tubes, for instance. But when that same nourishment is offered by hand, several states, including Oregon, draw a line, said Thaddeus Mason Pope, director of the Health Law Institute at Hamline University in St. Paul, Minnesota, and an expert on end-of-life law.
Across the U.S., the more than 5 million people living with dementia are typically encouraged to put their end-of-life wishes into writing early and to pick a trusted person to carry them out, said Beth Kallmyer, vice president of constituent services for the Alzheimer’s Association.
That’s no guarantee, however, that those requests can — or will — be honored. In Nora Harris’ court case, her advance directive and testimony from her husband, her daughter and two close friends all indicated that she wouldn’t want anything to prolong her life.
“That court decision basically condemned Nora to the full extent of the Alzheimer’s disease,” Bill Harris said. “They gave her no exit out of this situation.”
But Eric Foster, the court-appointed lawyer who represented Nora Harris, argued that her directive doesn’t specifically mention food and drink presented by hand. Because she now opens her mouth and swallows when food is offered, she has, in essence, changed her mind, he said in a court document.
Bill Harris said that opening her mouth is a reflex, an automatic response to six decades of habit.
Kallmyer, with the Alzheimer’s Association, said it’s hard to tell whether someone with dementia is acting out of reflex or desire. The association recommends against tube-feeding for patients with dementia, while also advising what they call “careful hand-feeding.”
“If they’re eating and they’re opening their mouth, it’s difficult to say they didn’t want it,” she said.
Foster’s stance was backed by a judge who sympathized with Bill Harris’ plight, but sided with Fred Steele, Oregon’s ombudsman on long-term care. Steele said Nora Harris’ advance directive wasn’t specific enough to advise Fern Gardens staff to withhold food and water.
“Our concern was just focused on the administrative rule,” he said. “If the rule exists to prevent a facility from committing elder abuse, our focus was on what the rule required. The rule requires the resident be cued with food and they have the choice of eating or not eating.”
Lynn Rawlins, the center’s administrator, said her hands are tied.
“We have to feed them until they stop opening their mouths,” she said before a tour of the center last month. “Unless feeding them causes more harm from aspirational pneumonia or a choking factor. We still have to feed them, even if they choke.”
Nora Harris is a small woman with graying brown hair and dark, confused eyes. On a recent 88-degree summer afternoon, she wore a maroon fleece sweater, gray sweatpants and mismatched socks.
She spoke in urgent whispers, syllables spilling out, unlinked from words.
Bill Harris put an arm around her shoulders reassuringly.
“Absolutely,” he said. “Of course.”
But he added later: “It’s difficult visiting her, especially when you know what Nora was like before.”
That’s the thorny issue at the heart of advance directives for people who lose the capacity to make their own decisions, said Pope.
If Nora Harris were aware enough to refuse food, instead of passively accepting it, there would be no question.
“Do we listen to the previous Nora or to the current Nora?” Pope said. “That is, unfortunately, not legally or ethically answered well.”
A bill introduced in the Oregon Legislature last year would have allowed an appointed committee to amend the state’s advance-directive form. Critics, including Oregon Right to Life, an advocacy group, opposed the effort, arguing that it paved the way for mistreatment of vulnerable people, including dementia patients like Nora Harris.
“OR legislators move to allow starving, dehydrating the mentally ill,” one headline read. The bill passed the state Senate, but failed to advance.
Nora Harris’ situation also raises issues surrounding a controversial method of hastening death for seriously ill people known as “voluntarily stopping eating and drinking,” or VSED. It causes death through dehydration, usually in seven to 14 days.
VSED is being used by a small but growing number of determined patients with the help of their families, Pope said.
In Washington state, board members at End of Life Washington, a nonprofit that supports medical aid-in-dying, created an advance directive focused on people with dementia. Soon the group plans to release a new form for people who want to leave instructions for stopping eating and drinking at the end of life.
Medical experts say VSED can be a relatively painless, peaceful death. In the absence of nutrition and hydration, the body produces opiate-like substances that blunt hunger and thirst. With additional painkillers, comfort can be ensured, they add.
An analysis of VSED research concluded that “terminally ill patients dying of dehydration or starvation do not suffer if adequate palliative care is provided.” A 2003 survey of nurses in Oregon who helped more than 100 patients with VSED deaths said they were “good” deaths, with a median score of eight on a nine-point scale.
Unlike aid-in-dying laws or rulings now in place in six states, VSED doesn’t require a government mandate or doctor’s authorization.
But the question of whether people with dementia can authorize a VSED death in advance, to be enacted later, when they’ve lost the capacity to choose, remains legally uncertain, Pope said.
“We don’t have statutes, we don’t have regulations, we don’t have a court case,” Pope said. “We have this thing where you’re allowed to refuse medical care. But this is basic care. Are you allowed to refuse basic care?”
For now, the answer in the case of Nora Harris is no.
That’s frustrating for Bill Harris, who says the emotional — and financial — toll of her illness has been enormous.
“The person you know, the person you married, who you love, is basically going away, fading away before your eyes,” he said.
He had planned to retire from his job at Wells Fargo Bank at age 67 but worked an extra eight years to pay for the costs of Nora’s care, which total more than $80,000 out-of-pocket each year. Because she fell ill at age 56, she didn’t qualify for Medicare or other government help.
Worse, though, is seeing his once “extremely bright” wife wandering the halls of the assisted-living center, “like a zombie,” he said.
“Nora was quite enamored of Virginia Woolf,” Bill Harris said, referencing the British author who drowned herself after years of mental illness.
“If she had known this would happen, she would have put rocks in her pockets and jumped in the river. This is absolutely where she never wanted to be.”
[W]hen children lose a parent during adolescence, their mental health as young adults may depend on how comfortable they were with the treatment and support provided at the end of their parents’ lives, a recent study suggests.
To understand the lasting psychological impact of the death of a parent during adolescence, researchers surveyed young adults who had lost a parent to cancer six to nine years earlier, when they were 13 to 16 years old.
Overall, 105 of the 593 young adults (18%) said they had little or no trust in the care provided during the final week of the parent’s life.
Compared to the participants who were satisfied with the final week of care, those who were unhappy were more than twice as likely to suffer from mental health issues like depression, anxiety and eating disorders, researchers report in the Journal of Clinical Oncology, online August 8.
“We already knew that children who have lost a parent are at risk for long-term psychological challenges including depression, risk of suicide, and risk of self-injury,” said Dr. Jennifer Mack, a researcher at Harvard Medical School and Dana-Farber/Boston Children’s Cancer and Blood Disorders Center.
“However, a link to trust in the medical providers of the parent was not previously understood,” Mack, who wasn’t involved in the study, said by email. “This is important because it offers a potential path forward to greater resilience and healing after a parent’s death for young people who experience this type of profound loss.”
The current study focuses not on how teens felt when their parent was dying, or immediately afterwards, noted lead study author Kim Beernaert of the End-of-Life Research Group at Vrije University Brussels and Ghent University.
Instead, it looks at how they feel after several years have passed, Beernaert said by email.
Young people who had little or no trust in the care parents received at the end of life were at least twice as likely to report still feeling bitter toward health providers for failing to make the correct initial diagnosis, stopping or never starting treatment, or not doing everything possible for the parent, the study found.
The mistrustful young adults were also more likely to still want more information about the parent’s disease, treatment decisions, and death.
The study wasn’t a controlled experiment designed to prove whether or how teens’ experiences during a dying parents’ final days influence mental health later in life.
Another limitation is the potential for factors not examined in the study to impact mental health for these young adults, as well as the potential for teens with psychological problems to be less trustful of medical providers than adolescents without mental health issues, the researchers note.
Still, the results highlight the importance of providing age-appropriate support and grief counseling to children and teens during a parents’ final weeks or months of life, said Dr. Amos Bailey, a palliative care researcher at University of Colorado Medicine in Aurora.
Resources tailored to young people are often lacking outside pediatric hospitals, Bailey, who wasn’t involved in the study, said by email.
“What is at stake for bereaved families is the potential for lifelong mental health problems that are probably more socially significant for a teenager (who) will live with this grief for 60 or more years as opposed to a widow who may outlive her husband by 3-5 years,” Bailey said.
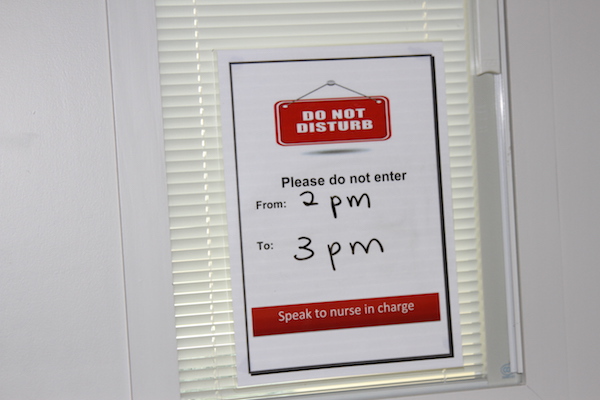
A ground breaking program at Neringah Hospital (Wahroonga, NSW) is meeting the sexual and intimacy needs of people coming to the end of their life.
[W]hile research has shown that patients in palliative care have unmet sexuality and intimacy needs, they are usually not addressed. At Neringah, a 19 bed palliative care hospital, patients and staff are encouraged to normalise topics around sex and sexual desire.
“Sexuality and dying are considered taboo subjects, and most people feel that people in this stage of their lives are too ill to think about sex,” according to Brigitte Karle, Clinical Nurse Educator with HammondCare.
“But our palliative care staff – and our patients – recognise that sexuality is part of the holistic care of patients, and this has resulted in the “Let’s Talk About It” program.
“We need to make it easier for patients, their partners and staff to feel that they can have the conversation without being uncomfortable,” she said.
To facilitate the process patients are advised that they can arrange for a particular sign to be affixed to their door that forbids entry for a certain period.
“Through our research we have identified that patients would like staff to initiate the conversation, and we have implemented a system where staff feel confident to recognise cues to take the appropriate action to provide “Private Couple Time”.
“We also identified a need for staff to have additional training and education so they feel more comfortable about the issue.”
At Neringah Hospital, patients can arrange for a particular sign to be affixed to their door that forbids entry for a certain period.
“Regardless of the setting it is important for all hospitals and staff working in sub-acute care to recognise that people who are in the last stage of their life may have sexual needs,” Ms Karle said.
Ms Karle said Neringah’s unique set up, which included private rooms, allowed patients to have intimate private relationships with their partners that might not be available in other hospitals.
Neringah Hospital Inpatient unit provides short term acute care to patients managing a life limiting illness and is not a long stay facility. The unit provides palliative care for:
short term admission to alleviate symptoms and the distress they cause
holistic care to meet the special needs of patients in the final stages of their illness
The hospital has 13 single beds and three double rooms. The study, Let’s Talk About It, was conducted over an eight month period and involved training for staff and designing ways that patients and their partners could have private time.
Brigitte Karle, Clinical Nurse Educator with HammondCare
In 2016, the first year health-care providers were allowed to bill for an end-of-life consultation, nearly 575,000 Medicare beneficiaries took part in the conversations, new federal data obtained by Kaiser Health News show.
[T]he 90-year-old woman in the San Diego-area nursing home was quite clear, said Dr. Karl Steinberg. She didn’t want aggressive measures to prolong her life. If her heart stopped, she didn’t want CPR.
But when Steinberg, a palliative-care physician, relayed those wishes to the woman’s daughter, the younger woman would have none of it.
“She said, ‘I don’t agree with that. My mom is confused,’ ” Steinberg recalled. “I said, ‘Let’s talk about it.’ ”
Instead of arguing, Steinberg used an increasingly popular tool to resolve the impasse last month. He brought mother and daughter together for an advance care-planning session, an end-of-life consultation that’s now being paid for by Medicare.
In 2016, the first year health-care providers were allowed to bill for the service, nearly 575,000 Medicare beneficiaries took part in the conversations, new federal data obtained by Kaiser Health News shows.
Nearly 23,000 providers submitted about $93 million in charges, including more than $43 million covered by the federal program for seniors and the disabled.
Use was much higher than expected, nearly double the 300,000 people the American Medical Association projected would receive the service in the first year.
That’s good news to proponents of the sessions, which focus on understanding and documenting treatment preferences for people nearing the end of their lives. Patients, and often, their families, discuss with a doctor or other provider what kind of care they want if they’re unable to make decisions themselves.
“I think it’s great that half a million people talked with their doctors last year. That’s a good thing,” said Paul Malley, president of Aging with Dignity, a Florida nonprofit that promotes end-of-life discussions. “Physician practices are learning. My guess is that it will increase each year.”
Still, only a fraction of eligible Medicare providers — and patients — have used the benefit, which pays about $86 for the first 30-minute office visit and about $75 for additional sessions.
Nationwide, slightly more than 1 percent of more than 56 million Medicare beneficiaries who enrolled at the end of 2016 received advance-care planning talks, according to calculations by health-policy analysts at Duke University. But use varied widely among states, from 0.2 percent of Alaska Medicare recipients to 2.49 percent of those enrolled in the program in Hawaii.
“There’s tremendous variation by state. That’s the first thing that jumps out,” said Donald Taylor Jr., a Duke professor of public policy.
In part, that’s because many providers, especially primary-care doctors, aren’t aware that the Medicare reimbursement agreement, approved in 2015, has taken effect.
“Some physicians don’t know that this is a service,” said Barbie Hays, a Medicare coding and compliance strategist for the American Academy of Family Physicians. “They don’t know how to get paid for it. One of the struggles here is we’re trying to get this message out to our members.”
There also may be lingering controversy over the sessions, which were famously decried as “death panels” during the 2009 debate about the Affordable Care Act. Earlier this year, the issue resurfaced in Congress, where Rep. Steve King, R-Iowa, introduced the Protecting Life Until Natural Death Act, which would halt Medicare reimbursement for advance-care planning appointments.
King said the move was financially motivated and not in the interest of Americans “who were promised life-sustaining care in their older years.”
Proponents like Steinberg, however, contend that informed decisions, not cost savings, are the point of the new policy.
“It’s really important to say the reason for this isn’t to save money, although that may be a side benefit, but it’s really about person-centered care,” he said. “It’s about taking the time when people are ill, or even when they’re not ill, to talk about what their values are. To talk about what constitutes an acceptable versus an unacceptable quality of life.”
That’s just the discussion that the San Diego nursing-home resident was able to have with her daughter, Steinberg said. The 90-year-old was able to say why she didn’t want CPR or to be intubated if she became seriously ill.
“I believe it brought the two of them closer,” Steinberg said. “Even though the daughter didn’t necessarily hear what she wanted to hear. It was like, ‘You may not agree with your mom, but she’s your mom, and if she doesn’t want somebody beating her chest or ramming a tube down her throat; that’s her decision.’ ”
Stacie Alves and Dr Julia Spade administer acupuncture and laser therapy to a dog with arthritis. Last Wishes has assisted more than 5,000 families with their petâs care since November 2012. Earlier this year, the organization opened the first compassionate comfort care center for pets in Houston. The center features comfort rooms that are used for hospice and pain management consultations, therapeutic laser, acupuncture, and compassionate sedation-euthanasia.
By Vagney Bradley
People and their pets can build a strong bond together, and losing a pet can be difficult. When a pet becomes terminally ill, Last Wishes, Houston’s first pet hospice service, steps in to take care of a geriatric pet, from moment of diagnosis through death and aftercare.
Dr. Christie Cornelius is the owner and veterinarian of Last Wishes. She also co-owns Earthman Last Wishes, Texas’ first water-based cremation service for pets. Cornelius and her associate, Dr. Julia Spade, will become the first two veterinarians in the state of Texas to become certified in Veterinary Hospice and palliative care in October.
“I started imagining a better way to offer end of life services after a few years of general practice. I saw how difficult it was for pet owners to bring in their painful or otherwise ailing companions into an unfamiliar, sterile, noisy, scary environment for euthanasia,” Cornelius said.
“I started offering home services through a feline practice I was working for at the time and found it extremely rewarding to be able to provide a peaceful passing for a pet in their own environment, surrounded by loved ones. As the years went by, I convinced myself there was a real need and desire for this type of service in our community.”
In 2012, Cornelius branched out and started Last Wishes while working full time at another veterinary clinic.
Last Wishes has assisted more than 5,000 families with their pet’s care since November 2012. Earlier this year, the organization opened the first compassionate comfort care center for pets in Houston. The center features comfort rooms that are used for hospice and pain management consultations, therapeutic laser, acupuncture, and compassionate sedation-euthanasia.
Cornelius’ goal is to help educate the community about pet hospice, comfort care, pain management, and gentle water-based aftercare services for pets.
Dr Christie Cornelius and assistant Betty Rose Bryant perform an exam on a dog.
Some of the common conditions the organization works with includes, but are not limited to, cancer, heart disease, liver disease, osteoarthritis, organ failure, cardiovascular and neurological disease, and vestibular disease.
“Last Wishes is unique in that we want to make the most of the time that every pet has left with their family. Our doctors and staff don’t just focus on making euthanasia as comfortable as possible when it is ultimately needed,” Spade said. “Our expertise in multiple forms of hospice techniques allows us to consider what is truly beneficial for each case and help strengthen the bond between the pet and their family.”
The majority of services are done in the comfort of the family’s home and in the pet’s environment. Services at the center include consultations, acupuncture, laser, sedation-euthanasia, pet loss support groups, and aftercare. Last Wishes also provides pet loss support groups and continuing education.
“We have established a network of providers, such as our very own grief counselor, pet sitters, pet groomers, and volunteers set up to meet all of our patients and family’s needs when it comes to providing care for an ailing pet diagnosed with a terminal disease,” Cornelius said. “In addition, we sponsor twice monthly pet loss groups and host a private Facebook pet loss support page.”
Additionally, the organization assists disadvantaged families and individuals with their pet’s end of life care through the Last Wishes Fund, a non-profit organization funded by public donations.
Last Wishes provides provide a folder of pet loss/grief information for each family, a clay paw print memorial keepsake, and gentle transport of the pet for aftercare services from the client’s home.
“It is such an honor to be invited into the homes and lives of the families of Houston,” said Jennifer Rames, Last Wishes office manager. “While euthanasia is never easy, we feel honored to provide our services so that these precious furry family members can pass with dignity, in the place they feel safest and happiest, and surrounded by the people who love them the most.”
Cornelius and grief counselor, Marilyn Ladin, are developing a pet loss support program. The program offers in-person and online individual and group therapy.
“Our goal is to heal some long-broken hearts,” Cornelius said. “We also aspire to help other veterinarians and veterinary staff struggling with compassion fatigue, depression, and anxiety among other issues. Too many of our colleagues are causing their own deaths.”
This month Last Wishes plans to unveil of a public pet memorial gardens in Cypress. The garden will include four gardens and handmade stepping stones as a tribute to the pets the organization has helped. The memorial will also feature a special Rainbow Bridge. Families will have access to the garden on Sunday mornings as an opportunity to visit their pet in a peaceful and natural setting.