by Kay Bransford
Caught off guard
[T]he final days for both my mom and dad were unexpected. When we got their initial diagnoses in 2012 — Alzheimer’s for dad and vascular dementia for mom — we were told they could live for a decade or more.
Early on, I fought to be their caregiver. Due to the nature of their conditions, they just didn’t recognize how many issues they had managing their day-to-day lives. Eventually, they accepted my help. I adapted to being the primary adult family caregiver and absorbed the additional responsibility to advocate for their needs.
I wasn’t prepared for how hard it would be to make decisions about life and death for my parents. Thankfully, I was very clear on their wishes. I spent most of my adult life living near my parents and visited them two or three times a week. On many occasions, as my parents were watching or caring for their own parents, they would comment on how they would like to be treated.
Over the years, my mom must’ve told me at least a hundred times that “If I end up like my mom, put a pillow over my head.” Obviously, I couldn’t do that, but it reinforced the fact that she wanted quality of life, not just life. My dad wasn’t as conversational about his wishes, but when he would share what was happening to colleagues and friends, we would discuss how our family might face the same situations. In those moments, I also learned what was important to him.
In 2013, after my parents moved into an assisted living community, life and caregiving became much easier, at least for a while. The biggest issue was handling the multitude of calls to come visit. Sadly, my parents never remembered when I visited. They would often call me while I was on the car ride home to ask when I was stopping by.
What’s wrong with dad?
In the spring of 2013, I noticed that my dad was starting to drool, and on some visits, his speech was a little garbled. The staff doctor at the assisted living community didn’t find anything unusual and felt that this was likely related to the Alzheimer’s. I wanted to be sure, so I set up an appointment with a specialist.
The specialist didn’t find anything out of the norm. My parents had dentist appointments coming up, so we decided to wait and see whether the dentist noticed anything unusual.
Unfortunately, the appointments my parents had with the visiting dentist came and went. When it came time to see the dentist, they’d both declined to be seen. They were put back on the dentist’s wait list, but I didn’t want to go that long without conclusive information about dad’s symptoms.
Instead of waiting for the dentist’s appraisal, I requested a swallow consult with the community’s speech pathologist for dad. I was surprised to learn that my dad’s tongue seemed to be paralyzed. My dad was immediately referred to the doctor at the assisted living community. The community doctor found a growth on the back of dad’s tongue and suggested that we see a specialist for mouth cancers right away.
Within a few days, the specialist confirmed that dad had a tumor. The tumor tethered his tongue, which prevented him from being able to move it to swallow or speak clearly. We learned that dad had options for treatment, but they would be extensive: chemotherapy, radiation, and a feeding tube. Thankfully, one of my brothers was able to come to town and help me figure out how to best help our dad.
Deciding what comes next
Two months before the doctor diagnosed dad’s tumor, our parents celebrated their 60th wedding anniversary. As their children, we were proud that we could keep them together as they were both living with similar stages of different types of dementia. There aren’t many options for couples who both need memory care.

Although they were together throughout dad’s new diagnosis, we knew that our mom didn’t understand what dad was facing. What we did know was that they were better as a pair, and we wanted to see if we could get them more time together. We were raised to put up a fight for the things we wanted, and we were prepared to go into battle for dad.
Getting his teeth cleaned by a specialist was the first step in getting treatment for his tumor. In order to get his teeth cleaned, he had to get cleared by a cardiologist for the procedure. This is because they would have to sedate him during the teeth cleaning.
It wasn’t until this meeting with the cardiologist that we realized just how weak he was. During the appointment, dad fell asleep on the examination table, something he would do during the many appointments to come.
We realized that if we moved forward with treatment for the tumor, it would create even more discomfort for our dad. Due to the nature of his dementia, he was already experiencing discomfort in his daily life. It seemed senseless to add yet another layer of suffering when recovery from the tumor wasn’t guaranteed.
We understood that it was time to meet with the hospice doctor to discuss palliative care and make dad as comfortable as we could for the rest of his life. Still, it was hard for us to absorb the reality that our father, a multiwar veteran, was going to die from a cancerous tumor on his tongue.
Dad’s tumor was diagnosed on August 27, 2013, and on September 27, 2013, he passed away in a hospice center. I’m thankful it was swift, but it happened so fast that I was thoroughly in shock, as were we all. Once we realized how much pain he was in, we were happy that he didn’t linger.
For whatever reason, my mom, siblings, and I decided we wanted one last family picture of us surrounding dad’s body. I’ve never seen 5 people look so forlorn in any photograph before or since.
Living with the loss
The coming days, weeks, and months were incredibly difficult to manage. Not only was I grieving for my dad, I was second-guessing my ability to be the family caregiver. I was also trying to figure out how to help my mom who, due to her dementia, couldn’t remember that her husband died.
I am now thankful that we took a picture with dad in his hospice bed — it turned out to be something I could share with my mom. Although many people will tell you to never remind someone with dementia about the loss of a loved one, I felt that it would be more harmful not to tell her.
My mom would spend her time roaming around the community looking for dad and grew increasingly anxious when she couldn’t find him. I wanted her to be able to grieve his loss. When I visited, I would bring pictures of dad, share a happy story about him with mom, and mention how much I missed him.

During the first month after dad’s death, mom became very combative with the other residents; before long, she was getting into physical fights with other people in the community. This was a new behavior for her, and it was unlike my mom to be physical.
I was called in to meet with the community’s director who told me we needed to find a way to help my mom manage better in the community or she would have to move out. They suggested we hire a personal care assistant (PCA) to help her manage her day. We realized that it was time to start looking into a community specifically for people who need memory care.
Helping mom adjust
We immediately hired a PCA after meeting with the community’s director. Due to her dementia, mom already had some issues with paranoia. Unfortunately, bringing a PCA in only made mom more paranoid. She felt like someone she didn’t know was constantly following her.
Mom was generally suspicious of suggestions from someone she didn’t know well. This meant that she had a hard time connecting with most of the residents and staff in her community. Without dad, she was truly alone much of the day.
I also hired an aging life care manager to help me find the best memory care community for mom. She helped me understand and recognize the key attributes of a good memory care community.
We needed a community with:
- scheduled activities that my mom would enjoy
- active reminders about upcoming activities or events so my mom wouldn’t miss out
- a standardized menu so that mom didn’t have to figure out how to piece together a menu of her own
- community cues to help mom recognize how to get to her apartment
Assisted living communities are designed to help people navigate physical limitations in order to complete daily functions and activities. They don’t offer activities designed for people with memory issues, and they aren’t staffed to deal with the types of behavior, like paranoia, that might present in someone with dementia.
Before we could finalize the details of mom’s move, she had a major setback. She had been complaining about back pain, so her doctor prescribed her Tramadol. Mom ended up on bedrest and behaved as if she were on hallucinogenic drugs.
We later found out that the medication caused this reaction because of the type of dementia that she had. Her doctor said that this wasn’t uncommon, but it wasn’t something we were prepared for. The possibility of such a reaction was never mentioned to me when she was receiving her prescription.
It took nearly 3 weeks for the drug to work its way out of her system. She spent so much time in bed recovering that she became weak and unsteady. Several months passed before she was able to walk on her own again.
Once mom was stable, we moved her into a memory care community. We moved her on January 17, 2015. We knew the transition would be difficult. Often, for people with dementia, switching residences can result in a recognizable decline. Although she adapted quite well, she had a fall that landed her in the emergency room after only a few months in the new community.
She was unable to fully recover from the fall and could no longer walk unassisted. To make matters worse, mom would never remember she wasn’t steady on her feet. She would try to get up and go whenever the notion struck her. To keep her safe, we brought a new PCA back on staff.
Mom lived in the memory care community for nearly a year. We were lucky to have found a PCA that doted on mom and that mom trusted. She would do mom’s hair and nails and made sure she was active and engaged in activities. It was nice to have someone I could contact to know how mom was doing on a daily basis.
Saying goodbye to mom
In December 2015, mom tipped over while washing her hands. She never hit the ground, but she complained of hip pain, so she was taken to the ER. When I arrived, I immediately recognized the significance of her injury.
Sometimes, when bones grow frail, a simple twist is all it takes to break a hip. While they took mom to X-ray, I found a private restroom and sobbed. I knew that elderly women who break a hip are at an increased risk of dying within a year of the incident.
When I met with the orthopedic surgeon, she confirmed that mom’s hip was broken. She told me that she couldn’t operate until I lifted mom’s Do Not Resuscitate (DNR) order. I was taken aback by the surgeon’s request.
When I asked her why, she said that they’d have to put in a breathing tube. I told her that if my mom died on the table she wouldn’t want to be brought back to a life with dementia. The surgeon repeated that to make mom comfortable, we should operate, and to do that, I needed to lift the DNR order.
I called the aging life care manager back in and a geriatric doctor to help me navigate my choices for mom. The geriatric doctor told me that mom most likely wouldn’t be strong enough to qualify for surgery. A few tests had to be run before we even needed to worry about the surgeon’s request.
The first test identified a heart and lung issue, eliminating the option for surgery. Mom’s body just wasn’t strong enough, and it was easy to see how much pain she was in.
She was alert even after four courses of morphine. She didn’t really understand what was going on. And at some point during her stay at the ER, she had a small stroke. My mom no longer recognized me, and she was unable to remember that she had children.
It had become clear that our only choice was to move mom into hospice care. Her health was fading fast, and we wanted to make her last days as comfortable as possible. We moved mom back to her community where she had 24-hour support and hospice care. I called all of my siblings and they scheduled one last trip to see mom.

Over the next week, mom mostly slept. Every day, I’d arrive with lotion and rub her feet. By the end of each visit, I would end up crying at the foot of her bed. I told her how much I would miss her, but reminded her that dad was patiently waiting for her to join him.
When I visited her on Christmas Day, her breathing was jagged. I knew she didn’t have much longer. The memory community nurse called at 5:35 p.m. to report that mom had passed away. Even though I felt it coming, I was still stunned. Thankfully, my husband and children were with me when I received the news. They were able to take me to see mom one last time and say my goodbye.
Learning to live with my decisions
If I knew how things were going to progress, I feel like I would have made many different decisions throughout my caregiving journey. It’s hard not to second-guess the decisions that I made during my time as caregiver.
A wonderful social worker told me that I should forgive myself, because I made the best decisions that I could with the information I had at the time. I’m still reminding myself of that. I often share this advice with other caregivers who feel the same remorse about their caregiving journey.
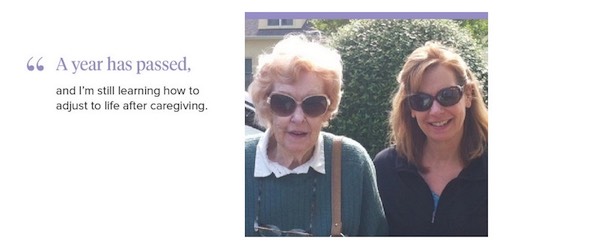
A year has passed, and I’m still learning how to adjust to life after caregiving. I was told quite often to be kind to myself during my journey. Now that my family caregiving journey is over, I believe that this is the best advice I was ever given. I hope that after reading about my experiences, you can take this to heart and find peace on your journey.
Life after caregiving
While I was caring for my parents, I started to build a part-time business focused on helping other caregivers. I wanted to help other caregivers navigate challenges like the ones I was facing — managing doctor’s appointments, getting finances in order, and maintaining a second home.
This part-time business would become MemoryBanc. For several years, I balanced work by limiting the number of clients I helped so that my parents would always be the priority. When I was grieving my mom’s passing, I realized how much I enjoyed being able to help her lead the life she wanted.
After a few months, I started to take on more clients. It felt good to be able to put my caregiving journey behind me, but also to use what I learned to make me a valuable resource for so many other families. While I still have moments of sadness, I’ve been able to focus on the great lives my parents lived instead of dwelling on the last few years we had together. I’m still adjusting to my new normal.
Complete Article HERE!