People left their seats to dance and sing along to a live performance of “Mustang Sally” while servers waited in the next room, poised with champagne and chocolate-covered strawberries.
This was not your typical funeral.
Hundreds of family, friends, and members of the public turned out for Audrey Parker’s celebration of life.
Audrey Parker wanted her friends and family to be uplifted by the ceremony and so she planned every detail with that aim before she died on Nov. 1.
“She planned it and she knew that when we walked out of here today we would remember that life is supposed to be a celebration. This is a celebration of life, not just Audrey’s but all of ours,” said her friend Nancy Regan, the master of ceremonies.
Several hundred people gathered at Pier 21 on Friday afternoon to commemorate Parker, the 57-year-old Halifax woman who chose to die with medical assistance as she faced a terminal cancer diagnosis.
Many of the speakers mentioned how popular Parker was, with a large and adoring group of friends and a close-knit family who made up much of the crowd. But the ceremony was also open to the public, who came to know Parker in the final months of her life as she advocated for change in Canada’s assisted dying legislation.
Parker left two legacies: one for the people who knew her and were inspired by her exuberant kindness and another for those in the public who were spurred to take a closer look at a complex law.
“I’m gonna get a little political now, because I want to talk about Aud’s legacy,” said her friend Kimberley King, the last of seven speakers at Friday’s ceremony.
“Audrey knew that she wanted to be a spark, but she never imagined she’d be a national advocate,” King said.
Parker was diagnosed with Stage 4 breast cancer in 2016 and as her illness progressed she experienced excruciating pain from tumours in her bones. She was approved by a doctor for medical assistance in dying (MAID), but as it stands, the law stipulates that patients must give late-stage consent.
It’s a safeguard that’s meant to protect people in a vulnerable state — such as when their physical health and mental faculties may be failing — but Parker said that in her circumstance, all it did was cut her life even shorter.
“I really wish that we had her this Christmas,” said her stepdaughter, Lucie MacMaster, after reflecting at Friday’s ceremony on past holidays they’d shared.
“But here we are,” she added.
Parker chose Nov. 1 for her final day because she knew that she would still be able to give the necessary late-stage consent. The cancer has recently spread to the lining of her brain, and she worried that if she waited much longer, the opportunity would be lost.
Before she died, Parker called on Ottawa to amend MAID so that people like her could give advance consent for their own death. It could not be amended in time for her, but she asked the public to keep pushing for the change.
“She did her part, and now it’s our turn. In Audrey’s honour and memory, I ask you to continue to support her movement. We have an opportunity to amend a federal law so that people who are invoking MAID don’t need double consent and therefore don’t need to die early like our Audrey did,” said King.
Local MLA Darren Fisher has said he’d like to see the legislation go “a little bit further,” but Justice Minister Jody Wilson-Raybould disagreed, telling reporters the day after Parker’s death that there were no plans to change the two-year-old law.
Parker’s friend Robert Zed announced on Friday that there will soon be a permanent memorial for Parker in Halifax’s Point Pleasant Park. A steel bench is to be installed on Monday, facing out toward the water on Sailors Memorial Way.
Mom’s terminal cancer diagnosis took her by surprise. “I always thought I would just fall over dead while I was walking across the backyard,” she told me. “Not me,” I responded. “I’m planning to go out like Uncle Ernest: Go to bed healthy and wake up dead. I think it’s called cardiac arrest.”
We were sitting at Mom’s kitchen table, trying to pretend everything was OK. A few years earlier, Mom had flitted away “a little bit of cancer,” as she called it, with a lumpectomy carefully timed so she did not miss her volunteer gigs. But we knew that this time — two cancers and increasing shortness of breath — was going to be different.
We tried to focus on the peach cobbler in our bowls. In our minds, though, we were coming to grips with the fact that we had fooled ourselves.
Mom and I thought of ourselves as great planners. Our pantries always well-stocked; the menu always worked out weeks before the big family dinner; a hundred-dollar bill always tucked in the sock drawer, just in case.
Mom’s End-of-Life Plan
Mom’s end-of-life plan was to die quickly. It turns out that is not a plan; it’s a hope. And the difference proved terribly sad when it came to the living will she’d prepared (a living will is an advance directive spelling out your desires regarding medical treatment if you’re no longer able to express them).
Like every good planner, Mom had a Plan B if she didn’t get the sudden death she was counting on. She was such an enthusiast for having a living will that I teased her about handing out copies like they were campaign flyers. When she turned 65 or thereabouts, she presented a copy to each of us four kids, her siblings and her doctor, along with a warning that “if you keep me alive on machines, I’ll come back to haunt you.”
That made us laugh. Mom was as threatening as a worn-out quilt. And after Dad died, when they were both in their mid-50s, she devoted the next three decades to making other people’s lives easier. She was a cookie-baking grandma happy to babysit on five minutes notice; the lady who made hash brown casseroles for bereavement dinners at her church.
Mom’s Living Will
Looking back, I wonder where she got all those copies of her living will. In my mind’s eye, I see her — super-white tennis shoes and polyester slacks — standing next to the copy machine at the library, fishing dimes out of her coin purse, while a young library intern pushed the button. “I better get a couple more copies, if you don’t mind. My kids lose things like you wouldn’t believe,” she might have said.
We all knew the living will was Mom’s way of saying she didn’t want to die like my dad did, suffering horribly from lung cancer treatments known to be futile even before they started.
What we didn’t know is that she would suffer horribly because we didn’t adequately plan for her end-of-life care — and that the living will would prove useless.
Our Big Mistake
Mom was of the “whatever you think is best, doctor” generation, but none of her kids are wallflowers. Yet we were unprepared to advocate for Mom’s end-of-life preferences, so we politely acceded to her physician’s auto-pilot protocol of tests and specialists in unfamiliar medical centers and painful blood draws even though Mom was clear from the outset that there would be no chemotherapy and radiation.
Years earlier, my cousin had complained about the hospice nurse that cared for her dad, but I changed the subject, murmuring about how nice the funeral was. So I missed the opportunity to find out what had gone wrong, what was the name of the hospice and, most importantly, how we could avoid the same mistake if we needed hospice services in the future.
That turned out to be our big mistake.
We were caught off-guard on the day that Mom was too weak to get out of bed and I couldn’t turn her. Although we did have options (in-home help, inpatient hospice in the city 75 miles away or the local nursing home), during Mom’s months-long decline, we had not discussed them because we were hoping —there’s that word again — we wouldn’t need them.
The Hospice Trouble We Encountered
I woke up that morning, expecting another day of helping Mom from her lift chair to wheelchair to toilet to hospital bed. When we realized it was not to be, I panicked. I administered the first dose of morphine for the day and, as Mom dosed, started frantically trying to make a plan that should have been made weeks earlier.
The home care agency in her town, it turned out, only served patients not on hospice; they had a list of nurses who moonlighted, but nobody could be arranged on short notice.
The inpatient hospice had an opening, but that would mean Mom spending her last days in the city, too far for her five siblings to visit. Would she want that? In her frail and despairing condition, I couldn’t bring myself to ask.
So we headed to the nursing home, where Mom died 10 days later.
Before all this, I would have said that our one end-of-life plan was that Mom would not die in a nursing home that was just as miserable as we all feared it would be. But what I really meant was that was our hope. We didn’t have a plan.
Virtual reality may be able to transport you to spectacular other worlds, but a large part of its promise is the ability to also put you into the shoes of other people. In doing so, the hope is that VR could help make us more empathetic, since it gives us the ability to literally experience life from another person’s perspective.
That’s what VR studio Embodied Labs hopes to do. Based in Los Angeles — arguably the entertainment capital of the world — Embodied Labs wants to use cutting edge virtual reality to do something more than provide escapism. It wants to use it to promote empathy. And it wants to do it in such a way that can help train tomorrow’s caregivers.
We’ve previously covered Embodied Labs’ work creating a virtual experience intended to simulate the effects of Alzheimer’s disease. Called “The Beatriz Lab: A Journey Through Alzheimer’s Disease,” it follow the fictitious character Beatriz, a math teacher in her 60s, as she grapples with the neurodegenerative disease. Now Embodied Labs is back with another virtual training tool, this time designed to function as an end-of-life simulation for educating staff and medical students in hospices, hospitals, and universities. It’s currently being used at the Gosnell Memorial Hospice House in Scarborough, Maine, as well as by medical students at the University of New England.
Meet Clay
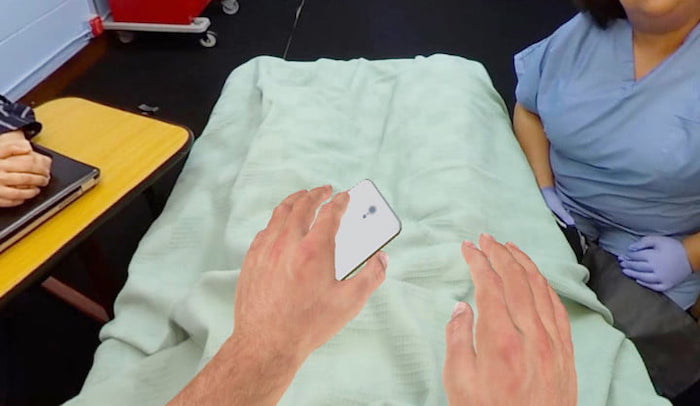
The 30-minute simulation places users in the role of “Clay,” a 66-year-old lung cancer patient in need of hospice care. During the course of the VR story, Clay has important conversations with family, suffers a fall that puts him in the E.R., and eventually winds up in hospice care. Through simulating physical changes in virtual reality — such as how Clay’s skin alters and his senses dull — the user also gets to feel some approximation of what it would be like to experience end-stage cancer. By the end of the experience, Clay’s eyesight becomes dim as his life comes to a close. For anyone who associates VR predominantly with gaming, the effect is surprisingly poignant.
“The embodied experience includes receiving a terminal diagnosis from your oncologist, counseling from your case manager, and care from your hospice provider and family, and ultimately, it involves reaching the end of your life,” Erin Washington, co-founder and COO at Embodied Labs, told Digital Trends. “By embodying Clay, people gain insights into challenges faced by patients and families when curative treatment is not available, learn how hospice care supports loved ones, and explore the physical, spiritual, and mental changes that may occur at end of life.”
Through its painstakingly created and very human VR experiences, the company has cornered the market on a type of next-generation training tool. It provides an experience that caregivers or clinicians cannot get simply by reading textbooks.
“Embodied Labs creates immersive training and wellness tools for healthcare students, and for professional and family caregivers, so they can feel more empowered and confident in having the difficult conversations that surround end-of-life decisions,” Washington continued. “Organizations such as skilled nursing facilities, medical schools, hospice and home care agencies, and assisted-living providers use Embodied Labs to improve outcomes, operations, and culture.”
In addition to creating its experiences, Embodied Labs creates customized assessment questions to be answered before and after staff and students sample a VR scenario. This qualitative and quantitative data can then be used to provide new insights, on the part of professionals, into things such as how conversations about end-of-life are carried out.
Building empathy
But does this actually work, or is this a case of creating a solution to a problem that doesn’t actually exist? In fact, according to a new piece of research, virtual reality really be prove to be a useful tool in encouraging empathy.
In a study published this month in the open-access journal PLOS ONE, researchers from Stanford University compared the attitudes of people who had read a first-person narrative piece of writing about homelessness, those who had experienced a 2D interactive narrative about it on computer, and those who had undergone a perspective-taking VR scenario on the same topic. They found that the people who had experienced the VR simulation were more likely to sign a petition to support homeless populations. Follow-up surveys also found that they experienced longer-lasting empathetic feelings than those who had done the narrative-reading task.
Of course, there are problematic aspects with the idea of building empathy through VR. A 30-minute simulation about end-of-life conversations is not the same thing as experiencing it for real. A person really experiencing the effects of homelessness or discriminatory activity cannot simply take off their headset when they decide they’ve had enough of their life circumstances. Attempts to “gamify” complex scenarios risk inadvertently diminishing them, and carry the chance of turning something intended for good into something exploitative.
However, properly considered, there is room for virtual reality as a teaching tool. Certainly, it needs the proper care and attention of trained professionals, and it shouldn’t be considered a substitute for other forms of teaching. But as something that we’re glad to see being explored? Absolutely. And if it potentially means more empathetic treatment for yourself and your fellow human beings, you should be, too.
Librarian Marissa Lamer has come to appreciate the powerful messages that can be relayed in graphic novels.
ByMarissa Lamer
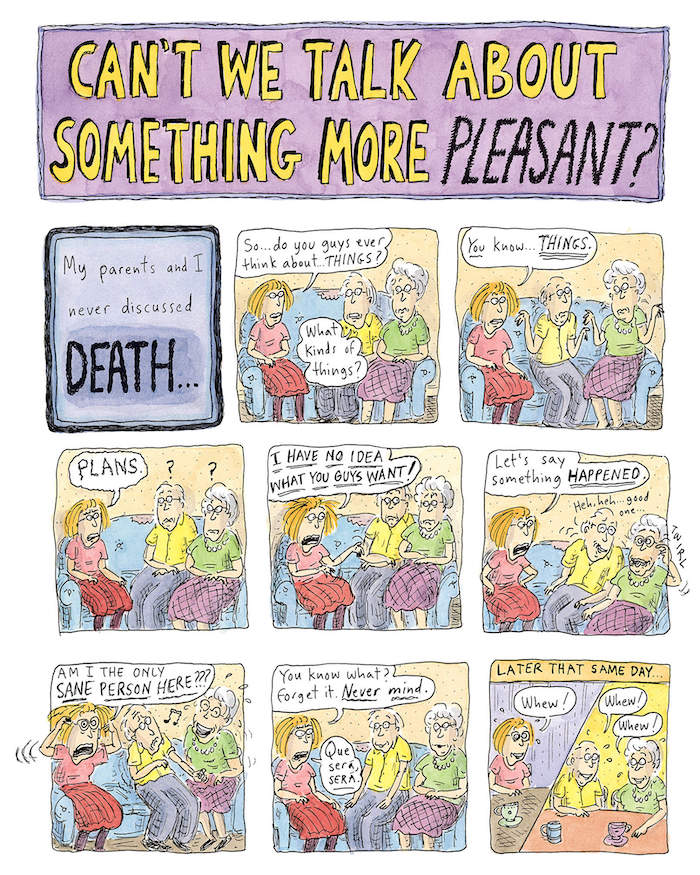
Can’t We Talk About Something More Pleasant? by Roz Chast is a compelling graphic memoir about the struggle Chast goes through as she watches her parents age and eventually die.
Although I have seen my parents grieve the loss of three of my grandparents, I have not yet experienced that kind of loss firsthand. And it’s definitely not an experience my parents felt necessary to discuss with me or vice versa.
People don’t talk about death and dying in our culture, even though it affects every single person at some point in their lives. However, Chast’s memoir broached the subject in such an endearing and accessible way that it got me thinking: what is it about graphic memoirs that make addressing such difficult, even taboo topics more approachable than a traditional novel?
Hello, this is Marissa Lamer for the Radio Readers Book Club and I am coming to you from the public library in Hays, KS. Growing up I was rarely exposed to any type of graphic novels and comics. As I worked my way through college towards a career as a librarian, graphic novels became a genre of literature that grew increasingly intriguing, especially ones that were memoirs and nonfiction. I hesitantly started with a small graphic novel every now and then but have slowly come to truly enjoy and appreciate the value they add to reading.
Can’t We Talk About Something More Pleasant is a blend of comic strips and paragraphs of memoir. Chast finds the humor in an otherwise depressing time in the life of both her and her parents. For example, her mother’s increasingly outlandish stories help ease the pain of death reflected in more somber moments like when Chast stated “I could see that they were slowly leaving the sphere of TV commercial old age and moving into the part of old age that was scarier, harder to talk about, and not a part of this culture.”
The illustrations provide context and a visual for the parts of Chast’s story that are the most emotional and difficult to express in words.
Graphic memoirs like Chast’s make tough topics more accessible. They provide an abundance of extra layers in the writing style, illustrations, and format of the book that a traditionally written memoir cannot provide.
Scholar Eileen M. Richardson describes this advantage, “graphic novels are more than just stories with pictures; they have engaging illustrations that help readers infer the emotions and motivations of characters as well as more fully understand the twists and turns within the plot.”
Using visuals along with text can provide greater insight into the human condition and subjects that are tough to talk about or lay outside our cultural spheres.
Can’t We Talk About Something More Pleasant? is just the tip of the iceberg when it comes to graphic novels exploring thought-provoking subjects.
Here are a few to add to your reading list: Maus by Art Spiegelman is a two-volume, Pulitzer-Prize-winning graphic novel. The only graphic novel to be awarded such an honor. Animal characters are used to stereotype different races and nationalities illustrating the story of Spiegelman’s parents surviving the Holocaust and his relationship with his father.
Persepolis by Marjane Satrapi is another two-volume memoir of a girl growing up in Iran during the Islamic Revolution. It paints a vivid portrayal of life in Iran during a turbulent time through the eyes of a child.
The March trilogy by John Lewis and Andrew Aydin has won multiple awards and chronicles Lewis’ thoughts, feelings, and experiences throughout the Civil Rights Movement. The illustrator uses emotional black-and-white imagery which captures the raw emotion of people portrayed during this pivotal time in history.
Once again, this is Marissa Lamer coming to you from Hays for the Radio Readers Book Club. I hope you have enjoyed reading Can’t We Talk About Something More Pleasant? and the next time you are deciding what to read, you consider adding a graphic memoir to the list.
We had started down the path of honoring our mother’s wish to have a good death until a hospice nurse figured out that she wasn’t really dying.
Monona Yin, right, with her mother, Fay Hoh Yin, and brother, Duncan Yin.
By Monona A. Yin
Three years ago, my family and I had the experience of going through a full “dress rehearsal” for my mother’s demise. At 83, she had become alarmingly weak from stage IV lymphoma and atrial fibrillation, and asked me and my brother to come home to Delaware for her next oncologist visit.
Mom had already undergone chemotherapy and cardioversion, so we knew there were few treatment options left. Still, we were utterly unprepared when the doctor said, “She probably has less than six months,” and recommended that she begin hospice care.
Widowed at just 37 with two small children, Mom has trained herself to face challenges without flinching. She is that rare Chinese elder who isn’t superstitious about mentioning or planning for her own death.
True to form, when we got home from the oncologist’s office, Mom sat us both down at the kitchen table to discuss her end-of-life wishes. She had witnessed two horrible lingering deaths up close — her mother’s and a longtime friend’s. What she feared most was pointless suffering and the loss of control over her own life. She wanted us to understand that, if she had little hope of recovery, she’d rather go quickly than fall apart slowly and painfully.
My brother, at the other extreme, wanted Mom to pursue every medical option, no matter how long the odds. He believed that doctors were fallible, there was always another treatment out there, and life was worth clinging to. And he couldn’t bear the thought of living without her.
Then there was me, torn between them. I had spent hours listening to Mom’s fears and understood them. A decade earlier, my mother-in-law had died with a feeding tube in her side while her oncologist suggested more surgery — after six months of wasting away from metastatic cancer. It would have been infinitely kinder to allow her to die peacefully in her own bed.
We had given my paternal grandmother just such a “good death.” We sat by her bed and told family stories as she slipped into unconsciousness. We turned away from the outside world and drew close to one another. All was quiet and time seemed to stop. Finally, we held her as she took her last breaths, letting her know how much we loved her but also letting her go. I remember that week as a thing of rare beauty. It taught me that dying well can be a balm and a blessing to all involved.
Recognizing the enormous gulf between those two scenarios, I supported Mom’s right to die on her own terms. Like my brother, I desperately wanted more time with my mother. Despite her failing body, Mom’s mind remained sharp. In recent years, our occasional mother-daughter tensions had subsided, leaving a much warmer and less complicated companionship.
After an emotional week of debate, we all agreed to bring Mom to New York for a second — and final — opinion from the world-class doctors at Memorial Sloan Kettering. If they too determined that nothing more could be done, we would accept the inevitable.
At Sloan Kettering, Mom went through the scans without incident but afterward her blood pressure dropped dangerously low and she was admitted as an inpatient.
By the next night, Mom could hardly breathe at all. It was agonizing to watch her gasping for air. She was terrified of suffocating and on the verge of panic. Finally, she pulled me close to say, “Tell them to stop everything.”
I had promised to honor her wishes, so I found a doctor and activated her D.N.R. In a few minutes, my husband, Steve, and our 14-year-old daughter, Maya, arrived and Mom couldn’t hold back her sobs. “I’m so sorry I won’t see you grow up! I’m sorry I won’t see you graduate or get married!”
We had all been coming to terms with Mom’s mortality for months but the shock and pain were still overwhelming.
Then something that seemed miraculous happened. A hospice nurse, Tracy Kahn, arrived and went in to check on Mom. She came back to tell us that she didn’t think Mom was going to die that night, the next night, or maybe for weeks.
Based on years of observing hospice patients, Tracy did not believe Mom was dying of cancer right then.
Instead, without our realizing it, her heart had been severely weakened by the cardioversion, which required high doses of a toxic drug. Almost two liters of fluid had accumulated in the lining of her right lung.
We immediately reversed the D.N.R. but it would be another 10 days before Mom grew strong enough to have the fluid drained. Over the next month, the hospital’s lymphoma, cardiology and pulmonary teams worked together to bring Mom back from the brink. They administered steroids, gave her blood transfusions, stabilized her immune system, optimized her diuretic and treated her infections.
Mom transferred to a rehabilitation center for another month, then came to live with me in Brooklyn. With our newfound sense of “now or never,” Mom and I fulfilled one of her longtime dreams. We edited and self-published her memoirs, which she’d been writing for years, and she’s enjoyed positive reviews from friends and strangers alike.
Today, Mom still wrestles with neuropathy, shortness of breath, and sometimes crushing fatigue — but she is very much alive. Even more amazing, she has been living on her own for the past two years.
We’ve had time to reflect upon our decisions, how we influenced one another, and what we’d do differently. My central insight is that it took all three of us to steer clear of the twin shoals of dying too soon and dying too late. We made better decisions because we listened to one another and weighed all the conflicting information. In hindsight, my mother acknowledges that she wanted to “pull the plug” too soon because she became overwhelmed by fear.
No one thinks clearly in the grip of panic. That’s why it’s so important to start talking long before the end. Not merely about what constitutes a good death but, more important, what makes even a diminished life worth living. As Atul Gawande writes in “Being Mortal,” “Our ultimate goal, after all, is not a good death but a good life to the very end.”
The end-of-life conversation is equally important to both sides — the dying person and the survivors. One of my mother’s greatest comforts is knowing that her children understand her wishes and will honor them. We proved that during the dress rehearsal.
Only recently have Mom and I realized how much it cost me to be her health care proxy, rather than a grieving daughter who wanted to do anything to save her mother. I’m still going to be torn between those two roles “the next time” but simply being aware of that inner conflict helps mitigate it. And Mom’s future decisions will be informed by all the joy she would have missed had she died that night in late 2015.
“Grief is a force of energy that cannot be controlled or predicted. It comes and goes on its own schedule. Grief does not obey your plans, or your wishes. Grief will do whatever it wants to you, whenever it wants to. In that regard, Grief has a lot in common with Love.”
By Maria Popova
“All your sorrows have been wasted on you if you have not yet learned how to be wretched,” Seneca told his mother in his extraordinary letter on resilience in the face of loss. One need not be a dry materialist to bow before the recognition that no heart goes through life unplundered by loss — all love presupposes it, be it in death or in heartbreak. Whether what is lost are feelings or atoms, grief comes, unforgiving and unpredictable in its myriad manifestations. Joan Didion observed this disorienting fact in her classic memoir of loss: “Grief, when it comes, is nothing like we expect it to be.” And when it does come, it unweaves the very fabric of our being. When love is lost, we lose the part of ourselves that did the loving — a part that, depending on the magnitude of the love, can come to approximate the whole of who we are. We lose what artist Anne Truitt so poetically termed “the lovely entire confidence that comes only from innumerable mutual confidences entrusted and examined… woven by four hands, now trembling, now intent, over and under into a pattern that can surprise both [partners].”
But we also gain something — out of the burning embers of the loss arises an ashen humility, true to its shared Latin root with the word humus. We are made “of the earth” — we bow down low, we become crust, and each breath seems to draw from the magmatic center of the planet that is our being. It is only when we give ourselves over to it completely that we can begin to take ourselves back, to rise, to live again.
How to move through this barely survivable experience is what author and altogether glorious human being Elizabeth Gilbert examines with uncommon insight and tenderness of heart in her conversation with TED curator Chris Anderson on the inaugural episode of the TED Interviews podcast.
Gilbert reflects on the death of her partner, Rayya Elias — her longtime best friend, whose sudden terminal cancer diagnosis unlatched a trapdoor, as Gilbert put it, into the realization that Rayya was the love of her life:
Grief… happens upon you, it’s bigger than you. There is a humility that you have to step into, where you surrender to being moved through the landscape of grief by grief itself. And it has its own timeframe, it has its own itinerary with you, it has its own power over you, and it will come when it comes. And when it comes, it’s a bow-down. It’s a carve-out. And it comes when it wants to, and it carves you out — it comes in the middle of the night, comes in the middle of the day, comes in the middle of a meeting, comes in the middle of a meal. It arrives — it’s this tremendously forceful arrival and it cannot be resisted without you suffering more… The posture that you take is you hit your knees in absolute humility and you let it rock you until it is done with you. And it will be done with you, eventually. And when it is done, it will leave. But to stiffen, to resist, and to fight it is to hurt yourself.
There’s this tremendous psychological and spiritual challenge to relax in the awesome power of it until it has gone through you. Grief is a full-body experience. It takes over your entire body — it’s not a disease of the mind. It’s something that impacts you at the physical level… I feel that it has a tremendous relationship to love: First of all, as they say, it’s the price you pay for love. But, secondly, in the moments of my life when I have fallen in love, I have just as little power over it as I do in grief. There are certain things that happen to you as a human being that you cannot control or command, that will come to you at really inconvenient times, and where you have to bow in the human humility to the fact that there’s something running through you that’s bigger than you.
Illustration from Cry, Heart, But Never Break, a Danish meditation on love and loss
Gilbert goes on to read a short, stunning reflection on love and loss she had originally published on Instagram:
People keep asking me how I’m doing, and I’m not always sure how to answer that. It depends on the day. It depends on the minute. Right this moment, I’m OK. Yesterday, not so good. Tomorrow, we’ll see.
Here is what I have learned about Grief, though.
I have learned that Grief is a force of energy that cannot be controlled or predicted. It comes and goes on its own schedule. Grief does not obey your plans, or your wishes. Grief will do whatever it wants to you, whenever it wants to. In that regard, Grief has a lot in common with Love.
The only way that I can “handle” Grief, then, is the same way that I “handle” Love — by not “handling” it. By bowing down before its power, in complete humility.
When Grief comes to visit me, it’s like being visited by a tsunami. I am given just enough warning to say, “Oh my god, this is happening RIGHT NOW,” and then I drop to the floor on my knees and let it rock me. How do you survive the tsunami of Grief? By being willing to experience it, without resistance.
The conversation of Grief, then, is one of prayer-and-response.
Grief says to me: “You will never love anyone the way you loved Rayya.” And I reply: “I am willing for that to be true.” Grief says: “She’s gone, and she’s never coming back.” I reply: “I am willing for that to be true.” Grief says: “You will never hear that laugh again.” I say: “I am willing.” Grief says, “You will never smell her skin again.” I get down on the floor on my fucking knees, and — and through my sheets of tears — I say, “I AM WILLING.” This is the job of the living — to be willing to bow down before EVERYTHING that is bigger than you. And nearly everything in this world is bigger than you.
I don’t know where Rayya is now. It’s not mine to know. I only know that I will love her forever. And that I am willing.
Onward.
Gilbert adds in the interview:
It’s an honor to be in grief. It’s an honor to feel that much, to have loved that much.
Hundreds of thousands of people have already discussed the last great taboo at one of Michael Hebb’s ‘death dinners’. Here he offers some advice for the rest of us
Two things preoccupy the US writer Michael Hebb – food and death – and he has managed to combine them in his new book, Let’s Talk About Death Over Dinner. It is the product of an idea he had five years ago when he set up an organisation called Death Over Dinner, whose goal was to bring disparate (and sometimes desperate) people together over an informal meal to talk about what is so often a taboo subject. Since then there have been more than 200,000 “death dinners” all over the world. The new book charts the gentle revolution Hebb initiated, as well as offering prompts for readers who want to organise their own death dinners and guidance on coming to terms with the loss of family and friends, and with our own mortality. No one, after all, is going to get out of this alive.
“The way we die in western society is broken,” says Hebb. Now 42, he was 13 when his father died, leaving a gap that he felt his mother and immediate family were unable to properly address. “I had a hunch that open conversation about our end-of-life wishes could be the most impactful thing we could do to heal that system and to heal the way we die. We are death-illiterate, and when we don’t discuss death we are not empowered to make decisions.” In a long phone conversation from his home in Seattle, he spells out his philosophy for dealing with dying. You may not be able to conquer death, but you can at least exercise some control over how it happens.
1. Remember you will die
Hebb says we have “ingrained cognitive bias” not to talk about death because we don’t really believe in our own mortality. “We believe we are an exception to basic rules,” he says. “If we haven’t experienced something, it’s hard to know it or to discuss it.” But there are no exceptions, and sooner or later you will have to confront it.
2. Talk now, not later
“Death is a reality for all of us,” Hebb says. “How prepared do we want to be? How comfortable? How much grace do we want to have in the face of it?” He argues that it is better to talk about death when you are well than when you or your parents or other members of your family are terminally ill. “Thinking and talking about death can identify how you want to live,” he says. “If we haven’t made ourselves comfortable with this conversation, we end up being oppressed by it.”
3. It’s not true that you die alone
Before talking to Hebb, I was doubtful that the living could relate meaningfully to the dying. My father died last year and, in the five months that were left to him after he was diagnosed with terminal cancer, I found it hard to find the right words to address what was happening to him or to know how to use what limited time we had together. Everyone, I surmised, had to face death alone, to make their own peace, but Hebb disagrees. “Dying is a realm with no experts, but my sense is that you can reduce the suffering of those who are dying by being as present as possible to them. A lot of people already start dying when they’re diagnosed, but you can live while dying. There is much to be gained from being present until the final chapter. It has the potential for deep connection. I’m not going to gleefully state that dying is a happy time, but I do know that people grieve longer when they don’t know how to honour the person who has died.”
4. Where there’s a will there’s a way
“Statistics show we are very unprepared for death,” says Hebb. “Most people don’t have their end-of-life documents in order.” Sixty per cent of adults in the UK have not made a will; in the US, that figure is 57%. For Hebb, this isn’t just foolish at a practical level; it suggests an unwillingness to talk about death at all. “The documents are important, but more important are the nuanced conversations. If somebody is going to be your health proxy or advocate for you when you are unwell, you want them to have more than just a signed legal document. You want that person to have an entire forest of information about how you feel about end of life.” He says that if you give someone power of attorney to conduct your affairs in the event of you becoming incapacitated, you need to make sure that person really understands you. Spell out exactly what you want in terms of end-of-life care, perhaps through an advance care directive or a living will; do not assume your proxies will make the right calls.
5. Decide what sort of funeral you want
Specifying what you want in terms of your funeral and disposal of your body can be important to the dying. But it may be even more important to the grieving family. “If it makes somebody’s last years more peaceful knowing that their wishes will be fulfilled, then fantastic, but communication is really a gift to the people you leave behind. It’s an important element of the moving through and getting on with their lives.” Making it clear that you do not want a gun carriage pulled by six white horses, or choosing a cardboard coffin rather than a fancy mahogany one with brass handles, can also save a fortune and keep relatives out of the clutches of funeral directors who may be tempted to oversell. How much is spent on a funeral is not a measure of the love felt for the departed.
6. Think about your legacy
Fretting about your legacy seems to me a pointless act of ego, but Hebb disagrees. “Many people do work in this world that they want to extend beyond their death. Some of that can be seen as ego, but some of it is humanitarian in nature, and I think it’s OK to want to have a continuing impact. If that’s what gives your life meaning, I’d say embrace it.” Above all, though, he says, don’t make your legacy suffering and confusion. “You will have a legacy. Everybody has a legacy. So often in families when these things aren’t discussed, there is infighting. For me, it’s not enough to say child A, B and C gets X, Y and Z; if they can have some understanding around your decisions, it’s less likely to haunt them.”
7. Be ready to talk to children about death …
You should involve children in your conversations about death, with one proviso – that you go at the pace they set. “My older daughter is interested in the topic,” Hebb says, “but my younger daughter has zero interest and I feel bad for her that her father is the death guy, so I don’t force it on her. But if a child is interested in, curious about, scared of or ruminating on death, it is of great benefit to meet them in their curiosity or concern or fear. It’s also a great way to know your child better.”
8. … And be there for bereaved parents
“We are often afraid to bring up death in the presence of parents who have lost children,” says Hebb. “It’s an unimaginable amount of grief for lots of us. But if we want to stay connected to those people, it’s imperative we engage with them because it is certainly in their thoughts and dreams all the time.” He says many people also lose friends when they lose children because those friends are too frightened to discuss the subject and the relationship breaks down.
9. God makes little difference
You would think belief in an afterlife would make the pain of dying less, but Hebb is sceptical. “Faith plays a role, but it isn’t as central as you would think. Grief will exist regardless of whether or not people have faith. If that’s an excuse not to have the conversation, you’re not doing yourself any favours.”
10. Accept that caring for the dying is hard
People who are dying fret about being a burden on their friends and family, while carers feel they have to be perfect and never show frustration or exhaustion. Hebb says both should be honest about any resentment they feel. “Care-givers should feel they have permission to have all these conflicting emotions,” he says. “If the person thinks they are the only one who feels this way, that’s much more traumatic than realising that it’s OK to resent the person you’re taking care of. ”
11. Death is not a medical act
Like others who have written about death, notably Atul Gawande in his book Being Mortal, Hebb emphasises that death is a human and community event, not a medical event. “Medicine is what keeps you alive and that’s what doctors are focused on,” Hebb says. “We have to reclaim the death part. Don’t leave it in the hands of tacticians.” He praises a project at the Cleveland Clinic called “The Pause” where the medical team gather round the bedside of a person who has just died to have a moment of silence and then share their recollections of the patient. It is not merely a medical failure to be recorded and a body to be disposed of; it is a life and a person to be honoured.
12. There are no rules for grieving
Finally, Hebb says, it is impossible to systematise grief. “Every case, every person, every situation is different. We should give ourselves permission to grieve in precisely the way we need to.” If you beat yourself up for the way you are grieving, you will only lengthen and deepen your grief.






 Through its painstakingly created and very human VR experiences, the company has cornered the market on a type of next-generation training tool. It provides an experience that caregivers or clinicians cannot get simply by reading textbooks.
Through its painstakingly created and very human VR experiences, the company has cornered the market on a type of next-generation training tool. It provides an experience that caregivers or clinicians cannot get simply by reading textbooks. Of course, there are problematic aspects with the idea of building empathy through VR. A 30-minute simulation about end-of-life conversations is not the same thing as experiencing it for real. A person really experiencing the effects of homelessness or discriminatory activity cannot simply take off their headset when they decide they’ve had enough of their life circumstances. Attempts to “gamify” complex scenarios risk inadvertently diminishing them, and carry the chance of turning something intended for good into something exploitative.
Of course, there are problematic aspects with the idea of building empathy through VR. A 30-minute simulation about end-of-life conversations is not the same thing as experiencing it for real. A person really experiencing the effects of homelessness or discriminatory activity cannot simply take off their headset when they decide they’ve had enough of their life circumstances. Attempts to “gamify” complex scenarios risk inadvertently diminishing them, and carry the chance of turning something intended for good into something exploitative.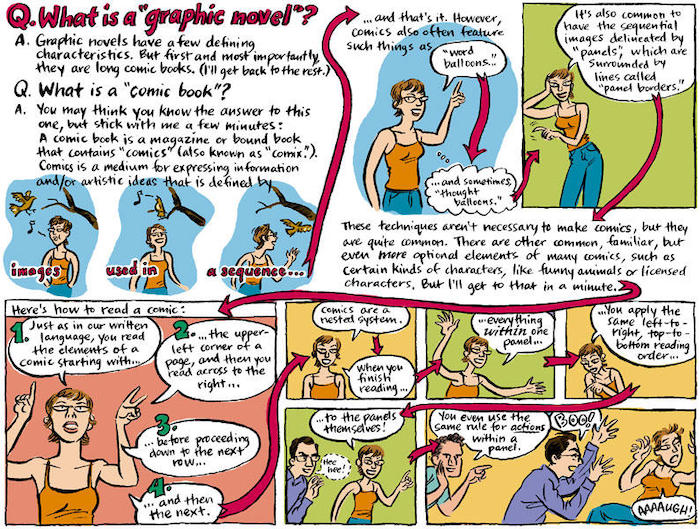


 Gilbert reflects on the death of her partner, Rayya Elias — her longtime best friend, whose sudden terminal cancer diagnosis unlatched a trapdoor, as Gilbert put it, into the realization that Rayya was the love of her life:
Gilbert reflects on the death of her partner, Rayya Elias — her longtime best friend, whose sudden terminal cancer diagnosis unlatched a trapdoor, as Gilbert put it, into the realization that Rayya was the love of her life:

