by InspireMore Staff
There is nothing more painful than the death of a loved one. Aside from sadness that comes with the loss, there’s also the task managing that comes with sudden tragedies. Calling the family, talking to the police if necessary, and– yes– posting on Facebook.
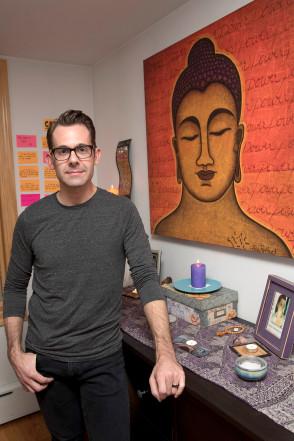
As silly as that last point may sound, it’s become a very real part of the grieving process in this social media age. So much so that, a woman named Taya Dunn Johnson, wrote the following open letter after her husband’s death, titled “Please read this before you post another RIP on social media.”
It’s a powerful reminder to put people first– to honor what Taya calls “the hierarchy of grief”– even in our social media obsessed world.
Grieving in the technology age is uncharted territory.
I’ll take you back to Saturday, June 9, 2012. At 8:20 a.m., my 36-year-old husband was pronounced dead at a hospital just outside Washington, D.C.
By 9:20 a.m., my cellphone would not stop ringing or text-alerting me long enough for me to make the necessary calls that I needed to make: people like immediate family, primary-care doctors to discuss death certificates and autopsies, funeral homes to discuss picking him up, and so on. Real things, important things, time-sensitive, urgent things.
At 9:47 a.m., while speaking to a police officer (because yes, when your spouse dies, you must be questioned by the police immediately), one call did make it through. I didn’t recognize the number. But in those moments, I knew I should break my normal rule and answer all calls. “He’s dead??? Oh my God. Who’s with you? Are you OK? Why am I reading this on Facebook? Taya, what the heck is going on?”
Facebook? I was confused. I hadn’t been on Facebook since the day before, so I certainly hadn’t taken the time in the last 90 minutes to peek at the site.
“I’ll call you back”, I screamed and hung up. I called my best friend and asked her to search for anything someone might have written and to contact them immediately and demand they delete it. I still hadn’t spoken to his best friend, or his godsister, or our godchild’s parents, or a million other people!
Why would someone post it to Facebook SO FAST?
While I can in no way speak for the entire planet, I certainly feel qualified to propose some suggestions — or, dare I say, rules — for social media grieving.
How many RIPs have you seen floating through your social media stream over the last month? Probably a few. Death is a fate that we will each meet at some point. The Information Age has changed the ways in which we live and communicate daily, yet there are still large voids in universally accepted norms.
This next statement is something that is impossible to understand unless you’ve been through it:
There is a hierarchy of grief.
Yes, a hierarchy. It’s something people either don’t understand or understand but don’t want to think or talk about — yet we must.
There is a hierarchy of grief.
Hierarchy is defined as:
1. a system or organization in which people or groups are ranked one above the other according to status or authority, and
2. an arrangement or classification of things according to relative importance or inclusiveness.
What does this mean as it relates to grief? Let me explain. When someone dies — whether suddenly or after a prolonged illness, via natural causes or an unnatural fate, a young person in their prime or an elderly person with more memories behind them than ahead — there is one universal truth : The ripples of people who are affected is vast and, at times, largely unknown to all other parties.
A death is always a gut punch with varying degrees of force and a reminder of our own mortality. Most people are moved to express their love for the deceased by showing their support to the family and friends left behind.
In the days before social media, these expressions came in the form of phone calls, voicemail messages, and floral deliveries.
If you were lucky enough to be in close proximity to the family of the newly deceased, there were visits that came wrapped with hugs and tears, and deliveries of food and beverages to feed all the weary souls.
Insert social media. All of those courtesies still occur, but there is a new layer of grief expression — the online tribute in the form of Facebook posts, Instagram photo collages, and short tweets.
What’s the problem with that? Shouldn’t people be allowed to express their love, care, concern, support, and prayers for the soul of the recently deceased and for their family?
Yes.
And no.
Why? Because there are no established “rules,” and people have adopted their own. This isn’t breaking news, and you’re not trying to scoop TMZ. Listen, I know you’re hurt. Guess what? Me too. I know you’re shocked. Guess what? Me too. Your social media is an extension of who you are. I get it. You “need” to express your pain, acknowledge your relationship with the deceased, and pray for the family.
Yes.
However…
Please give us a minute.
We are shocked.
We are heartbroken.
Give the immediate family or circle a little time to handle the immediate and time-sensitive “business” related to death. In the minutes and early hours after someone passes away, social media is most likely the last thing on their minds. And even if it does cross their mind, my earlier statement comes into play here.
There is a hierarchy of grief.
Please pause and consider your role and relationship to the newly deceased. Remember, hierarchy refers to your status and your relative importance to the deceased. I caution you to wait and then wait a little longer before posting anything. This may seem trivial, silly, and not worth talking about, but I promise you it isn’t.
If the person is married, let the spouse post first.
If the person is “young” and single, let the partner, parents, or siblings post first.
If the person is “old” and single, let the children post first.
If you can’t identify the family/inner circle of the person, you probably shouldn’t be posting at all.
Do you get where I’m going with this?
In theory, we should never compare grief levels, cast the grief-stricken survivors into roles, or use words like status and importance. But maybe we need to at this moment (and for the next few weeks and months).
The “RIP” posts started hitting my timeline about an hour after my husband’s death, and I certainly didn’t start them. This created a sense of confusion, fear, anxiety, panic, dread, and shock for the people who knew me, too. What’s wrong? Who are we praying for? Did something happen? Did someone pass? Why are there RIPs on your wall and I can’t reach you? Call me please! What’s going on?
That’s a small sample of messages on my voicemail and text inbox. I had to take a minute in the midst of it all to ask a friend to post a status to my Facebook page on my behalf.
Your love and expressions of support are appreciated and needed, but they can also be ill-timed and create unintended additional stress.
The person is no less dead and your sympathy no less heartfelt if your post, photo, or tweet is delayed by a few hours. Honestly, the first couple of hours are shocking, and many things are a blur. Most bereaved people will be able to truly appreciate your love, concern, prayers, and gestures after the first 24 hours.
I’ve learned this from the inside — twice within the last four years. And I assure you that if we each adopted a little patience and restraint in this area, we would help those who are in the darkest hours of their lives by not adding an unnecessary layer of stress.
A few extra hours could make all the difference.
Complete Article ↪HERE↩!