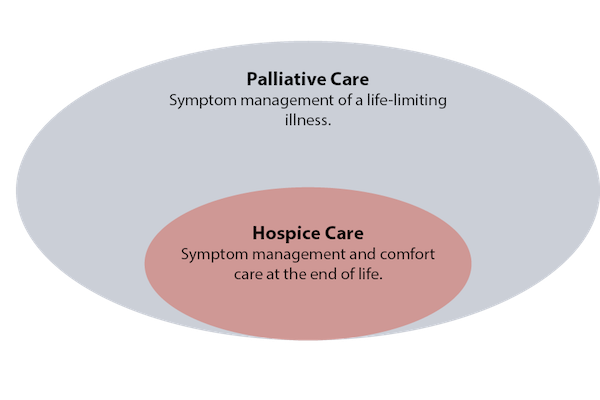
Hospice a word that is synonymous with “end of life” care. Palliative – a little more confusing and often confused with ‘end of life’. The two are very different therapies but Palliative Care is an offshoot of Hospice.
Hospice is a service for patients who are terminally ill and have decided not to take any more medication that might “cure” them (i.e. chemotherapy for a cancer patient). The focus becomes relief from pain and symptoms and not a cure. There are some who say that going into Hospice means you’re giving up or that you will no longer receive the medical care you need. That is not true – you have chosen to focus on your quality of life not the quantity and the medication used is to do just that.
A Hospice team usually includes a doctor, nurse, social worker and chaplain (if you wish). They work together to meet the patients physical, emotional and spiritual needs. This team also cares for the family who can be against the choice to, in their eyes, “give up.” There is counseling, hugs and support from a good Hospice team – my Mother’s team was unbelievable and supported and counseled our entire family through the last three days of her life.
To qualify for Hospice your doctor must state that the patient’s death is expected in 6 months or less. If a patient chooses Hospice then changes his or her mind it isn’t an issue. The patient simply goes back into the curative therapy with their doctor. You can also change your mind again and be readmitted . . . there is no pressure – it’s about what you, the patient want.
Palliative Care (pronounced pal-lee-uh-tiv) is specialized medical care for people with serious illness. This type of care is focused on providing relief from the pain, symptoms and stress of a serious illness for both the patient and family.
Again, it’s a team of specially-trained doctors, nurses and other specialists who work in partnership with the patient’s other doctors to provide an extra layer of support. It can be used at any age and at any stage in a serious illness. The services are offered in tandem with the curative treatment. A good example of Palliative Care use is in Parkinsons or Multiple Sclerosis when there are flare ups.
Both Hospice and Palliative Care are paid for by most insurance companies including Medicare and Medicaid. Both are offered in your home, nursing homes, assisted living centers, hospitals and provide respite care when the caretaker family needs a break.
What these two services offer us are choices in treatment for serious illnesses. We each have our own journey and whilst none of us hope it comes to either of these services, we can make informed decisions for us or our loved ones knowing that they exist. No matter how strong you are physically and emotionally – watching a loved one suffer is often intolerable. There are teams out there to support and comfort. Use them if you need them.
Many of us are so used to living in the past or the future that we have no awareness of what being in the present means. Recent research has shown that we are not as conscious as we think we are. In fact, we are unconscious most of the time as we move about our day, with […]
Many of us are so used to living in the past or the future that we have no awareness of what being in the present means. Recent research has shown that we are not as conscious as we think we are. In fact, we are unconscious most of the time as we move about our day, with only specific decisions making their way into our consciousness. Because of this, we struggle to live in the present because our mind swings from thought to thought, only briefly settling somewhere that captures our truest form of attention. To become more mindful and present in your life, focus on these three areas.
Unselfconsciousness
Thinking about yourself and how you appear to others takes you out of the moment. When in a situation you already feel anxious about, focusing on the anxious feeling worsens it. Instead of focusing on what’s going on in your head, think instead of what’s happening around you and how you are a part of that. Mindfulness blurs the line that exists between yourself and others. Without feelings of self-consciousness, you’re able to witness the passing of feelings and perception of being evaluated by others without feeling threatened and taking it personally.
Savoring
Being so caught up in our thoughts prevents us from truly experiencing and enjoying our own lives. Instead of appreciating what we’re experiencing, we think of when the next time we’ll get to experience this again is or how the experience could be better. Learning how to direct your attention allows you to become an expert at savoring the present moment. No matter what the moment is, take note of how you’re feeling in all of your senses. Taking a few extra minutes to savor daily activities helps you to feel more joy and happiness and fewer depressive symptoms. Savor the taste of food, rather than gulping it down. Savor the feeling of fresh air as you walk to your car rather than re-playing what happened in your meeting. Savor the smell of your favorite cologne, perfume or lotion to bring yourself into the moment. Because the majority of negative thoughts involve the past or future, thinking in the present forces you to stop ruminating on the past and stop catastrophizing about the future.
Acceptance
When faced with pain or discomfort, our natural reaction is to avoid it. Resisting unpleasant feelings and thoughts means you don’t have to face them. Humans have two types of emotions: primary and secondary. Secondary emotions are ones that we feel around other feelings. When we feel stressed out about being busy at work, the primary emotion is the stress surrounding your workload. The secondary emotion is hating feeling stressed. Instead of fighting these emotions, allow yourself to take them in. Be open to how you feel in the present moment without judging your feelings or trying to push them away. Focusing on your secondary emotions instead of feeling your primary ones actually prolongs the negative feelings. Accepting these emotions doesn’t mean you like them and want to feel this way forever. It instead means that there are some things you can’t change, and how you feel right now is one of those things. Accepting your feelings doesn’t mean resigning to them.
Applying these three techniques will help you develop PRESENCE. When you are able to bring your presence to each situation in your life, be it at work, in your relationship, or even when hanging out with friends, the quality of your life experience will increase dramatically.
Fifty years ago, a physician was admitted to the hospital with stomach cancer. He wrote down in his own medical chart that he did not want CPR or to be connected to a breathing machine. His wishes were disregarded — he underwent CPR numerous times and was connected to a breathing machine until he died. Back then, not only were people treated in ways they did not want, many patients were also arbitrarily denied potentially lifesaving therapies.
Doctors decided who deserved to live or not: In one New York hospital, doctors put purple stickers on the charts of patients they determined would not receive CPR or other similar measures without the patients’ or their families’ knowledge. Decisions about life and death were subjective and opaque.
End of life care has considerably improved since then. Patient preferences now help direct physicians and nurses about what type of care they would want to receive. But 50 years into the future, we will look back on today and conclude that medicine was sorely lacking when it came to how we handle death.
Many in medicine, as well as patients and caregivers, continue to equate more procedures, more chemotherapy, and more intensive care with better care. Studies in patients with cancer and heart disease, the two greatest killers of mankind, show that patients receiving palliative care, which is an approach that focuses on quality rather than quantity of life, can actually live longer. While the goal of palliative care is to help people with a serious illness live as well as possible — physically, emotionally and spiritually — rather than as long as possible, some people receiving palliative care might also live longer since they avoid the complications associated with procedures, medications, and hospitalization
In addition, while medical advances have moved forward at blinding pace, the ethical discourse surrounding many technologies has not kept up. Take, for example, cardiac devices such as pacemakers and mechanical pumps that can be placed in the heart. Many patients with terminal illnesses who want to deactivate these devices find resistance from the health system, since some continue to equate deactivating them with euthanasia. We need to continue to make sure that even as technological advances blossom, patients remain at the center, and physicians continue to honor their wishes.
And while the palliative care specialty has greatly improved end-of-life care, too often, palliative care has been used as a way to avoid the culture change needed by all medical specialties to better handle death. Despite its many benefits, many patients and physicians are scared of “palliative care” because of its strong association with the end of life. Some have been compelled to change the title of their practices to “supportive care.” To many patients, the very name “palliative” implies that they will be abandoned, making them very reluctant to accept their services. The fact is that palliative care can, and should, be delivered to patients with serious illness alongside conventional care.
But the issues go beyond the name — one recent study showed that palliative care-led meetings with families of patients in intensive care units led to an increase in post-traumatic stress disorder symptoms among family members. Palliative care specialists are often consulted in tense situations when patients are critically ill, and they often have no prior relationship with patients or their families, who might be unprepared to have serious discussions with them. That’s why most of these difficult conversations should be delivered by the doctors and surgeons primarily responsible for treating the patients. One study estimated that by 2030, the ratio between palliative care specialists and eligible patients will be 1 to 26,000. Palliative care specialists cannot be entirely responsible for end-of-life care by themselves.
To emerge on the right side of history, the entire culture of medicine needs to be turned around. End-of-life care is not just palliative care’s business. It is everyone’s business, from emergency room doctors to primary care physicians. Physicians need to abandon outdated ideas that their role as healers is incompatible with helping patients die comfortably and on their own terms. Helping patients die well is as important as helping them live to the fullest.
In this Feb. 4, 2019 photo, Donald Granstaff, 92, sings Louis Armstrong’s “On the Sunny Side of the Street” at his Princeton, Ky., home with board certified music therapist Kenna Hudgins, a contractor with Pennyroyal Hospice. Hudgins designs Donald’s weekly music therapy sessions to help decrease any feelings of isolation.
By MICHELE VOWELL
“At 92 years old, I finally learned to do as I’m told,
The sun comes up, the sun goes down,
The earth keeps goin’ ’round and ’round.
I’m content where I am.
In the winter of life, I do the best that I can.”
Princeton resident Donald Granstaff spends much of his time these days looking back on his life.
The 92-year-old husband, father, Navy veteran, musician, preacher and missionary served his country and God for decades around the globe. Today, Donald often reflects on those times from his bedroom while under the care of Pennyroyal Hospice.
“I was thinking the last few days, what have I accomplished?” he said Monday afternoon. “Around the world twice. Haiti and the West Indies — all that. And all I can come up with is the guys that I prayed with and I lead them to the Lord. And, I suppose that’s what it’s all about.”
To help Donald face the winter of his life, Kenna Hudgins, board certified music therapist, brings her keyboard, drums, guitar and even a tambourine, weekly to share an hour of tunes with the elderly patient at his home. Hudgins and Donald sing familiar songs and play the instruments together in an effort to make his transition easier.
“The main goal I initially assessed (for Donald) was for anticipatory grief — to work through the acceptance of the fact that we are terminal and now on hospice (care),” she said. “He’s very aware, so day after day just knowing that it’s coming and there will be changes and decline. Life is hard. Music therapy offers a way to process that musically.”
Music therapy
“Anyone who responds to music can benefit from music therapy, especially in hospice,” Hudgins said. “Music plays a role in all of our lives. It always has. It’s why we can watch a movie and feel scared, feel love or feel emotion. Music causes neurologic response — it affects our whole brain — in multiple areas simultaneously. Because of that, music therapy is not about being a musician. It’s not about understanding music. It’s about just responding.”
Hudgins, who is a contractor with Pennyroyal Hospice, uses her skills as a board certified music therapist to address the needs of patients in Christian, Todd, Trigg, Lyon and Caldwell counties in western Kentucky.
“Hospice is very grounding,” Hudgins said. “Every day that you go into somebody’s house and they’re dealing with their struggles, it brings you back to true purposes — day-to-day tasks and stresses don’t matter as much because life is short. Personally, it’s just a very rewarding field.”
Communicating with hospice social workers, Hudgins identifies patients who may benefit from music therapy. She asks family members for 10 minutes of their time to visit their loved one and share a song or two with them to assess his or her responses.
“I don’t usually talk much about it, I just let them experience it,” she said, smiling. “I’ve never been told not to come back and it’s never just 10 minutes.”
Hudgins said everyone has memories associated with certain music.
“A therapist’s job is to find that music that is significant to that person,” she said.
Working with some patients can be difficult, Hudgins said, because of the emotions tied to facing the end of life, but sharing music with them is rewarding.
“Music is so joyful,” she said. “When I get to bring joy to a family and a loved one … that’s not a sad job. … I’m really blessed to just be a part of their lives. To bring joy is just huge.”
Music with Donald
After working with Donald for several weeks, Hudgins said her therapy goals for him shifted to decreasing his feelings of isolation.
“I try to get as much participation from him physically, whether that’s playing the keyboard or drumming,” she said. “As his hands might get more stiff, clapping — anything to get his body engaged. If his body is unable, then just getting him to verbally participate. That, in and of itself, will decrease isolation.”
In Monday’s music therapy session, Hudgins wanted Donald to sing some love songs with her while playing instruments.
“With Valentine’s day coming up next week, we’re going to do sweetheart songs,” she said.
“The old sweetheart songs,” Donald said. “That’s the best kind, the old ones.”
The duo harmonized to Bing Crosby’s “Let Me Call You Sweetheart” as Hudgins played the keyboard.
“Let me call you sweetheart
I’m in love with you
Let me hear you whisper
That you love me too …”
In the middle of the song, Don stopped singing to share a childhood memory.
“I used to hear my dad sing that one all the time,” Donald said.
“Yeah? Did he sing it to your mom?” Hudgins said.
“Yeah. He worked in vaudeville for a long time,” he said. “He played mandolin and violin, and he sang all the time. He loved to sing.”
“Good memories,” Hudgins said.
Donald married his own sweetheart Betty 68 years ago. They exchanged vows on June 16, 1950.
“It was my birthday,” he said.
In the living room, Betty sat on the couch quietly listening to her husband sing and play music with Hudgins. She said music therapy is a comfort to her and Donald, who played several instruments, including the organ, keyboard and drums since he was a boy.
“I love that he’s even trying,” she said after the session. “I think this is a good thing for him because he was a musician. It meant so much to his heart. That was his life.”
Back in his bedroom, a second song, Frank Sinatra’s “My Funny Valentine,” also sparked Donald’s memories of his father.
“That’s a good song,” he said. “He used to sing songs like it.”
“I’m glad I’m making you think about your dad. I haven’t heard you talk a lot about him,” Hudgins said.
“He was quite a man. Yeah boy! He was something else,” Donald said, remembering times they would go fishing together at Lake Barkley. “He owned a couple of boats. Nice, big boats. And I used to go with him on the boats.”
Midway through the hour, Hudgins sang the chorus to a song about Donald’s life they wrote together after three or four music therapy sessions.
“I am a husband, a father, a preacher, a teacher
A born-again, saved-by-grace man …”
“When I came out of college, I was a really smooth character,” Donald said, listening to the lyrics. “I was fast and furious, and I didn’t stay that way very long. I was saved in June 1959, and before that I was a ‘religious’ human being …”
Early in their marriage, Donald and Betty took their five children to the mission field in the British Isles of the Caribbean and later in Haiti. Donald also helped another missionary build a radio station in Dominica. When they moved back to the U.S., he pastored a few churches in McMinnville, Tennessee, and Princeton. For a time, he often played the organ in the Barkley Lodge dining room.
“He was a musician from the time he was little,” Betty said. “Every church we were a part of he would play the organ until he wasn’t able to physically.”
Now, Betty said, some days can be difficult.
“Sometimes I have an overwhelming sadness. It’s hard to see him not be able to do anything,” Betty said, crying. “God love him, he never complains. Never, ever complains about anything. He’s just always up and very sweet. He’s still a testimony to everybody that visits him because of his attitude.”
Happy Trails
To close out Monday’s music therapy session, Donald and Hudgins sang the Roy Rogers and Dale Evans classic, “Happy Trails.”
“Who cares about the clouds when we’re together?
Just sing a song, and bring the sunny weather.
Happy trails to you,
Until we meet again.”
“I think it’s good. It can help lift you up,” Donald said of music therapy with Hudgins. “I’m not like some guys. Some guys get tired of it, throw their hands up and leave. I’ll try.”
Hudgins said Donald “still has a lot of life in him.”
“Whether (the patient) is a musician or not, music is a way to connect with the outside world. It can pull you into different areas of your own life, make you feel alive again,” she said.
Part of Donald’s legacy will be the song he and Hudgins wrote together.
“We have created a tangible song that he can leave for his family,” she said. “His family are musicians so they can actually play that song and play it with him.”
The chorus is:
“I am a husband, a father, a teacher, a preacher
A born-again, saved-by-grace man.
I’m a musician, woodworker, a servant, missionary
But most of all I’m just a good ole boy from Kentucky.”
Donald and Hudgins plan to meet next week for music therapy.
“Every one of us has had music in our lives that has impacted us,” Hudgins said. “It’s my job to figure out what is going to impact someone at the end of their life for the best end-of-life experience possible.”
Dr. Susan Wong sat down with an 84-year-old patient in the hospital, where he’d been admitted with a flare-up of a serious autoimmune condition and deteriorating kidney function.
The older man told her he wanted to go home; he’d had a good life and was ready for its end. He didn’t want aggressive care — including dialysis — having witnessed his wife and son die painfully in intensive care years ago.
Wong, an assistant professor of nephrology at the University of Washington, was prepared to follow the man’s wishes, but other physicians, eager to pursue tests and treatments, disagreed. For a week, the doctors argued about what to do. Finally, they discharged the patient, who died in hospice care a few weeks later.
Older adults with advanced kidney disease who want to forgo dialysis often encounter similar resistance from physicians, according to a new study in JAMA Internal Medicine by Wong and colleagues at the Veterans Affairs Puget Sound Health Care System in Seattle, where she’s an investigator.
The researchers documented doctors’ reactions by reviewing medical charts of 851 older patients with chronic kidney disease who refused dialysis at the VA health system from 2000 to 2011. In their notes, physicians frequently speculated the patients were incompetent, depressed, suicidal or irrational.
With dialysis, people are hooked up to a machine that removes waste from their blood, usually three times a week for four hours at a stretch. Many older adults find the treatments burdensome, and medical complications are common.
Yet patients who expressed reservations about this treatment were sometimes labeled as difficult or unprepared to confront the reality of their medical condition. “Still in denial about his kidney disease and his need for hemodialysis in the near future — repeat discussions with patient and wife regarding compliance,” one nephrologist wrote. Even when patients were firm about declining dialysis, doctors repeatedly questioned their decisions.
“Clinical practice guidelines for advanced kidney disease are geared toward survival, not what would give patients the best quality of life or the greatest functional capacity,” Wong said. Another factor at play: Nephrologists aren’t trained to ask seriously ill patients what’s most important to them and shape treatment recommendations accordingly. Although most patients want to have such conversations with a kidney specialist, few do so, studies have found.
“We don’t really know how to help patients with serious illness make decisions that are right for them or what to do when they don’t really want dialysis,” said Dr. Jane Schell, an assistant professor of palliative care and nephrology at the University of Pittsburgh.
Conversations about the potential benefits and burdens of dialysis, as well as alternatives, are especially important for frail patients 75 and older who have two or more chronic conditions, such as diabetes and high blood pressure, and difficulty with daily activities such as bathing or walking — a group at risk of experiencing significant complications from dialysis but not achieving longer life.
Healthier older adults have better outcomes on dialysis — a valuable treatment for many people. “We shouldn’t limit access to dialysis based on age, but we should have meaningful conversations about goals of care and make it clear that dialysis is a choice and that patients have alternatives,” said Dr. Bjorg Thorsteinsdottir, an assistant professor of internal medicine and bioethics at the Mayo Clinic.
Options that should be discussed include comprehensive conservative care, which calls for preserving as much kidney function as possible, managing a patient’s health problems, dealing with symptoms such as nausea, swelling, itchiness, pain and breathing difficulties, and preparing for end-of-life care; peritoneal dialysis or hemodialysis at home; and palliative dialysis, a less intensive version of this treatment that keeps people alive for longer but isn’t meant to restore kidney function.
Comprehensive conservative care programs are few and far between (in New York City, Pittsburgh, Seattle, San Francisco and a few other locations), but efforts are underway to change that. With funding from the American Society of Nephrology, Schell and colleagues at the University of Pittsburgh have developed an online conservative care curriculum set to debut in March. Nineteen nephrology training programs for physicians are set to participate.
Also, the Pathways Project, funded by the Gordon and Betty Moore Foundation, is working to make palliative care (also known as supportive care) for patients with advanced kidney disease widely available. (KHN’s coverage of end-of-life and serious illness issues is also supported in part by the Gordon and Betty Moore Foundation.) Dr. Alvin Moss, co-investigator of the project and professor of medicine at West Virginia University School of Medicine, said the project hopes to sign up 10-15 dialysis centers this year.
Sometimes, patients choose a time-limited trial of dialysis with the understanding that they can change their minds down the road.
Cyndy Patton’s 86-year-old mother, Isabel, learned last spring she had advanced kidney disease after going to a Pittsburgh hospital, sickened by repeated bouts of vomiting. Physicians suggested she try dialysis for a few weeks and see if her kidneys might rejuvenate. (The older woman had survived open-heart surgery and a stroke and was living on her own after her husband’s death.)
After a week in the hospital and another week in a rehabilitation center, there was no change: Patton’s mother still needed dialysis. Five weeks later, she confessed to her daughter that the treatment was making her miserable. But giving it up felt like committing suicide, she told Patton — an unacceptable option.
A week later, Isabel had changed her mind. “This is not a life I care to lead, being hooked up to these machines,” she told Patton. “What am I doing this for?” The older woman had consulted with Schell at the University of Pittsburgh about palliative care and hospice care, and she chose hospice.
Dialysis ended and the family gathered at Isabel’s bedside. “She was all ready to die — but she didn’t, and is still living to this day,” Patton said.
It’s an example of how hard it can be to predict what will happen to any given patient with advanced kidney disease. What’s important for the patient to understand is that “it’s not always all or nothing — dialysis or death,” Thorsteinsdottir said.
Meaghan Jackson has a surprising amount of insight into death and love for a 36-year-old.
“Working here, it’s changed me,” Jackson said from a wood-panelled room at the North Shore Hospice, where she has worked as a music therapist for four years.
“It’s completely changed the trajectory of my life.”
Meaghan Jackson is a music therapist at the North Shore Hospice. Jackson says working in palliative care has changed her life.
Jackson guides the residents at the hospice through their final days. She helps them write songs for their loved ones, and plays music for them as they take their last breaths.
Jackson has worked in “death and dying” since she was 22. She says her experiences prompted her to have children early in life, and focus on the present, no matter how difficult.
“I practice the art of being present when that present isn’t pleasant,” she said.
Health practitioners like Jackson say their experiences working with dying patients offer insights into love, relationships and how to focus on what matters.
A room at the B.C. Cancer Centre in Vancouver. Health practitioners say patients facing death tend to prioritize their relationships.
Each of the four practitioners interviewed for this story — a doctor, a social worker, a nurse and a music therapist — say dying patients tend to focus their energy and attention on the people they love.
Dr. Pippa Hawley, a palliative care doctor at the B.C. Cancer Centre, says she has seen couples and families reconcile after decades apart. She’s also seen several of her dying patients get married in the palliative care unit, sometimes in their beds.
Hawley says dying patients don’t have time to take loved ones for granted.
“All of that stuff that we bother with on a day-to-day basis just fades into irrelevancy,” she says.
Dying patients face many challenges with their partners, even when they prioritize love.
Melanie McDonald, a social worker who also works in palliative care at the B.C. Cancer Centre, says every couple she helps deals with death differently.
Couples who thrive during difficult moments are often those who can balance sadness with joy and love, she says.
Social worker Melanie McDonald says couples face many challenges when faced with death.
Nurse Jane Webley, who leads Vancouver Coastal Health’s palliative care unit, says the strongest couples are best at honestly communicating their needs, feelings and end-of-life plans.
Webley says patients who find it too difficult to discuss those matters are often the same ones who push loved ones away and face death alone.
“I think that’s a protection mechanism,” she said. “I would say 90 per cent of the time, it’s fear — and that fear is brought about by lack of communication.”
Dr. Hawley says some of her patients are never able to communicate their feelings and needs. Often, she says, that’s been a long-standing issue for them.
“People tend to die as they have lived,” she said.
Talking about death and end-of-life plans is often easier for older couples who are often more in touch with mortality. But Webley says it’s never too soon to have those difficult conversations.
Another challenge couples face when one is dying is learning to give or receive help, health practitioners say.
Social worker McDonald says people who aren’t used to being caregivers, typically men, often struggle when they’re suddenly thrust into that position. But most people learn to take on that role, she says.
Health practitioners say that learning to ask for help can be a steep learning curve for some patients.
Dr. Hawley says patients can face problems as they lose their independence. But she says it’s important for people to let their partners care for them.
“Don’t feel like you’re a burden,” she said. “It’s actually a wonderful gift to be allowed to care for somebody, to show them that you love them.”
All four of the health care practitioners say love at the end of life can take many shapes.
“Love looks differently in different situations,” says social worker McDonald. “Love shows up in the end of life in friendship and in families and pets and faith traditions and all sorts of different ways.”
Humans are sexual beings. This urge does not stop when the clock strikes 60. Or even 90.
Young adults may deny older relatives are having sex, but sexual activity is a strong indicator of healthy aging and vitality. In fact, sexual activity is roughly equal to climbing two flights of stairs.
Sex education and research use a medical model of sexual health focusing mainly on pregnancy, sexually transmitted infections (STIs), and sexual dysfunctions. However, sexuality is complex. Beyond genitals and Kama Sutra-like positions, it considers sexual and gender identity; sensuality; sexual response; intimacy; and positive and negative ways we use our sexuality.
As we age, the complex interplay among biological, psychological, cognitive, socioeconomic, religious and even societal factors, contribute to changes in our roles and responsibilities. For example, changes in physical or cognitive health over time can create differences in analytical thinking, mobility, and health care needs. We also experience changes in work, social and family roles and responsibilities over time. Examples include transitions from working to retirement, parenting to empty-nesting, child-rearing to caring for aging parents or partners.
These changes may alter our sexual desires, expression and the frequency in which we engage in sexual activities with partners. For example, sexual functioning and activity may decrease over time, but having open communication with a partner who is responsive to our needs can increase our feelings of intimacy and desire, and in turn stimulate sexual activity.
Evolving social support and activities may change opportunities for sex and intimacy. Partners may disappear through death or moving away, or appear, such as when meeting new people after moving to an aging community. Over one-third of adults over age 65 use social media or internet technologies. These tools may expand sexual interest or activities by increasing access to sexual aids and partners.
Sex after 60
There are myths, misconceptions and stigma associated with aging and sexuality that hinder older adults’ ability to openly communicate with family, friends and health care professionals. This misinformation limits their access to sexual education, health care, and ultimately, their sexual rights.
The first myth is that older adults are not as sexually attractive or desirable as their younger counterparts. While an 80-year-old may not be as appealing to an 18-year-old, he or she may be very desirable to peers. More importantly, he or she may feel more sexually desirable and confident than their younger self.
A second myth is that older adults lack interest in and desire for sexual activity—and that they are somehow asexual. Research from ongoing national surveys support the ideas that sexual interest, desires and behaviors can decrease over the life course. For example, among women ages 57 years and older, over 80 percent of participants expressed interest in having sex, but less than two-thirds of women surveyed perceived sex as “important,” and fewer than half reported having sex in the previous year. However, the reality is that these trends are not universal among older adults. Results from another recent survey found that 39 percent of men and 17 percent of women ages 75 to 85 years are sexually active.
Another myth is that older adults are so medically fragile that sexual activity is dangerous. This is simply not true in many cases. Recent studies have shown that healthy older adults are more likely to have sex. Even when chronic illnesses are present, sexual abstinence is not a foregone conclusion. For example, a 2012 American Heart Association statement contains evidence-based recommendations about sexual activity among patients with specific cardiovascular conditions. The recommendations generally advise assessing risks with a doctor and disease management, rather than abstention.
There are well-documented relationships between common medical conditions such as heart disease or diabetes and treatment-related effects on sexual functioning. Yet, older adults and their health care providers are not discussing sexual concerns during routine care. Missed opportunities during visits deprive older adults of access to newer treatments and other best practices in sexual medicine, which can impact their mental and physical health.
A bigger problem may be ageist attitudes among providers and internalized ageism in their patients that may interfere with sex education and application of newer standards. The result is that many believe older adults are uninterested in, or lack desire for, sexual activity and cannot engage in these activities.
Love has a lot to do with it
There is more to sexuality than physical acts. While much of the existing research focuses on sexual activity and intercourse as predictors or outcomes, most older adults also desire companionship, intimacy and closeness. Non-intercourse-focused activities, such as hand-holding, cuddling and massage, have not been studied as much as intercourse. Yet, there is reason to believe that they can enhance intimacy. Research about physical and mental health outcomes resulting from older adult sexual activity reveals additional benefits, including reduced cognitive decline, loneliness and depression, and improved reported health status, physical functioning, and other aspects of quality of life.
Recent studies also reveal that sexually active older adults are more likely to communicate needs and concerns with health care providers and have them addressed. Providing high-quality sexual health care requires providers to take comprehensive sexual health histories from older patients and engage in direct, positive communication concerning gender and sexual identity, and sexual knowledge, beliefs and practices.
Discussions should promote understanding about sexual risk behaviors for STIs and effects of physical and cognitive or psychological aging on sexual health and sexuality. To maintain or improve older adults’ sexual health and well-being, health care providers should provide safe and welcoming environments for patient-provider collaboration, resources and interdisciplinary referrals to clinical social workers, sex therapists, physical therapists and other allied health specialties.