— An interview with Michele DiTomas and Keith Knauf
In the early 1990’s, California Medical Facility (CMF) created one of the nation’s first licensed hospice units inside a prison. This 17-bed unit serves inmates from all over the state who are approaching the end of their lives. A few are let out early on compassionate release. Many are there until they die.
Today’s podcast is part one of a two-part podcast where we spend a day at CMF, a medium security prison located about halfway between San Francisco and Sacramento, and the hospice unit housed inside its walls.
We start off part one by interviewing Michele DiTomas, who has been the longstanding Medical Director of the Hospice unit and currently is also the Chief Medical Executive for the Palliative care Initiative with the California Correctional Healthcare Services. We talk about the history of the hospice unit, including how it was initially set up to care for young men dying of AIDS, but now cares for a very different demographic – the rapidly aging prison population. We also talk about the eligibility for the unit, what makes it run including the interdisciplinary team and the inmate peer workers, and the topic of compassionate release.
Afterwards, we chat with the prison’s chaplain, Keith Knauf. Keith per many reports, is the heart and sole of the hospice unit and oversees the Pastoral Care Workers. These are inmates that volunteer to work in the hospice unit, serving a mission that “no prisoner dies alone.” We chat with Keith about how hospice in prison is different and similar to community hospice work, the selection process and role of the peer support workers, the role of forgiveness and spirituality in the care of dying inmates, and what makes this work both rewarding and hard.
Part two of the podcast, which comes next week, is solely focused on the Pastoral Care Workers. We interview three of them in the hospice unit and take a little tour of the hospice gardens.
When the time of passing is close, emotions run high. When hospice if involved, it helps, but the pain of upcoming loss and all the unresolved issues are still left. In the US, people are taught to believe in happy endings. Generations have watched television shows and movies where in 30, 60 or 120 minutes all the issues are resolved and there is a last minute confession and a rebounding moment. Real life is neither as clean or as happy.
Does marijuana help in those final hours? In the moments with palliative or hospice care, anything that can help makes a difference.
Palliative care is medical care for people living with a serious illness, such as cancer or heart failure. Patients in palliative care may receive medical care for their symptoms, or palliative care, along with treatment intended to cure their serious illness.
Hospice care focuses on the care, comfort, and quality of life of a person with a serious illness who is approaching the end of life. Hospice is prescribed when a path to cure has come to an end and the focus changes to focus making the patient comfortable until the end.
Two evidence-based guidelines address the use of medical marijuana in a palliative care setting. The first evidence-based guideline explicitly recommends against the use of medical cannabis as a first or second line option for palliative cancer pain. The guideline suggests that it could be considered in the case of refractory symptoms and with careful consideration of potential risks. The second evidence-based guideline similarly recommends that medical cannabis only be used in the palliative care setting when other treatments have failed, and after consideration of the potential for adverse events and drug interactions.
In study after study, medical marijuana can helps increase appetite, relieve painful constipation, and diminish pain. Hospice focuses on the focus well being, knowing there isn’t a long-term cure. Currently, most science shows medical marijuana manages systems but not resolve an serious ailment or injury.
Perhaps equally importantly, marijuana is used in the hospice care setting to ease spiritual and existential suffering. Some studies showing an important therapeutic role for patients faced with the despair of a terminal illness, loss of functions, and a lifetime of reflections. A mild euphoria or sense of well-being can ease a patient’s mind, body and spirit as they come to terms with their fate.
In 2019, a study was conducted among hospice professionals. About half of the respondents were nurses followed by administrators and physicians. Regardless of legal status, hospice staff members were overwhelmingly in agreement that medical marijuana is an important tool in supporting their patients.
Though medical marijuana is legal in 40 states, plus the District of Columbia, conflicting federal laws present a challenge for hospice and palliative care programs whose patients are interested in medical cannabis or already using it to manage pain and other symptoms.
The situation is particularly challenging for hospices, which are primarily funded by Medicare. Many hospices say they cannot legally prescribe medical marijuana because it remains a Schedule 1 controlled substance under federal law.
Gallery: Cheryl Hauser smiles as she looks out the window Friday, Nov. 5, 2021 at her home in Hopkins, Minn. Hauser, who has Alzheimer’s disease, has decided to eventually hasten her death by voluntarily stopping eating and drinking after watching her brother die from it.
It’s not the dying I mind, Cheryl Hauser used to say.
It’s the leaving.
She left us this month. On her own terms, in her own time; surrounded by as much love, music and kindness in death as in life.
This is her parting gift to us. A chance to talk about the part of life nobody wants to think about.
The end.
“We would sing to her and rub her feet and her hands,” said Cheryl’s daughter, Wendy Longacre Brown, who chronicled those final days as her terminally ill mother voluntarily stopped eating and drinking to hasten the end.<
"You're in it together," said Brown, who has worked for years as a death doula, easing the transition from this life to whatever comes next. “There’s a lot of joy and laughter. But there is sadness.”
Cheryl had loved the life that Alzheimer’s was stealing from her.
“She was everything,” her daughter said. “She was someone who could sing in the grocery store aisle, then have a long conversation out in the parking lot with a total stranger.”
But Cheryl knew what was coming. She lost her brother Bill to Alzheimer’s, years before the disease actually killed him.
When she was diagnosed, she knew how she wanted her story to end. When the time came, she would VSED — voluntarily stop eating and drinking.
“When the day comes when nothing matters anymore, I’ll begin,” she told the Star Tribune in 2021. “My brother died of this disease and it was torture. I don’t want that for me and my family.”
Instead of languishing for years in memory care, she chose to spend her last weeks at home in Minnetonka. Friends visited, musicians serenaded her, and her grandchildren pressed her thumb into soft clay to create keepsakes. She sat outside in the sun, surrounded by summer flowers and birdsong.
One of Cheryl’s daughters is a birth doula. The other a death doula. Welcoming us into the world and helping us say goodbye.
“The more that death is part of the conversation and less of a taboo, the more we as a community can be present for one of the two most significant moments in your life,” Brown said. “It’s never too early to start a conversation of what people wish for around their end of life.”
Brown had helped other families through the goodbyes that nobody wants and everyone needs. Now she was the one saying goodbye. Every day, she shared photos and updates on her mother’s condition on cherylhauser.com.
The site started as a way to share news with family and friends. But it also drew strangers, who grieved with them and marveled at their generosity. In a culture that shies away from talk of death, here was a family showing us what dying looks like. Or what dying could look like.
“People often ask, did she have doubts? I can honestly say she did not,” said her husband, David McNally.
VSED is not a swift or simple death and patients in cognitive decline need special care to ensure that they are capable of giving informed consent. But this had always been Cheryl’s plan.
There were moments, as Cheryl was dying, when she would become confused and forget. Her family would sing to her, massage her legs as they cramped from dehydration, and offer her a tiny spritz of water or a cold spoon to hold in her mouth for comfort.
VSED cases are overseen by doctors and hospice staff. Caregivers were with Cheryl to make sure she was comfortable and had medicine to ease any pain or anxiety.
It was a death only possible in a family that talked about the end of life long before they needed to.
“Several times in the journey [in the four years between Cheryl’s diagnosis and death], I would say to her ‘How are you feeling about VSED?’ ” McNally said. “She would say no, I’m good, I’m going to do it. When my time comes, I will do it.”
The couple met when they were 60 and married when they were 70. Sixteen years. That’s all the time they were given. They made the most of their last four years together; traveling, going on adventures and advocating for the right to a dignified death.
Cheryl “was a very outgoing, very joyful person, just an extraordinary personality. She lit up a room,” he said. “She connected with people. She had this uncanny ability, when speaking with people, of making them feel special.”
There were incredibly sad moments, he said, as the disease progressed and her beautiful life started to slip away. Cheryl lost the ability to drive, to play the piano, sometimes she struggled to tell one grandchild from another. In the end, he said, she could do almost nothing for herself without help.
In May, she told her family she was ready.
Cheryl Harms Hauser, who had a smile that could light up a room, died on June 2, 2023. She was 76 years old.
Sherry Campbell, director of Welcome Home, stands with former resident Clint Jackson outside the hospice and medical respite home in Chattanooga, Tennessee, on April 2, 2023.
A few years ago, Mark Adams was diagnosed with colon cancer. His doctors didn’t want to operate, he said, because his recovery could be too risky without a clean place to recuperate. He was living on the street.
Soon, it was too late, his cancer too far along. That’s what they discovered after he moved into Welcome Home, a facility offering long-term medical respite and end-of-life care for unhoused adults.
Instead of getting better, he’ll likely live out the rest of his days there – one of a small number of places in the United States that offers unhoused people a comfortable and dignified option when they are terminally ill.
Sufficient end-of-life care in the United States is a growing problem for the general population, as America’s aging baby boomer generation needs more intensive and expensive help and supply isn’t keeping up. For many unhoused adults — who frequently lack a strong social safety net — long-term medical or hospice care are effectively inaccessible. In the absence of publicly funded solutions, private organizations and nonprofits are trying to plug the gaps, but the patchwork network of end-of-life care homes is far too limited to address the need.
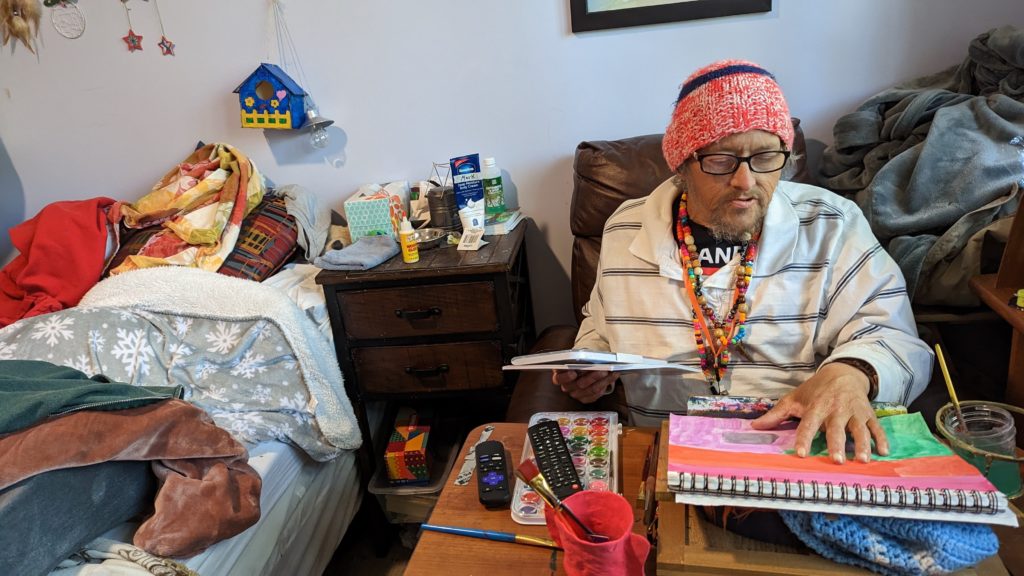
On a mild spring Sunday, Adams worked on a painting in his cozy, eclectic room – filled with vinyl records, potted plants and his own art – while his friend Clint Jackson relaxed nearby. Up the hill, Standrew Parker rested on a wrought iron chair in his yard, soaking up the early afternoon sun and chatting with his new roommate, Heidi Motley. Parker, 40, and Motley, 58, are staying there while undergoing treatment for cancer.
Mark Adams displays his artwork in his room at Welcome Home in Chattanooga, Tennessee, on April 2, 2023.
Across the country, there are a handful of facilities like Welcome Home, which sits on nearly five forested acres in Chattanooga, Tennessee. Some 1,300 miles west, there’s Denver’s Rocky Mountain Refuge for End of Life Care. Salt Lake City is home to The Inn Between, while Washington, D.C. has Joseph’s House. In Sacramento, Joshua’s House plans to open its doors this fall. Dozens more offer medical respite beds, generally for those undergoing long-term medical treatment. But outside of these organizations, experts told the PBS NewsHour that there are few other places where people experiencing homelessness can go for end-of-life or hospice care.
These facilities aren’t massive – Welcome Home has three medical respite rooms in addition to its four hospice beds, and is opening another house with an additional three rooms this month. Rocky Mountain Refuge, the smallest and newest of the group, has three beds solely for end-of-life care.
The need for those beds is great: People who are homeless are at far higher risk for many illnesses and conditions, such as heart disease. Medical research also shows that unhoused people’s bodies have often aged as if they were at least a decade older.
Being without a home is itself “a life-limiting diagnosis,” as Hannah Murphy Buc, a researcher who studies palliative and end-of-life care for people experiencing homelessness, wrote in the journal Caring for the Ages.
When someone is already in poor health, there are basic obstacles of living without a home – not having access to a fridge to store medications or the ability to secure narcotics for pain management, for instance. Some people without permanent addresses, like Adams, have reported they were denied treatment for their cancer due to the physical demands of recovery.
“Hospice and palliative care, but particularly hospice, is completely reliant on having a place to receive it,” Murphy Buc told the NewsHour.
For Adams, 51, living at Welcome Home has been life-changing, even though he often feels sick and he says he knows the cancer will likely kill him.
“I feel good here. I feel like I’m welcome here,” he said.
What we know about deaths among the unhoused
There is no official national data on where, when and how people experiencing homelessness die. According to an analysis by the National Health Care for the Homeless Council (NHCHC), at least 5,800 people died while experiencing homelessness in 2018. That’s almost certainly an undercount, and the report noted the actual number could have been anywhere between 17,500 and 46,500 deaths for that year.
With more people expected to become homeless and as that population ages, that mortality figure expected to rise, said Dr. Margot Kushel, director of UCSF’s Center for Vulnerable Populations and Benioff Homelessness and Housing Initiative.
“The truth of the matter is most of the country is entirely unprepared for this,” Kushel said.
An inspirational sign is displayed near a cookie jar in the kitchen of Welcome Home, in Chattanooga, Tennessee, on April 2, 2023. Residents gather nightly for dinners provided by volunteers as a way of fostering community.
Local reports can help explain what’s happening currently to those who can’t access end-of-life care. Across several months in 2021, deaths among unhoused people in San Francisco occurred primarily outdoors, in places like encampments, vehicles or on the street, a report from the NHCHC found. Others died in medical facilities; motel rooms, either rented by the person or as a shelter-provided space; other people’s homes; and homeless shelters.
Similarly, in King County, Washington, about half of the people experiencing homelessness who died in 2018 perished outdoors, according to a report from the council. Only 26 of the 194 deaths occurred in residences.
A 2022 report from the Colorado Coalition for the Homeless found that among the unhoused individuals who die of so-called “natural causes,” 30 percent died in hospitals or other medical facilities, and 25 percent died outside.
“That means under a bridge, on a sidewalk, behind a bush, in a tent,” said Brother James Patrick Hall, the executive director of Rocky Mountain Refuge.
While in prior decades people experiencing homelessness may have died from acute causes, such as violence or illness, the aging population of unhoused people is now living with the chronic conditions that plague many seniors, such as COPD, heart failure, strokes and cancer.
“These folks often need a lot of personal care. They have pain issues … It’s like a disaster, to be honest,” Kushel said. “What we found in Oakland is [that] a lot of folks just died on the street, short of breath, in pain, incontinent.” Others were admitted to hospitals, and some ended up at nursing homes or acute care facilities, “but it wasn’t where they wanted to be.”
When given a choice, people overwhelmingly want to die at home, according to Murphy Buc. Death at home can lead to healing in relationships and help soothe those left behind. But even when that’s an option, it can be draining for those doing the caretaking, she noted, even with hospice nurses visiting a few times a week.
In the U.S., “we don’t do death well,” Murphy Buc said.
The problem of older people dying on the streets, in motel rooms and in cars is the ultimate result of disinvestment in affordable housing, skilled nursing care and health care, experts at the NHCHC told the PBS NewsHour.
It’s not that people who become homeless are falling through the cracks, said Barbara DiPietro, senior director of policy at the NHCHC. Instead, people are often forced into “gaping caverns” where underfunded social safety nets, such as Medicaid and public housing, fail to catch them.
An older adult who has worked as a manual laborer her entire life might have a stroke and lose employment, be unable to pay rent and end up without a home, said Caitlin Synovec, senior program manager with the council’s medical respite team. Shelters frequently can’t help people with enhanced medical needs, so they have nowhere else to turn.
The unhoused population is also disproportionately vulnerable, low-income and people of color — all groups who have historically experienced disparities and may distrust the nation’s health care and social services systems.
In addition to that added barrier, people may just not know they have medical respite and end-of-life care options, Murphy Buc said. Many of the current residents of these facilities were referred there by health care professionals or social workers, but had not previously heard of them.
‘Health care isn’t housing’
Having a home, in and of itself, can be considered a form of health care, advocates say. Those who work or volunteer at care homes sometimes witness very sick people make dramatic recoveries simply because they have a safe, comfortable and stress-free place to live.
Though each facility operates slightly differently, these homes offer more than just a physical address, providing services like palliative care, case management and transportation. Volunteers and staff can remind residents to take medicine, ask how they’re feeling, and, crucially, drive them to appointments.
Before Standrew Parker lived at Welcome Home, he would have to travel to the hospital from his mother’s house to receive five days of cancer treatment every few weeks. In addition to being an unwelcoming environment, her house was about 45 minutes away by rideshare, which cost around $60 to $70, he said. To avoid the trip back and forth, he would instead often spend his days living outside the hospital.
“We didn’t have that money. So I was in and out, just like hanging out. If I had multiple appointments for days on end there, I just [stayed outside the hospital]. I would have to or I wouldn’t get the correct shots or the treatment,” Parker said.
Crystal Jones, nurse case manager at Joseph’s House in Washington, D.C., works at her desk on April 4, 2023.
Now, volunteers drive him to and from his treatments, and during his weeks off from chemotherapy, he recuperates in his room at Welcome Home. Beyond the care he receives, the empathy and compassion from staff and volunteers helped shift his entire perspective on healing.
“It’s like a world of difference between surviving and actually being able to get well,” he said.
A crucial goal of each facility is to establish a sense of normalcy for people whose lives have been thrown out of balance. Welcome Home serves dinner every night, where residents can gather and rib one another. People living at The Inn Between can join the resident council, which offers both community and a way to effect change, such as what times coffee is available. For the patients who recover enough, these homes can help them adjust to life outside of the facility so they can leave.
When NHCHC began their medical respite programs in the late 1980s, they were originally intended as short-term stabilization. However, some of the programs that specialize in medical respite have begun to consider incorporating end-of-life and hospice care into their models to fill the gap, said Julia Dobbins, director of medical respite at NHCHC’s National Institute for Medical Respite Care.
In contrast, patients without somewhere to go sometimes cycle between a hospital and the street, being readmitted when their problems are acute enough to warrant immediate care, and released when they’re stabilized, Murphy Buc said.
Sending still-sick people back to the streets is called “patient dumping,” and “it’s horrible,” Kushel said. But, she added, the solution can’t be that people live at a hospital for months on end until they die. That’s an inefficient use of resources, not to mention that it’s unlikely to be where a patient wants to spend the rest of her life.
Hospitals don’t want to deny people care, Kushel said. When she heard about Adams’ doctors refusing to treat his cancer while he was experiencing homelessness, she noted that his situation was not uncommon. Doctors worry about harming people who don’t have access to long-term, safe and clean care, but it doesn’t make it an easy decision.
“It happens all the time,” Kushel said. “And when you speak to the surgeons, they actually feel terrible about it.”
In the long run, even medical respite doesn’t solve the problem of where people can live, said NHCHC’s DiPietro.
“We often say housing is health care. Absolutely,” she said. “Unfortunately, health care isn’t housing.”
For many, providing medical respite or end-of-life care to people experiencing homelessness with their own limited resources can feel like a Sisyphean task.
For every person given a bed, there are countless others who need and can’t access one. Each organization can only serve their local community, leaving hundredsof people or more to dieon the street nationally each year.
Beyond what the organizations receive from state and local funding, there’s little — if any — government funding for long-term medical care or end-of-life care for people with no fixed address. These organizations’ funding models are largely reliant on grants and donations, without long-term stability.
“It’s local advocates who are seeing the suffering of their community members, and so they’re creating these programs that are funded by the good of people’s hearts, and that’s it,” Dobbins said.
Rocky Mountain Refuge, which opened its doors a little over a year ago, struggles to find enough funding to stay open, Hall said. That’s an experience echoed across the country.
“One of the stresses for us here is, every year, are we going to be able to keep our doors open because of the funding?” said Kowshara Thomas, director of Joseph’s House in Washington, D.C.
Founded in 1990 during the HIV/AIDS crisis, the three-story house in a quiet residential neighborhood has served community members dying of the disease for decades. This year, however, they lost a major grant that comprised 30 percent of their revenue, which worries Thomas. Other medical respites in the D.C. area receive Medicaid funding, and larger organizations are often better positioned to write grants and secure funding. But Thomas says Joseph’s House, with only eight beds, is too small to follow suit.
A memorial wall of former residents is displayed at Joseph’s House in Washington, D.C., on April 4, 2023.
The organization has largely, though not entirely, pivoted from end-of-life care to medical respite, something Thomas sees as both a result of better health among their community and a way for them to provide continuing care for people after they’re discharged. Joseph’s House has around 25 community members for whom they provide supportive services.
Thomas is also proud of the community that Joseph’s House anchors, with former residents coming back for meetings, social time and sometimes additional long-term or end-of-life care.
“Having a place where you can feel safe and get the support — the medical and the psychosocial support — is really what helps our community,” Thomas said. “Joseph’s House is, for some of our residents, the first time they’ve ever had family or felt like they belonged somewhere and they could just be who they are.”
My family member was clear: She wanted her life to end without extreme measures — to go when it was “her time” with no life support, no CPR, no intubation.
Though my family and her spouse knew this and loved her dearly, the reality of letting her go and following her wishes without “doing more” became difficult as her condition progressed. At the time of her death, medical interventions had sustained her life for several years — against her wishes.
Unwanted, aggressive medical care at the end of life can not only rob you of a peaceful death, it can also place an enormous financial and emotional burden on your loved ones. Fortunately, advances in healthcare delivery at end of life, such as hospice and hospital-at-home options, are combining with more candid and open discussions of end-of-life care to reduce the number of Americans who die hooked up to machines in hospitals against their wishes.
But it takes more than industry shifts and education to ensure that you or your loved one have a desired end-of-life experience. If you want to avoid end-of-life hospital stays, some proactivity is required.
1.Know what documentation you need
What if you were in a car accident? How would you consent to, or decline, mechanical breathing intervention? Advance directives — which can include many different types of documentation — are more than just planning for far-off end-of-life scenarios.
An advance directive should account for any scenario in which you are unable to speak for yourself.
An advance directive should account for any scenario in which you are unable to speak for yourself and need a healthcare proxy to be your voice, whether at the end of a long battle with cancer or after being rendered temporarily incapacitated by a skiing accident. Everyone needs such documentation, not just the sick and elderly.
The documents that set out what a hospital, elder care community or other caregiving entity should and shouldn’t do on your behalf can vary by facility and state, and the methods for ensuring they are considered legally binding can also vary.
2. Designate a healthcare proxy and be real about your choice
The legal and healthcare system will decide for you if you don’t designate a healthcare proxy yourself, with your spouse being the default and adult children second. That’s a pretty solid default, but your closest loved ones may not always be the best choice
Ask yourself: Will they be able to let me go after a long life when I’m ready to rest? Yes? Lovely. But what if I’m in a car accident tomorrow and life support is offered? Will it be fair to ask this particular person to focus on such decisions? It’s quite possible. But it may be kinder and more prudent to say, “I love you, and so you’re not the one to make these decisions. I want you to be holding my hand when I take my last breath, not deciding if I should be on life support.”
For single people without children, it is imperative to have a detailed advance directive.
End-of-life decisions are particularly fraught for unmarried people. While the healthcare system does look for legally binding end-of-life wishes documentation, if no such documentation is found, there’s a possibility that a physician would expend unwanted efforts to extend your life. In extreme cases, the hospital ethics board could become involved in decisions you may have wanted to keep within your circle of loved ones. For single people without children, it is imperative to have a detailed advance directive.
3. Use free resources to plan with your family or doctor
Contrary to popular assumption, you don’t necessarily need an attorney to complete an advance care plan — though it may be advisable in specific circumstances. If you do choose to hire support, weigh that cost against the costs of not planning — which can include unplanned stays at nursing homes, costly interventions that may not result in extending life in a positive way, or family disputes over your end-of-life wishes.
Every state has free, downloadable documents for advanced-care planning available for their residents. If you find them challenging to navigate or understand, your physician can also guide you to social workers and other support. The secure online portal. My Living Voice is one example of a free resource that helps simplify the process of documenting your advance directive. It can help you to think through who your proxy should be, to document your preferences for care during a medical crisis or life-extending care, and to make those wishes both legally binding and known to your physicians, your insurance company, your healthcare proxy and your family.
Prioritize discussing an advance directive at the start of your next physician appointment with a simple ask: “I’d like to do an advanced care plan. How should we go about that?”
4. Share your plans
Too frequently we assume our designated healthcare proxy will “just know” that they are the proxy and how you feel about what decisions will need to be made. Too frequently, that simple communication and documentation doesn’t happen. If the role comes as a surprise to them in the midst of a health crisis (or even an anticipated health event), it can cause undue stress on someone you love.
Another common scenario: You have a living will, but it’s in a file in your closet, completely inaccessible to those who need it most, like your physician
Actualizing your end of life wishes requires that your advance directive is documented, communicated and accessible.
Actualizing your end of life wishes requires that your advance directive is documented, communicated and accessible. If required in your state, get it notarized. Communicate its contents with your loved ones and doctor. Provide your loved ones and healthcare providers with copies, both paper and digital if possible. Furthermore, if you have children, make your plans and proxy designation clear to each one of them to save them from agonizing disputes. Consider the right time to have these conversations with your family based on your unique family dynamic and set a time for that discussion.
Not sure how to start the conversation? Print this article and say, “I was reading this, and it made me think. Can you all read it too and then we can talk?” Legally documenting your wishes can provide your loved ones with peace, structure and protection at a time when they might have their head in their hands, saying, “I don’t know what to do.” Give them the strength and confidence that helps them take the actions you want taken.
— A death doula explains how to respect and accept different end-of-life choices
By Lee Woodruff
I was on the other side of the world when I got the text. “Did you know Karla is dying?” my friend wrote. “They called in hospice and she only has a few days to live.”
My enjoyment of a long-planned vacation with my husband suddenly came to a screeching halt in my brain. How could this be? I’d spoken to Karla * a few months ago and we’d celebrated the news that she was pronounced cancer-free. We’d gabbed away for almost an hour, catching up on kids, her future plans and the challenges with chemo, all with her signature optimism and honesty.
I was never someone Karla would have counted in her inner circle. We were in different places in life, my youngest kids still home at a time when she was enjoying dinners out and weekends away. I’d met her more than 20 years ago as part of a group of moms who sat on the sidelines at their kids’ games and drove one another’s children to playdates and sleepovers. Life had moved us to different cities, and a year or more would easily go by without seeing one another. Any time we spoke, we’d always pick right up where we’d left off. She was that kind of friend.
Listening to the relief in Karla’s voice on that last, long-ago phone call, I recalled that we’d talked about a getaway weekend with girlfriends at the beach and rebooting that group dinner we’d canceled when her doctor unexpectedly discovered a small, pesky tumor. The last of it, she’d said.
When communication stops
For the past two years, Karla had been throwing everything she had at the disease, using a combination of the finest cancer care, physicians and hospitals, with holistic medicines, organic foods and juicing. Nothing that contained any chemical or synthetics was allowed on or in her body. Karla, or so we thought, had won.
How had this rosy picture gone into a death spiral so quietly? It wasn’t so much the shock that the cancer was back. Live long enough and you understand that cancer is a sneaky thief. Anyone who has experienced a brush with cancer never fully lets their breath out. But still…. Days to live? How had someone who had brought us along so fully on the journey, who had grabbed life by the throat and been honest and transparent about her illness gone so quiet? How could we, her friends, not have known?
Next came the wash of guilt. Each person responds to illness or injury so differently. There is no one playbook or template. My style has always been to take the cues from others and to give everyone space to do what was comfortable. But now, knowing I wouldn’t make it back in time to see her, I regretted showing up at her door.
When my journalist husband was injured by a roadside bomb in Iraq 18 years ago, my instincts were to immediately pull the shades down from the outside world. The prognosis was so devastating, I wanted all my energy to tend to him and help our kids process what was happening. I drew my circle tight, initially letting in mostly family and a few trusted friends who helped with critical roles to move life forward. I understood shock and trauma, but it was hard not to personalize it, even though I knew that was ridiculous.
Loss is a part of life
At a certain stage of life, loss becomes a theme. And there is no question that when something strikes out of the blue, a sudden diagnosis, a death, accident, or a spouse who leaves, we cannot help but think of ourselves. How would we handle it? How will we handle it when it’s our time to die? I’d seen people around me die in many different ways, from flinging open the doors and having a party to closing the curtains and going quietly, as Karla had done.
My in-laws never wanted to talk about dying or even do much in the way of preparation. My mother talked about it frequently and matter-of-factly, especially toward the end. She had every detail prepared and outlined, but she lost so many opportunities to live in the moment. There is only so much we can control. What would I choose when it was my time? It was impossible to know.
End-of-life choices
Alex Rosen, 42, from Armonk, New York, is a death doula. Her job is to support, guide and provide companionship and comfort for those at the end of their life. Ideally, Rosen works with people from diagnosis through the transition to the end of their life, from their emotional state to the physical setting, whether it be in a home or hospital.
“How we choose to be and exist at the end of life is our choice and our personal journey,” she says.“When possible, it should look and feel how a person wants it to, within the confines of the medical system.”
Part of the work Rosen does as a doula is helping the person and their family accept death and make it feel as comfortable and safe as possible.
“In our society and culture, talking about death is so taboo. So many things are said privately and behind closed doors,” she says. “Part of being alive is understanding that all of us are going to die. The more we can talk about it, the more we can begin to accept it.”
One of the insights I gleaned from talking with Rosen was the potentially harmful language we use around “battling” disease as a society. While comments about “waging war” against cancer can rally a patient to summon energy and desire to combat a disease, if the disease “wins,” there can be a sense of letdown.
“There’s a societal mentality around losing,” Rosen says. “And people who thought they’d ‘beaten’ the cancer or had the potential to, can experience a feeling that they didn’t fight hard enough, weren’t strong enough, that their body failed them. That mentality can bring a feeling of shame and failure rather than a sense of calm and peace at the end of a physical life.”
Karla was a competitor; I could imagine her devastation as she received the grim news from her doctor after a scan that revealed the cancer was back. The story didn’t sound right. From completely cancer-free to riddled throughout her body? But then again, this wasn’t information I had any right to know. This was Karla’s story to tell and to handle any way she chose. She had already been through so much.
The aftermath
I’m still processing Karla’s loss and the way in which we all learned about her dying. I’m still shocked on some level. The news feels like a rug that got pulled out from under me and others who knew her. And of course, there is still so much guilt and remorse over what I would have done differently, had I known. But guilt is a useless emotion, especially when it comes to death.
Karla wouldn’t have liked all this hand-wringing from her friends, and that thought comforts me. I am also consoled by the knowledge that she chose this. I know that this was the way she wanted it to go down because there were many opportunities to do it differently.
You take the good with the bad, I can imagine Karla saying. And I’ve had a pretty wonderful life.
My hope for Karla is that she got to experience death on her terms. By all accounts, she did.
Case in point: A new JAMA Open Network study found that cancer patients in states with palliative care laws, which can require health care providers to tell patients about their end-of-life treatment options, were more likely to die in the comfort of their home or in hospice care rather than a hospital bed.
Why it matters: The vast majority of people want to die at home, but many do not. End-of-life spending on hospitals can also quickly drive up costs while making little difference in length or quality of life.
What they found: Cancer patients dying in a state where a palliative care law was in place was associated with a 12% to 18% increased likelihood of dying at home or in hospice care, researchers found, depending on how prescriptive the state law is.
Nationwide, researchers found that 22 states have either a non-prescriptive state law, like an established advisory council, or a more prescriptive state law, which can require hospitals to have palliative care programming for patients.
For patients with a serious illness that was not cancer, the results were similar: Researchers saw a 23% to 43% increased likelihood of a patient dying at home or in hospice in states with nonprescriptive and prescriptive palliative care laws, respectively.
The bottom line: With the number of aging Americans projected to dramatically increase in the coming decades, understanding how to cater to patients’ preferences in end-of-life care will only become more important.
“In this study, we observed that a state-level intervention had a measurable association with place of death for individual decedents,” researchers wrote. “This finding was noteworthy given the difficulty with improving palliative and end-of-life care delivery in the US.”


 We start off part one by interviewing Michele DiTomas, who has been the longstanding Medical Director of the Hospice unit and currently is also the Chief Medical Executive for the Palliative care Initiative with the California Correctional Healthcare Services. We talk about the history of the hospice unit, including how it was initially set up to care for young men dying of AIDS, but now cares for a very different demographic – the rapidly aging prison population. We also talk about the eligibility for the unit, what makes it run including the interdisciplinary team and the inmate peer workers, and the topic of compassionate release.
We start off part one by interviewing Michele DiTomas, who has been the longstanding Medical Director of the Hospice unit and currently is also the Chief Medical Executive for the Palliative care Initiative with the California Correctional Healthcare Services. We talk about the history of the hospice unit, including how it was initially set up to care for young men dying of AIDS, but now cares for a very different demographic – the rapidly aging prison population. We also talk about the eligibility for the unit, what makes it run including the interdisciplinary team and the inmate peer workers, and the topic of compassionate release. Afterwards, we chat with the prison’s chaplain, Keith Knauf. Keith per many reports, is the heart and sole of the hospice unit and oversees the Pastoral Care Workers. These are inmates that volunteer to work in the hospice unit, serving a mission that “no prisoner dies alone.” We chat with Keith about how hospice in prison is different and similar to community hospice work, the selection process and role of the peer support workers, the role of forgiveness and spirituality in the care of dying inmates, and what makes this work both rewarding and hard.
Afterwards, we chat with the prison’s chaplain, Keith Knauf. Keith per many reports, is the heart and sole of the hospice unit and oversees the Pastoral Care Workers. These are inmates that volunteer to work in the hospice unit, serving a mission that “no prisoner dies alone.” We chat with Keith about how hospice in prison is different and similar to community hospice work, the selection process and role of the peer support workers, the role of forgiveness and spirituality in the care of dying inmates, and what makes this work both rewarding and hard.