Embracing the natural stages of the dying process through hospice care
By Lauren Glendenning
When patients need hospice care, family members and other loved ones often feel overwhelmed with emotion. A caring and supportive hospice team can help alleviate some of these feelings.
We asked Kristine Cooper, executive director of Home Health and Hospice at Memorial Regional Health, to help readers understand more about hospice care at MRH and how it affects patients’ families.
What are some ways that hospice care can relieve stress for those who may be in charge of an elderly loved one?
Kristine Cooper: Hospice really provides support not only to the patient but also to the caregivers. We have nurses that spend time with caregivers, educating them about the disease and dying process. We also have our LCSW (Licensed Clinical Social Worker) who spends time with the patient and caregivers, discussing end-of-life planning. She also works with caregivers and families to address anticipatory grief.
Are there any myths about hospice care you’d like to clarify?
One myth would be that hospice hastens death. Hospice really embraces the natural stages of the dying process and neither intends to hasten or prolong death. Our team partners with the patient and family on the journey. Another myth is that hospice is expensive. Medicare actually covers the cost of hospice, including medications to treat symptoms related to the patient’s terminal diagnosis as well equipment needed to care for the patient safely in their home.
Why is it important for families to know about hospice care?
Hospice is not about giving up hope, it’s about refocusing hope. With hospice, there is hope that pain and other symptoms can be managed so that loved ones can live their best life in their final days. Hospice also offers hope to families and caregivers by providing support during this difficult time.
When is hospice care is necessary?
Hospice is here for patients who have been diagnosed with a life limiting or terminal illness with a life expectancy of 6 months or less to live.
What kind of care do hospice patients receive?
Hospice provides nursing, emotional and spiritual support. Hospice can also provide support from physical, occupational and speech therapy with the focus of helping patients move safely. We also have volunteers that can provide companionship and assist with light housekeeping and cooking. All these different services make up the patient’s care team that works closely with their doctor. The overarching theme about hospice is that it is really about what the patient or family needs.
For many people, the thought of being surrounded by death (and have that be a central part of how they earn their living) can seem quite morbid. But for Alua Arthur, the founder of the end-of-life planning service Going With Grace, it feels exactly the opposite.
Arthur is a death doula—also often referred to as a “death midwife.” Arthur’s journey to becoming a death doula is a profoundly personal one, but she represents a number of professionals who are active in the growing “death wellness” and “death-positive” movement. As Fast Company‘s Rina Raphael previously reported, this movement rests on the notion that having a good death is “part of a good life.”
Fast Company recently spoke to Arthur about her motivations for becoming a death doula and how she copes with work-life balance as she helps others through the grieving (and often stressful) administrative process that comes before and after a loved one’s death. The interview has been edited for length and clarity.
Helping people become clear on what death looks like
A death doula is a non-medical professional who provides holistic support for the dying person of the family and the family members. I help the people who are close to death on what it looks like. After that, I help family members deal with their affairs.
I also work with healthy people. The way I conceive it, as soon as someone comes into any recognition that one day they’re going to die, that’s the time to start preparing for that, so I help them with an end-of-life plan. It’s where we write down all the stuff that’s going to be a pain. We get clear for what their desires are for life support, and who’s going to make the decisions for them. We walk through important information and documents, like where’s their birth certificate? Where is their retirement account? Where do they bank?
I also help people who are terrified of death. I find that people are more afraid of the dying process than death itself, so with them, I do death meditations. This looks like us going through the eventual decline of the body, their systems shutting down, and their breathing becoming ragged. It’s an opportunity for the person to lay there with whatever it is they experienced. A lot of times, people experience a sense of peace after going through this process.
The desire to build a career around death
Growing up, I wanted to be lots of things. I really wanted to be an astronaut. I loved to read and immerse myself in another world. I also wanted to be a conductor. I applied to a music conservatory, but I ended up in a liberal arts school that had an okay music program. I got involved in student government and decided to go to law school. I worked in property law, starting with government benefits, and then I moved to domestic violence and then not-for-profit development. I fumbled around for 10 years and started getting really depressed, so I took a medical leave of absence. That’s how I found death work.
I met a woman in Cuba. She had cancer and was traveling, and we bonded. We spent 14 hours on the bus together, and I asked all the difficult questions. What would be undone in her life if the disease killed her? What does she think happens after she dies? Did she live with the recognition of death constantly? They were questions I never really had myself. That was the first time it hit me that death was very real and that we don’t talk about it enough. It became clear that I wanted to spend my career talking about death.
That was solidified when my brother-in-law got sick and died. It showed me how all the ways that we do it now are broken. We had so many questions—how do we transfer the title for his vehicle, and what should we do with his leftover medication? There was nobody to answer them.
A day in the life of a death doula
A typical day always includes a lot of emails. So many emails. The part of my job that stresses me out is the business part. God, it’s the worst! I need to go back to my vision of helping people feel less alone to keep me in clear focus.
I start my day checking on various things—with the people who are dying, how things were over the course of the night. I’ll also check on plans for any funeral procession. I do a lot of phone calls and talk to therapists who work with people that are dying. If I do have clients that are dying, I see them in the afternoon, or I will see my end-of-life planning clients.
These days, I also do a lot of education around death and dying. I’m doing a lot of talks to reach people about how to do this work because we’re all going to have to do it for somebody in our lives.
When it comes to work-life balance, I do things like meditate daily, exercise regularly, and drink a gallon of water every day. I just got my nails done. I don’t deny myself pretty things.
On death and relationships
I talk about death all the time with my friends and family. I think sometimes I can be a little bit annoying because I want people to be authentic in their decision-making. I tend not to tell people what to say or do, and I listen actively. My best friend and I, we always have challenges because she always wants to tell me what to do. It is a struggle for my friends who have a hard time with the concept of their own mortality, because I’m talking about it all the time.
I don’t push the issue with my friends who are uncomfortable, but with my family members, I do. For my dad, he first had to come around to the idea that I wasn’t going to be practicing law anymore. Being an African parent, he wanted me to be either a lawyer, doctor, or engineer. I was like, how about death? He was like, how about what? That was a little tricky. But eventually, we got around to talking about it. After all, I’m the one who’ll have to deal with it when it happens.
I think people actually want to talk about death, but they feel like they don’t have permission to do so because it’s “heavy.” Well, it’s a regular part of living. Without death we wouldn’t have life. It’s funny: when I meet someone for the first time and I tell them I’m a death doula, so many of them say, “Oh, when x died, I wish that you had been there.”
They’re changing how we approach end-of-life care.
by Kristen Fischer
To many people, the word “doula” refers to a childbirth coach. But doulas aren’t only available for when life begins — they can help when life ends too.
An end-of-life doula is a nonmedical professional trained to care for a terminally ill person’s physical, emotional, and spiritual needs during the death process. While you may never have heard of this position in the healthcare field, there’s quite a market for “death doulas.”
The role is also referred to as an “end-of-life coach,” “soul midwife,” “death midwife,” or “transition guide.”
Searching for a way for patients to have a “good death” has become increasingly important in the medical community. Last year the medical journal Behavioral Sciences devoted an entire issue to communication over end-of-life issues to ensure patients’ end-of-life wishes were realized.
“In the American culture, where the majority of people die in hospitals, death has been routinely denied, sterilized, and/or removed from view,” said Maureen P. KeeleyTrusted Source. Keeley, who is director of graduate studies at the Department of Communication Studies, Texas State University, wrote in the journalTrusted Source. “Talking about dying with the person that is terminally ill can relieve anxiety for both participants in the conversation, and it can help ensure that final wishes regarding treatment at the end of life are honored.”
Currently there a few organizations that administer credentials for death doulas, including the International End of LifeDoula Association (INELDA), International Doulagivers Institute, and Lifespan Doula Association (LDA).
Jeri Glatter, vice president of INELDA, said her organization has trained about 900 end-of-life doulas in the United States since 2015. The organization provides personal certifications as well as training to hospital staff members including hospice workers. In addition to popularity in the United States, there is a significant interest for training in Asia.
Individuals who seek a personal certification often go on to run their own businesses. An INELDA certification involves attending a training session and then applying for the credential. Several requirements, including hands-on work, must be completed to become certified, which takes the average person six to nine months and is quite rigorous, Glatter said.
Life as a death “doula”
For those who embark on the career, it’s quite a personal choice.
Kelly Sanders, RN, an end-of-life doula from Michigan, worked as a nurse in the long-term care field for many years before becoming a death doula.
“I saw people die without any control over the process,” she recalled. “It seemed as soon as the terminal diagnosis came, the patient became invisible to family and friends. They would talk as if the patient was already gone, even while the patient was in the room.”
She said that hospice cannot provide all of the services a person needs — especially the emotional help — when they have a terminal prognosis.
“Hospice does a great job taking care of the medical aspect of dying, but due to the changing nature of healthcare compensation, little time was left for the other aspects of dying that are just as important for a peaceful passing,” she said. “End-of-life doula services fit that need.”
She said there is a big misconception that hospice provides the same services as a death doula.
“I think it was the overall idea of hospice, but because of Medicare/Medicaid cuts, hospice only has time to deal with the medical needs. They do not have the training to even do the work of a doula.”
Death doulas can fill a gap in care. People can work with a death doula before they reach a point where they qualify for hospice. And an end-of-life doula is able to devote themselves to a single person, going in without an agenda to fulfill that person’s needs.
What a doula does
Sanders said a huge part of the job is to establish trust and build a relationship with patients and their families. It’s important to respect their wishes and not influence their decisions, she said.
As part of her services for Peaceful Journey Home, LLC, Sanders is often asked to take family photos or assist patients in writing letters to ask for forgiveness. Some patients hire her to plan their funerals.
“The more time that you have with a person, the more you learn and it is easier to learn their life story and advocate for their wishes,” she said. Sanders said it’s important to be flexible during the process. When she notes a patient’s wishes and they change, she gently reminds them of their initial preferences but allows them to change their minds.
“It is their death, so they can certainly have the right to change focus,” she said. “Sometimes we don’t always know what we want, and we mold the idea as we go along.”
Some family members rely on the doula to remain present and keep them informed on the patient’s status while they take a much-needed break.
A death doula can also answer questions about the dying process and empower family members to create the kind of environment that the person dying has requested, said Christy Marek, an end-of-life doula from Minnesota who sees patients locally and offers her services via phone and video conference.
“We help family feel competent and central to the process and less afraid of the unknown,” Marek said. “It is a true partnership, and I think that’s the best support we offer for families — assuring them they are not alone.”
Typical services include helping patients create legacy projects or planning a person’s final days and moments. Mostly, Marek said she focuses on creating a safe space for clients to do the emotional and “soul” work needed to help them prepare for their death.
“I help the individual who is dying to stay close to what is most important in the time that remains, to focus on what is possible rather than on limitation, and to support their loved ones in staying as involved as desired as things progress,” Marek said.
One of the biggest advantages of having an end-of-life doula is the continuity of care and consistent support. Patients often transition from actively seeking curative treatment to no longer receiving treatment. Some are put in hospice, and some “graduate” from hospice before their death, Marek explained.
“These are all circumstances where care teams change and support systems get disrupted and lost. Having an end-of-life doula throughout the process of end of life ensures that there is a consistent supportive foundation that remains the same,” Marek said.
Family ties can help lead to a ‘good death’
Sanders said it is best when family members are actively involved with the doula to respect the patient’s wishes.
“I try to encourage and engage families to participate in the process, especially if they are not in agreement with the process,” she said. “All input is valuable, but I like to politely remind families that this is not their death. So, the dying person’s wishes and needs come first.”
“Many times, a patient is not able to articulate their wishes, such as cases of dementia, but the patient still deserves a lasting tribute,” Sanders said.
Marek said her goal is to serve the patient even if they forget they hired her, don’t remember what they initially asked for, or have different wishes than family members.
She said her ultimate goal is to get what the patient wants — even if she is hired by family members.
Aside from bedside manner, death doulas have to run their business. Their services might be too costly for some patients, and insurance is unlikely to cover their work.
Sanders said an individual package may cover 20 hours for $700 plus an additional fee if the patient wants more time with the doula.
Marek said that prices typically are flexible and can include a weekly or monthly retainer or individual sessions and packages. An end-of-life vigil, which takes place during the active dying process, can range from $1,500 to $3,500 or so.
Leaning ‘into’ the fear
Anyone who is struggling with their diagnosis or wants to leave something behind for family, may want to seek out a death doula.
Sanders loves her job but admits that it’s hard when a patient passes away. “That part never gets easy,” she said. “I take comfort that I was able to help them transition on their terms.”
“Our culture holds so much fear around death that when we find ourselves face-to-face with it, either our own mortality or that of someone we love, we typically don’t know what to do,” Marek added. “It’s incredibly scary to face into the unknown, so most of us do our best not to.”
But Marek said ignoring real life can be harmful.
“It affects not only the person who is dying, but the entire circle that surrounds them,” Marek said.
The presence of an end-of-life doula helps people “lean into” the pain and fear of the unknown. That frees up space and energy so they can experience the emotions including actual joys that come with death. She said the doula’s experience helping others through death can ease the process for both family and patient.
“The comforting presence of a doula enables opportunities for the dying to connect more deeply with loved ones and to enjoy the time that remains, focusing on possibility rather than only on limitation, on what they can control rather than on what they can’t,” Marek said.
She said she believes that many people would benefit from having an end-of-life doula because they can help foster connections even during an emotionally painful time.
“I believe a death doula — the openhearted presence of someone who won’t turn away in the face of suffering and will offer support to help us work with it rather than fight against it — would benefit everyone at end of life.”
Australian oncologist Ranjana Srivastava says: In order to die a good death, it helps to have lived a good life. And a good life must involve contemplating one’s own mortality.
By Sally Pryor
It’s a circular philosophy that, as it happens, doesn’t feature nearly enough in the average person’s thinking, at least not in secular Australia. But for oncologist Ranjana Srivastava, living and dying are completely intertwined, and it’s those patients who are able to accept their own death – inevitable, albeit often untimely – who have inspired her to contemplate what it means to die well.
It’s a question, she says, that many doctors don’t manage to properly consider. The medical profession is focused largely on treating illness and making patients better.
“As I have matured as a doctor and became an oncologist, I have been very struck how there seems to be very little place – or no place, sometimes – in our day to talk about dying, let alone dying well, but simply dying,” she says.
And yet her work involves dealing, daily, with dying patients, often caught up in the complexities of the medical system, at sea when it comes to dealing with what happens next. From the young woman, unable to work and far away from her family, to the 80-year-old man, refusing to accept an end point when it comes to treatment that isn’t working, Srivastava can see all the ways that our society – focused primarily in succeeding and moving forward – leaves little room for contemplation.
Srivastava has been writing, compulsively, since childhood, but it was relatively early in her medical career that she realised the power of story-telling, of human narrative, in allowing her to empathise with her patients, and to do her job properly.
“I’m incredibly aware that no matter how ambitious you are as a doctor, you can only do so much, so that’s why a lot of my public writing and thinking has been devoted around how do we empower everyone else, and how do you not just talk to doctors, but how do you go around doctors and talk to people and patients?” she says.
Her latest book, A Better Death, is a meditation on all the different ways in which death, and our awareness, can give meaning to our lives, even without a terminal illness.
“I guess I saw from an early age that what resonated with me, even as a trainee doctor or even going back as medical student, was someone’s story, because you could present a sterile case,” she says.
We’re sitting in a bustling Melbourne cafe, amid a noisy Saturday morning brunch crowd. On the face of it, it’s a jarring setting in which to nut out the concept of death, but Srivastava has a tranquility about her – a calm and blessed kind of reason – that makes you think she’d be the perfect person to have to deliver bad news, and to guide someone through the process of dealing with a terminal diagnosis. Those familiar with her writing – she is a regular columnist in The Guardian – will know that her commentary often starts with the story of an individual. It’s these personal stories that often drive the point home more vividly than any textbook.
“When I began writing, I thought, well how do I convey what I feel without illustrating why?” she says.
“And I continue to think that the way we empower people and the way we educate people is through letting them get a glimpse of themselves in each of those patients.”
One of the most important lessons she has learned is that everyone has the ability to control the way they die, through the way they choose to live out their last days. The many stories in A Better Death bear this out in different ways, but all with the same ultimate conclusion: if we could all live knowing that we will one day die, our lives will have more meaning, and we will be more motivated to leave some kind of legacy. Insisting on further treatment, even when it has become futile, or refusing to make arrangements for family and help them plan for the future, can make dying well impossible. But how individuals respond to dying has as much to do with society’s fear of morbidity, of talking about death, as with the individual.
“I absolutely think we have control over it, but the more I work, I think that it needs to be almost a societally determined thing,” she says.
“I think it’s very difficult for an individual to do this on their own, because there are so many forces. I will see this, where one of my patients will say, ‘I think I’m ready to just go peacefully, to stop treatment, to focus on being outside on a day like this and enjoying the gardens’, and someone else, who has not come to terms with their mortality but someone close to that patient, will have a different view. And I think it’s always easy to get taken in by that, and I think our medical system makes it very difficult to call it a day.”
Ultimately, she says, dying without a sense of peace is costly, both to the individual, and to society at large.
“There is an enormous cost to the family and to survivors, and this borne out by research and evidence, and then there is the cost to the taxpayer and society, so at every level there are serious costs,” she says.
“I think it’s driven both by patients and doctors, I would say, I don’t think every doctor is pushing patients to have more treatment, to not adopt palliative care, to not think about quality of life, I don’t think it’s as binary as that, and I think it goes back to the kind of society we are. There’s a lot of instant gratification in life – you want something, you get it. You see something, you can buy it, and health literacy is low in general. So I think people genuinely have trouble believing that many chronic illnesses and terminal illnesses cannot be reversed, and are not curable.
“We all have to ask this question of ourselves as to how we are going to contemplate our mortality and not just leave it to our doctors.”
And yet, she says, her work – and the world in general – is filled with examples of hope. While she is “continually astonished” by the number of elderly patients who, when asked, say they have never thought about dying, she is often consoled by examples of people who have thought the whole thing through.
“Just in the news I was listening to Bob Hawke’s widow speak about his death, and one of the things she said that quite struck me was Bob felt he had nothing else that he wanted to do – he was ready,” she says.
“And I thought, here is a man who has soared to the heights of accomplishment, and somehow he has managed to step back and back every year and every decade, until he has reached a point where he says, I have done what I need to do… I found that remarkable, and that’s why there is so much peace associated with him – he lived to a good age, he was able to live well, but he was able to articulate to the family left behind that he was ready to go, and I think it’s very consoling.”
How does she think she will come to deal with her own mortality?
“That’s a really good question. I would like to think that a career in oncology will not have been wasted when it comes to my contemplating my own mortality,” she says. “The reason I could never be sure about this is that I see how people can change when they are ill. It’s very difficult to be over-confident about how you would be when you are sick, when you are speaking about it when you are well. It’s something that each of us has to experience for ourselves. But I do feel that I am more blessed than most in having a lot of good teachers.”
As Robert Fuller lay dying, he knew he was not alone.
His husband, Reese, stood by his head, crying into a pink towel. They’d been married that morning. A soprano sang over the mezzo piano melody of a violin, soft, but enough to fill the small, crowded room. Those closest to him laid their hands on his arms, torso, thighs and shins.
Downstairs, in the common room of Primeau Place, the affordable housing complex in which Fuller lived, the atmosphere was jovial, full of memories, food and music.
But later, in the bedroom as Fuller’s eyes closed, the gravity of the moment was palpable — to be there was an honor beyond grief.
Perhaps a few people in the room had watched a person die. It seems unlikely any had ever received an Evite to a combination wedding/death-day themed with Hawaiian shirts, courtesy of the host. But there’s a first for everything.
There are those by profession or by predilection who choose to stay with the dying until the dying is done, to comfort the loved ones left behind and ease the souls of the deceased into whatever comes next. They sit in calm vigil so that others, like Robert Fuller, need not be alone.
These are their stories.
Nancy Rebecca
Nancy Rebecca performs a marriage ceremony for Reese Baxter and Robert Fuller.
At 10:30 the morning of Robert Fuller’s death, Nancy Rebecca joined Fuller and Reese Baxter in marriage.
She anointed them with nag champa oil, rubbing the scent of magnolia and sandalwood into their hands and asked each to take the other in lawful and spiritual marriage. They obliged.
For nine and a half hours, the two were wed. And then, at roughly 8 p.m., Fuller exhaled his final breath.
To Rebecca’s eyes, it wasn’t the end of Robert Fuller. This was simply a new beginning.
Rebecca isn’t just a marriage officiant. That happy task was more of a favor than a calling.
Rebecca is a healer of conventional and unconventional methods. She practiced as a hospice nurse for eight years, caring for people as they groped blindly toward the eventual conclusion of life. That work takes a toll on the living as well as the dying. In 1994, she bought a book on meditation and gave the calming practice a try.
Everything changed.
“I went to bed and I had a spontaneous out of body experience,” Rebecca said. “When my spirit came back to my body I could see energy fields and I could see spirits.”
Initially, Rebecca found the experience overwhelming, she said. After all, she was a registered nurse, trained in Western medicine. Seeing spirits and energy fields simply wasn’t done.
“In some ways, the energy fields I see around people are quite beautiful. That is not what was disturbing me,” Rebecca said. “It didn’t fit with what I thought to be the truth.”
Rebecca decided to consult professionals.
Rebecca’s mother was a psychiatrist, her father a medical doctor. Afraid of going to an outside physician with her concerns, Rebecca went to her parents. Her mother reassured her.
“There’s nothing wrong with you,” her mother said.
It took time to process her new, perceptive abilities, to parse what and who she was seeing. But it afforded her the capacity to stay with people under her care, observing the angels that came to visit them and helping them understand their own brief glimpses into the beyond at the end of their lives.
Rebecca works mostly with the living these days, helping them to heal their bodies by righting their energies through meditative practice. However, her wife had known Fuller for years, and although he didn’t feel that he needed her healing talents, the pair did have discussions about what came next.
One day, she asked him what he thought the afterlife would be like.
“He said, ‘Well it’s a realm of judgment and grace. For me I hope it leans a little more toward grace,’” Rebecca recalled.
“I said, ‘Based on my experience, it does,’” Rebecca said.
Sile Harriss
Sile Harriss, a music-thanatologist by training, played harp for the dying and their families for nearly 20 years.
The harp in Sile Harriss’ apartment is roughly 22 pounds and rises to the level of her chest when she stands next to it. The burnished gold of the maple wood glows in the low light — though she’s had it for decades, the instrument looks as though it was purchased the day before.
It’s small for a harp, Harriss said. It’s a Celtic harp, not an orchestral version, meaning it lacks pedals and has fewer strings, a deficit made up for in part by small levers at the top of each string that allow her to adjust the note produced by a half step.
That’s OK, though. She could hardly bring a larger instrument into hospital rooms.
For nearly 20 years, Harriss worked as a music-thanatologist, employing ancient melodies and lyrics to respond to the needs of the dying and their families. It’s a unique profession — Harriss estimates there are only 100 of her colleagues in the United States.
Music-thanatology is more than beautiful music, Harriss said. It’s about using the cadences and meters of musical traditions from the Middle Ages to support people through the process of dying.
“Actively dying can be hard work,” Harriss said. “We’re using the music as support, able to observe and discern the sense in the room.”
While there is a repertoire of music, every session is individualized to the needs of the patient and their families. Music-thanatologists react to the breath of the patient, their heart rhythms pumping through the monitors and to the emotions of those watching them go.
Metered, comfortable lullabies might give way to unmetered plain chant as the body systems fail and the vitals weaken, requiring a piece with less structure. Some sessions involved a single phrase or bars of music used repetitively. Sometimes, relatives would request a loved one’s favorite song, or need care themselves.
If family dynamics got tense as the end neared, it was Harriss’ duty to tend to their unspoken emotional needs.
“The work at that time is to work with the family before I get to grandma,” Harriss said. “They need to let go what their hopes have been.”
Harriss trained at the Chalice of Repose, a school located near Missoula, Montana. She found herself looking for a new purpose after her marriage of 30 years ended, and a friend mentioned the school. The idea captured her, and she began preparing to move from Seattle before she was even accepted.
“The letter came 10 days before school started,” Harriss said.
Harriss would spend two years training with 14 classmates, memorizing the repertoire, learning Latin and ultimately signing on as harp faculty. When she began craving life in the city again, she moved to Portland and was hired at Providence Portland Medical Center. If her beeper went off, even in the wee hours of the morning, she would take her harp in its case, go to the bedside and begin to play.
Over time, Harriss developed neuropathy in her left hand — she can no longer feel the strings underneath her fingers and plays the harp through muscle memory. Still, the music emanating from her instrument is warm and calming.
“I’m just in awe and grateful for the opportunity to have been with people this way,” Harriss said.
Arline Hinckley
Arline Hinckley believes in doctors and medicine. She also believes in the right to die.
“We have a wonderful medical care system. It can work miracles,” Hinckley said. “Unfortunately, the tendency with all of this great medical care is to continue to treat people even when it isn’t going to benefit them.”
Hinckley is a board member and volunteer with End of Life Washington, the organization that helps patients like Fuller navigate the complicated road to dying with dignity. In the book “Extreme Measures: Finding a Better Path to the End of Life” by Dr. Jessica Zitter, Zitter compares the medical community’s response to terminal illness as a “conveyor belt,” Hinckley said.
“If you are very ill and get put on a respirator, that’s one way to get on the conveyor belt,” she said. “Artificial food and hydration is another way to get on it. Aggressive chemotherapy, and that kind of thing.
“Once you get on that conveyor belt, it is hard to get off. It is hard to say, ‘This is not what I want, please let me die,’” Hinckley continued.
Her experience in an oncology department after she graduated college convinced Hinckley that people needed a legal right to get off that conveyor belt. She saw many people die, sometimes horribly — the treatment was worse than the disease, she said.
Hinckley worked to get the Death with Dignity initiative on the ballot in Washington, more than a decade after the first of such laws passed in Oregon. She helped educate people on what it meant, and found that even those who did not want to use the law themselves saw value in affording others the opportunity.
She has also assisted people through the process herself.
“People are so full of grace and bravery at that time. They’re very determined,” Hinckley said. “The medication tastes terrible and some people have difficulty swallowing it, but I’ve seen 85-year-old, 95-pound ladies just chug that stuff. They’ve made up their mind, taken care of unfinished business, mended fences, come to a spot religiously where they feel this is OK. They’re just ready.”
End of Life Washington volunteers stay after the person has fallen asleep to help family and friends with the passing. The process can be healing for the living as well — the planning of the death allows people to come to terms with it more totally than a sudden loss, she said.
“They’ve done the work. So, of course they’re sad, but in some ways they’re relieved as well because the person they love is not going to be suffering any longer,” Hinckley said.
Only eight states allow people the option to take their own lives. The most recent law passed in New Jersey in March. Organizations like End of Life Washington are working to maintain the momentum so that everyone, regardless of their location, has an option at the end.
“People deserve a choice,” Hinckley said. “It’s not a choice everyone might make, but options are important to people.”
When Robert Fuller decided to die, it was a choice informed by personal experience.
Fuller, 75, suffered from terminal cancer. He started feeling sick in July 2018. By September, a CT scan found a tumor growing under his tongue. The news didn’t surprise him.
“I knew it was there,” Fuller said in April. “I could smell it.”
It was a sour scent, he said. More basic than acidic. He could smell it clearly when he was in bed, his face pressed against his pillow.
“I wrapped my head in a pillow trying to smell it. I wasn’t attempting to do anything else,” Fuller said. His body might be failing, but his humor was intact.
Fuller considered treating the cancer medically. He started a round of chemotherapy in January, but didn’t keep it up. As a nurse to the dying, he’d watched cancers take hold despite desperate attempts to hold the disease off.
In many cases, the supposed cure was as bad as, or worse than, the disease itself, he thought.
So, Fuller worked with a medical team to get access to life-ending drugs under Washington’s Death with Dignity Act. On May 10, surrounded by family, friends and some journalists, Fuller injected the drugs into his gastric tube and fell asleep. He would not wake up.
Fuller was able to die on his terms because he found doctors willing to help him and a pharmacy willing to procure or make the medicines he needed. But that isn’t always guaranteed.
The medical community is far from settled on the question of Death with Dignity or, more generically, physician-assisted suicide (PAS). The Code of Medical Ethics, a guide provided by the American Medical Association, opposes PAS, saying that it is “fundamentally incompatible with the physician’s role as a healer.” Add onto that a growing consolidation of medical services under Catholic organizations, run under the belief that suicide is a mortal sin, and the question of assisted dying rises from an ethical debate to a religious edict.
Doctors have covertly engaged in helping their terminal patients die for decades, but access to this style of care was based on relationships and stealth, not need or as a right. As the right-to-die movement expands to new states, advocates hope that will change.
Lay of the land
Only eight states and the District of Columbia afford people the right to die with the help of their physicians. New Jersey is the most recent after the state legislature passed a law similar to Washington’s in March.
Under those laws, physicians decide if they want to help their patients through the legally prescribed process. Some hospitals ban the practice outright. Individuals question their role. As a doctor, having sworn the Hippocratic Oath to “do no harm,” could that include prescribing death?
According to the Washington State Department of Health, 115 physicians and 51 pharmacies assisted 212 terminal patients in 2017 — the last year for which numbers are available. The vast majority operate west of the Cascades. On average, only 10 percent of people who use the law live east of the mountains.
Much of that is related to access, since many of the health care facilities on the east side are associated with Catholic organizations, said Helene Starks, an associate professor of bioethics and humanities at the University of Washington who has studied assisted death for nearly 30 years.
“The fact is that the Catholic health systems are the primary providers in the state outside of the western side, and the non-Catholic organizations are more prevalent on the western side than eastern side,” Starks said.
The UW Medical system — which for these purposes primarily includes Harborview Medical Center, University of Washington Medical Center and Valley Medical Center — allows its doctors to participate in the Death with Dignity process.
Not all want to, however.
Mollie Forrester was the associate director of social work at Harborview Medical Center, and it fell largely on her team to help patients navigate the complexities of the Death with Dignity law. But, the patients weren’t the only ones who needed help.
“It has been a powerful experience to watch doctors get this request from patients,” Forrester said. “This idea of facilitating the hastened death is a process for them.”
Forrester started with the team soon after the law went into effect in 2009, on maybe the third or fourth case that the Harborview team dealt with. The idea was that their group would coordinate the implementation of Death with Dignity, and that once it was established they would farm out the work to social workers in different disciplines.
But Harborview saw so few cases that Forrester and her team ended up handling the care altogether.
It was up to Forrester to sit down with patients asking to end their own lives and explain to them the process and help them through any logistical hurdles that might arise. Their interview might be the last time she ever spoke to those patients.
“I’m walking in and saying, ‘Hi, it’s nice to meet you, let’s talk about your death,’” she said.
Doctors needed help, too. Some refused to participate, flat out. With others, Forrester felt she was performing the role of social worker.
“From where I’m sitting, it’s easy,” she would tell them. “It’s my profession, patient autonomy and patient choice.
“They’re supposed to be healing and helping people live,” she said.
The ask
Death is the inevitable conclusion of life. Fuller knew that, had known that for a long time. He joined the Hemlock Society as a young man, a group that advocated for the right to die. The Washington state society was founded in 1988 as the AIDS epidemic ravaged the gay community.
“I believed in the cause before Kevorkian,” Fuller said, referencing Dr. Jack Kevorkian, the controversial physician who helped as many as 130 people to their ends. He was nicknamed “Dr. Death” by the media and was ultimately arrested and sentenced to up to 25 years in prison for second-degree murder. He got out in eight.
Robert Fuller injects a morphine solution through his gastric tube.
The national Hemlock Society considered itself predominately educational, and when the Washington chapter wanted to assist people in their deaths, they split off to form Compassion in Dying. In 2003, Compassion in Dying was renamed End of Life Washington.
Arline Hinckley is a board member and volunteer for End of Life Washington. She and others in her organization offer advice to medical institutions and direct assistance to individuals who need help finding doctors or prescribing pharmacies. They may also be with the patients at their deaths.
“I feel like it’s a tremendous honor to be allowed in someone’s life at that very vulnerable time,” Hinckley said.
Hinckley’s second job out of graduate school in the 1970s was performing a social work role on a hematology/oncology team, caring for deeply ill patients.
“I saw a lot of people die very badly,” Hinckley said. “I was asked to help a person and I could not do that. I felt terrible, because they were suffering so greatly.”
Her experience led her to join the then-Hemlock Society.
“I have always felt that what happens to your body should be directed by you,” Hinckley said. “People deserve a choice. It’s not a choice everyone might make, but options are important to people.”
In fact, of the small number of people in Washington who use Death with Dignity in a year, as many as 30 percent never take the medications. Some got the prescription and never filled it. Others planned to, but died before they could get the medications.
The medications become almost a safety net, not because people want to die, but because that element of choice is important to them, Starks said.
“I’ve never met anybody in death with dignity who wanted to die,” Starks said. “They wanted to live a lot longer, but they also didn’t want to be a victim of their own illness.”
Even though it’s legal, it’s not easy to come by the medications that are necessary. Many people don’t know they have the option. Hospitals and pharmacies aren’t advertising that they provide these services.
In fact, a pharmacist who spoke to Real Change for this article did not want to be named at all.
“People judge you for the kind of activities that you’re doing and sometimes they equate that with good and evil,” the pharmacist said. “‘You must be evil because you’re providing this.’ Really? If you talk to this family that is suffering with this patient, that are looking for not a means to an end but an option at the end? You’re depriving them of options.”
Moving forward
The medical community is still grappling with PAS.
The issue came up before the American Medical Association in summer of 2018 and was effectively tabled rather than rejected or affirmed.
In November, the AMA’s House of Delegates deliberated a report from its Council on Ethical & Judicial Affairs (CEJA) that looked into the legal and ethical ramifications of PAS. The existing guidance in the Code of Medical Ethics remained unchanged, but delegates also voted to take the matter up at a future policy-making meeting.
Attitudes are changing. More than two-thirds of Americans believe that doctors should be allowed to help terminally ill patients who are in pain to die, according to a 2015 Gallup poll. Young adults were particularly supportive with 84 percent of people between 18 and 34 on board with the concept.
For some, the act is still seen as suicide. Robert Fuller believed differently.
“It’s taking responsibility for the rest of my life,” Fuller said.
For the last hours of his 75 years on Earth, Robert Fuller was married to a man who he loved.
“I anoint you,” said Nancy Rebecca, a nurse, clairvoyant and sometime wedding officiant, “Mr. Robert and Mr. Reese Baxter-Fuller.”
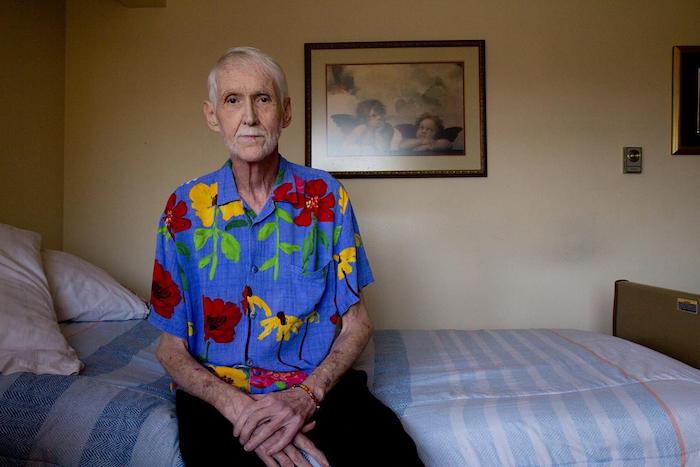
The cameras flashed, the tape rolled as Fuller and Reese Baxter exchanged vows, rings and a chaste kiss. It was a simple wedding. The couple sat on the couch in their shared apartment in Primeau Place, a senior housing building on Capitol Hill. Baxter wore a black and white sweater, Fuller a relatively restrained Hawaiian shirt with large, colorful flowers against a cerulean background, ready for the party that waited for the newlyweds downstairs. The ceremony commenced at 10:30 a.m. By evening, Robert Fuller would be dead.
The cancer was slowly choking him
Robert Fuller planned every detail of his death. He knew who he wanted to see — invites had gone out weeks before — and what music he wanted to play him out. He’d also planned the food, although he himself couldn’t eat it.
Fuller was dying of a virulent strain of cancer, a disease that lodged itself in his throat and, over the course of a year, was slowly choking the life from him. At the end of March, he already had significant difficulty swallowing, leaving most of his meals to be transmitted through the gastric tube installed in his stomach, hidden by clothes that hung on his tall, wasted frame.
A nurse by training, Fuller knew what the future held if he decided to wage chemical war against his opponent.
“I’ve taken care of patients like me,” Fuller said, sitting in his recliner, staring out his window at a view of the sunlit Puget Sound. “I have a friend whose father died of the same thing 50 years ago. He did pursue all of it, all of the radiation. I only did a little bit of it. He did it all and it was a horrible death.”
That slow, painful, fruitless fight was not how Fuller wanted to spend his final days. He wanted to die as he lived — on his terms. He turned to Death with Dignity.
Robert Baxter-Fuller sits on his bed in blue pajamas. The clock, above, ticked down the minutes until 3 p.m. when Fuller would ingest his life-ending medications.
A public death Death with Dignity began as an initiative passed by Washington voters in 2008. It allows terminal patients to end their lives by ingesting toxic amounts of drugs rather than suffer in their final months, weeks or days. They ease into sleep and never wake up.
Fuller became aware of it when a woman from California moved into the senior housing building in which he lived and helped manage.
“Wendy was her name,” Fuller recalled. “She started telling me about it pretty quickly, because that’s what people do when they meet me. Strangers tell me everything. On the bus, I don’t care where. They confess to me, they tell me their worst medical problems. They do. It just happens.”
Wendy moved to Washington to kill herself. It was one of the few states that allowed it. Although California would follow suit in 2016, Wendy didn’t have that long.
On the day she was to die, Wendy had a sign put on her door that read “Do Not Disturb.” When it came down, she was gone.
“I said, ‘Woah,’” Fuller said. “That solidified it for me. That’s what I’m going to do.
“But,” he continued, his voice hushed into a conspiratorial whisper, “mine is not going to be private. That is not the way I lived my life.”
Sharing stories, saying goodbye
Everybody seemed to call it something different. “Death Day.” “The Day.” Fuller didn’t care. When he spoke of it, he generally just referred to it as May 10.
“I’ll see you on May 10,” he told visitors in the days leading up to the event.
A gaggle of brightly colored helium balloons marked the entrance to Primeau Place’s common room, an open space lit harshly with fluorescent light. A piano stood against the eastern wall, a drumset assembled beside for the occasion.
People flooded the space, spilling out into the small patio that was sheltered from the spring sun by large trees. They munched on hors d’oeuvres, laughed and shared stories of Uncle Bob, as most people called him.
All the while, Fuller held court, seated next to his new husband as his guests came, one by one, to say their final goodbyes. He held a walking stick sanded down and polished into a smooth, golden surface and carved with tight grooves.
Someone he had sponsored made it for him while still using crack, Fuller had said more than a month before.
“I think that’s significant,” he said. “For people who are still into drugs and think nothing positive can still come out of this.”
That depth of compassion, of acceptance and understanding drew people to Fuller. He’d sponsored many in the room through the Alcoholics Anonymous program. He spent 10 years as a nurse in King County jail. He was an active member of St. Therese Catholic Church. He arranged for Primeau Place to “Adopt-A-Drain” outside the building to give back in another way.
Fuller was many things, said Scott Farrell, who had met Fuller at a spiritual retreat for gays and lesbians more than 40 years prior.
“He was always there for me,” Farrell said. “He was a light in my life. We haven’t been in touch a lot lately, but whenever I see him, it feels like there is no time.”
Nicholas Bross was one of the people Fuller sponsored. He was dressed in a Hawaiian shirt, a gift from Fuller specially for his big day.
“I’m supportive of his choice, his decision to do this,” Bross said. “I’ve been telling people that if I were in his shoes, I’d be doing the same thing.”
It took time for some to accept what he wanted to do, Fuller said. Most made their peace with it after the initial shock. Fuller gave them the space to process on their own terms. They might not be ready, but Fuller was. He had been for decades.
A partygoer leans over to speak to Robert Baxter-Fuller.
Escaping death during the AIDS epidemic
It was 1985. Fuller was living in Chelan, Washington, a handsome young man in his early 40s playing Schroeder, the philosophical musician, in a local production of “You’re A Good Man, Charlie Brown.”
He stopped paging through an old album and touched a photograph of his younger self with a frail finger. In the moment, a dapper Fuller was standing on stage with a seated woman playing a smitten Lucy.
“I have HIV in this picture, but I don’t know it,” Fuller said.
He had moved to Chelan to get away from the death he saw ravaging the gay community in Seattle. Fuller, a recovering alcoholic, watched as two or three young men a week disappeared from his Alcoholics Anonymous meetings.
“It just kept going, so I moved to Chelan,” he said. “There were no gay people and no AIDS, I told myself.”
He’d already taken the test by the time he appeared in that musical. The results would come back negative, but in his bones, he knew they were wrong.
That was when Fuller began packing his bags.
That was the phrase his community used to describe planning for their own deaths. Getting your living will in order, designating a power of attorney, making arrangements for your loved ones.
In the 1980s and 1990s, HIV could be a death sentence. Fuller stood by the sides of two men who he loved as they died. Chet, a swarthy man seated next to Fuller as the pair stare out over a lake, would be reduced to skin and bones in a matter of months. Bill, whom Fuller thought of as his first husband, although they could not legally wed, also died. Tom, an artist who Fuller described as a Jesus figure, appeared in a picture with Fuller at Chet’s funeral.
He would be dead a year later.
At the height of the epidemic, Fuller “packed his bags” every six months to a year. His viral load soared to 700,000 and his T-cell count dropped to 76, laying his body open to infection and possibly death. But he survived until the cocktail of drugs created in the late 1990s hit the market. He resisted the previous medications — those cures also killed.
Until his death, Fuller’s viral load was undetectable, but he carried the symptoms of HIV on his body. When he walked, he would pick up his feet like they were on marionette strings and plant them slowly and carefully on the carpet. It was called peripheral neuropathy, he said, lapsing into the assured cadences of a health care professional.
The loss of proprioception that comes with peripheral neuropathy brought Reese Baxter into his life. Baxter needed a place to stay, Fuller needed someone to help him — he’d fallen many times and struck his head.
“I didn’t know it would be three years,” Fuller said.
How to die with dignity
Dying seems easy. After all, we spend so much time and energy avoiding it.
Dying with dignity? That takes work.
Robert Baxter-Fuller prepares a mixture of morphine and CBD oil to ease his pain.
First, you have to find a doctor willing to let you die. The law doesn’t mandate that doctors participate in Death with Dignity, it only says that they can. Many won’t, for personal reasons. Others can’t because they are forbidden to do so by their employers.
Hospitals that belong to the University of Washington medical network opt in, said Professor Helene Starks, an expert in medical ethics who has been studying end-of-life issues for three decades.
“I think that the general feeling is as a public institution enacting a public law, there was an obligation to provide access,” Starks said.
Swedish Medical Center, in contrast, is affiliated with Providence Health & Services, a Catholic nonprofit organization founded by the Sisters of Providence in 1856. The Swedish Medical Center in Seattle does not forbid its employees from engaging in Death with Dignity, according to a position statement issued after the law passed, although some Catholic-affiliated hospitals do.
This partly explains why as much as 90 percent of people in Washington who use the act do so west of the Cascades — access is extremely limited in the eastern portion of the state.
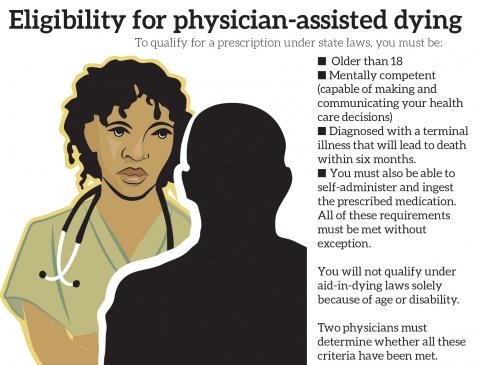
Fuller was able to receive care at Harborview Medical Center. First, he had to make an oral request. The doctor evaluated him to make sure that he was of sound mind — people with dementia cannot use Death with Dignity. It takes two doctors, one attending and one consulting, to complete the process.
No less than 15 days later, you have to make a second oral request. Fuller’s doctor accidentally scheduled his follow-up 14 days after the initial appointment. He had to come back the next day.
Once a person has jumped through these hoops and gets the prescription for the drug, they must find a pharmacy willing to fill it. This gets complicated, because pharmacists, like doctors, do not have to fill the script if they are opposed to the practice and some don’t have the expertise.
If you can find one — and there are a few in the area — the pharmacy has to be able to access the drugs.
Secobarbital — marketed under the name Seconal — is the preferred option. Called “reds” back in the day, secobarbital was used as a sleep aid until the danger of overdosing and negative interactions with alcohol became apparent.
Bausch Health, formerly Valeant Pharmaceuticals, bought the patent for the drug when it expired. Although the chemical makeup of the drug hasn’t changed in 80 years, the price did. When California passed its End of Life Option Act in 2015, the price of the drug doubled, according to NPR.
Today, the 100 capsules needed to end Fuller’s life would have cost him more than $3,000 without insurance.
Medical professionals created a cheaper cocktail of four drugs that cost roughly $400, but that is where the expertise comes in. A generic pharmacy can’t make the cocktail, but a compounding pharmacy can.
In the end, Fuller would use the cocktail — his pharmacy was not able to get the necessary amount of secobarbital.
The whole process takes weeks if not months for people who, by law, must have a six-month prognosis.
“You have to adhere to a strict process,” Fuller said. “You don’t just walk in and say, ‘I want to get rid of Grandma. I hear you have death panels.’”
Final act
As the clock ticked closer to 3 p.m., the mood at the party changed.
The jovial atmosphere gave way to the weight of the moment as the minute hand ticked by, moving inexorably closer to the time of Fuller’s death.
Robert and Reese Baxter-Fuller look at each other as people say their last goodbyes to Robert.
He went upstairs, his husband on one side, his walking stick on the other. There were balloons outside his apartment door as well, framing a nametag attached to the name plate that read “Uncle Bob.”
Bodies pressed into the small apartment, filling the T-shaped corridor that led from the front door to Fuller’s room on the left and the living room on the right. Fuller went into his room with a select few — he changed into a ocean-blue set of shiny pajamas, the “Hugh Hefner” pajamas, as he liked to call them.
He lay there, his twin bed strewn with pink rose petals, Baxter at his side, holding his hand.
In March, Fuller said that Baxter would hold his hand in a “fishhook,” a wrestling grip that is next to impossible to break until one of the parties lets go.
“He’s now the person whose hand I want to be holding when I die,” Fuller said. “He’s going to give me the cue when I’m falling asleep, or when I seem to be sleeping, that I can leave.”
When the doors opened, Fuller’s friends, adopted family and loved ones shuffled into the room until there was no space left. People squeezed into every nook and cranny, shoved into a closet, trying to use a flimsy clothing basket for support.
By law, Fuller had to ingest the drugs on his own. Many choke it down — the taste is terrible, bitter. He took a syringe and injected the poisonous cocktail into his gastric tube.
Almost a third of people who get the prescriptions never take it. Not Fuller. Now, he would die.
Baxter gripped Fuller’s hand, the other holding an electric pink towel he used to absorb his tears. A violinist put bow to strings, playing Amazing Grace and Ave Maria. As Fuller’s eyes closed and his body went still, the observers raised their voices in song. Those closest to him placed their hands on his body in farewell.
Robert Baxter-Fuller eases into a final sleep.
Technically, he was asleep. Death would come later, after the drugs wrested his final breath away from the cancer that tried to steal it. But Bob Fuller was gone.