[W]hen my father was dying of pancreatic cancer last summer, I often curled up with him in the adjustable hospital bed set up in his bedroom. As we watched episodes of “The Great British Baking Show,” I’d think about all the things I couldn’t promise him.
I couldn’t promise that the book he’d been working on would ever be published. I couldn’t promise he would get to see his childhood friends from England one more time. I couldn’t even promise he’d find out who won the baking show that season.
But what I could promise — or I thought I could — was that he would not be in pain at the end of his life.
That’s because after hearing for years about the unnecessary medicalization of most hospital deaths, I had called an in-home hospice agency to usher him “off this mortal coil,” as my literary father still liked to say at 83.
When a doctor said my father had about six months to live, I invited a hospice representative to my parents’ kitchen table. She went over their Medicare-funded services, including weekly check-ins from a nurse and 24/7 emergency oversight by a doctor. Most comfortingly, she told us if a final “crisis” came, such as severe pain or agitation, a registered nurse would stay in his room around the clock to treat him.
For several months, things went well. His primary nurse, who doubled as case worker, was kind and empathetic. A caretaker came three mornings a week to wash him and make breakfast. A physician assistant prescribed drugs for pain and constipation. His pain was not terrible, so a low dose of oxycodone — the only painkiller they gave us — seemed to suffice.
In those last precious weeks at home, we had tender conversations, looked over photographs from his childhood, talked about his grandchildren’s future.
But at the very end, confronted by a sudden deterioration in my father’s condition, hospice did not fulfill its promise to my family — not for lack of good intentions but for lack of staff and foresight.
At 7 p.m. on the night before my father’s last day of life, his abdominal pain spiked. Since his nurse turned off her phone at 5, I called the hospice switchboard. To my surprise, no doctor was available, and it took the receptionist an hour to reach a nurse by phone. She told us we should double his dose of oxycodone, but that made no difference. We needed a house call.
The only on-call nurse was helping another family two hours away. So my sister and I experimented with Ativan and more oxycodone, then fumbled through administering a dose of morphine that my mother found in a cabinet, left over from a past hospital visit. That was lucky, because when the nurse arrived at midnight, she brought no painkillers.
After the nurse left, my father’s pain broke through the morphine. I called the switchboard again, and it took three hours for a new nurse to come. She was surprised he hadn’t been set up with a pump for a more effective painkiller. She agreed that this constituted a crisis and should trigger the promised round-the-clock care. She made a phone call and told us the crisis nurse would arrive by 8 a.m.
The nurse did not come at 8 a.m. Or 9 a.m. When his case worker was back on duty, she told us — apologetically — that the nurse on that shift had come down with strep throat. Her supervisor stopped by, showed us the proper way to deliver morphine (we’d been doing it wrong) and told us a pain pump and a crisis nurse should arrive by noon.
Noon passed, then 1 p.m., 2 p.m. No nurse, no pump.
By this time, my father had slipped into a coma without our noticing; we were thankful his pain was over but heartbroken he wouldn’t hear our goodbyes. Finally, at 4 p.m., the nurse arrived — a kind, energetic woman from Poland. But there was little left to do. My father died an hour later.
At the end of life, things can fall apart quickly, and neither medical specialist nor hospice worker can guarantee a painless exit. But we were told a palliative expert would be at my father’s bedside if he needed it. We were not told this was conditional on staffing levels.
I didn’t realize how common our experience was until a few months after his death, when two reports on home hospice came out — one from Politico and one from Kaiser Health News. According to their investigations, the hospice system, which began idealistically in the 1970s, is stretched thin and falling short of its original mission.
Many of the more than 4,000 Medicare-certified hospice agencies in the United States exist within larger health care or corporate systems, which are often under pressure to keep profit margins up.
Kaiser Health News discovered there had been 3,200 complaints against hospice agencies across the country in the past five years. Few led to any recourse. In a Medicare-sponsored survey, fewer than 80 percent of people reported “getting timely care” from hospice providers, and only 75 percent reported “getting help for symptoms.”
I called Edo Banach, the president of the National Hospice and Palliative Care Organization, to get the trade group’s response. He expressed sympathy for my father’s suffering but was adamant that good hospice experiences “far outweigh” the negative ones.
Granted, more than a million Medicare patients go into hospice care every year, so the complaints are in the minority. Mr. Banach told me he’s worried that drawing attention to what he called the “salacious” stories of failed hospice care means more families will turn to less holistic, less humane end-of-life care. That could be true. But then, should there be more transparency early on? Should the hospice reps explain that in most cases, someone will rush to your loved one’s side in a crisis, but sometimes the agency just doesn’t get the timing and the logistics right?
As the number of for-profit hospice providers grows, does that model provide too great an incentive to understaff nighttime and weekend shifts? The solution may have to come from consumer advocacy and better regulation from Medicare itself.
A new government-sponsored website called Hospice Compare will soon include ratings of different agencies, which will ideally inspire some to raise their game. When I looked up the agency we had used, its customer satisfaction rate for handling pain — based on the company’s self-assessment — was 56 percent.
I considered making a complaint in the days after my dad’s death, but frankly we were just too sad. Even now, I believe hospice is a better option than a sterile hospital death under the impersonal watch of shift nurses we’d only just met. But I wonder whether that hospital oversight might have eased my father’s pain earlier on that last day.
Ultimately, even without pain relief, he was probably more comfortable in his own home, tended by his children, doing our best.
Barry Hyman always swore he’d die peacefully on his own terms. But living in a faith-based nursing home put his family in a difficult position to help him
Lola Hyman and her son Jackson look over photographs of Lola’s father Barry Hyman at their home in Vancouver.
[O]n the night that 83-year-old Barry Hyman was to receive a doctor-assisted death, his daughters were on edge, petrified that at any moment someone would burst through the door and stop them from granting their father his final wish.
Enfeebled by a stroke and diagnosed with lung cancer, Mr. Hyman had asked to die at home.
But his home at the time was a publicly funded Jewish nursing home in Vancouver whose board forbade assisted deaths on site, saying the newly legal practice violated the values and traditions of the Jewish faith.
That left Lola Hyman, the younger of Mr. Hyman’s two daughters and his main caregiver, with a choice.
She could transfer her father to an unfamiliar clinic to die, or she could sneak Ellen Wiebe, one of the country’s leading doctor-advocates of assisted dying, into her father’s room to help him die in his own bed.
Lola and the rest of her immediate family settled on the latter. They would deal with the fallout later.
Their first priority was making sure that Mr. Hyman died peacefully on his own terms, as he’d always sworn he would.
“The room was very quiet. We just held his hand and stared at him,” Lola said. “My sister was sobbing, just sobbing. I was a stone. A complete stone. My heart was racing that someone would open the door.”
nstead of focusing on their goodbyes, the Hyman family spent the last moments of Barry’s life worrying that they would be discovered and prevented from completing a legal medical procedure inside a publicly funded care facility.
Their story is an extreme example of the choices that grievously ill Canadians still face – 18 months after Ottawa’s assisted-dying law took effect – if they wind up near the end of their lives in a hospital or nursing home that refuses to allow assisted dying, either for religious reasons, or because the facility has simply decided to say no.
It is not clear if these institutions enjoy the same Charter-protected religious freedoms as individuals when it comes to refusing assisted deaths because the issue has not yet been tested in court.
In the vast majority of cases, such patients are transferred to another facility to die. But it isn’t always easy to find a place to send them.
Sometimes overcrowded secular hospitals say no. Sometimes the only hospital or nursing home in town is faith-based.
Other times, an unconventional location has to suffice: In Vancouver, Dr. Wiebe has opened her women’s health clinic after-hours for 34 assisted deaths, which means that in some cases, Catholic health-care facilities have transferred patients to an abortion clinic to die.
Canada’s religious health-care organizations, which have been tending to the sick in this country since long before Medicare, say they are doing their best to support terminally ill patients without betraying their own faith, offering options like palliative sedation to make patients’ natural deaths as painless as possible.
Some have softened their objections to the early parts of the medical-aid-in-dying process, allowing outside doctors to come in and conduct eligibility assessments on patients who are too fragile to be transferred for an appointment.
But when it comes to actual physician-assisted deaths, religious facilities – be they Jewish, Baptist, Catholic or otherwise – are refusing to allow the practice on their grounds.
“The core issue … is that Catholic and faith-based organizations are committed to the inherent dignity of every human life and would never intentionally hasten the end of a life,” said Christopher De Bono, vice-president of mission, ethics, spirituality and indigenous wellness at Providence Health Care, a Catholic health-care network that includes St. Paul’s Hospital in downtown Vancouver.
Nobody on either side of Canada’s assisted-dying divide is arguing that individual doctors or nurses should have to participate in assisted dying if they object to it, said Shanaaz Gokool, the chief executive officer of the advocacy group Dying with Dignity Canada.
But she is incensed that every province with faith-based health-care organizations except Quebec has allowed taxpayer-funded hospitals and nursing homes to refuse requests for a procedure the Supreme Court of Canada has declared a Charter-protected right. (And even Quebec allows some hospices to opt out.)
“Why are we making this so hard for people when it’s the one medical treatment that you have a legal right to in this country?” she said.
Throughout Barry Hyman’s long and colourful life – through founding a small publishing company, raising two daughters, divorcing twice, studying history and English literature at Simon Fraser University as a senior citizen and logging countless hours at casino poker tables – he told anyone who would listen that he had no desire to linger if his health failed.
“Ever since I can remember, and I mean over 50 years, my father has always told me that if he ever got to the point that he no longer had the ability to comprehend, the ability to socialize, the ability to do the things that he wanted to do … he was done,” said Leah Hyman, 54, Mr. Hyman’s eldest daughter.
Mr. Hyman, a Winnipeg-born businessman, dreaded one day losing the vitality that infused his life, first as a young waiter on the railroad, then as the founder of an Edmonton printing company that churned out small Jewish newspapers and government directories.
He also owned pool halls, nightclubs and a roller rink. He was still on J-date, the online Jewish matchmaking service, in his 80s.
“He just rolled up his sleeves and dove into everything,” Lola said – including introducing his only grandson, Jackson Doyle-Hyman, now 19, to the worlds of business and (responsible) gambling.
Mr. Hyman once took a kindergarten-aged Jackson to the track and showed him how to bet $10 at a time on the top horses.
Lola, now 51, later found cash spilling out of the pockets of Jackson’s little navy polo jacket.
As he grew older, Jackson often tagged along to business meetings where ad space was traded for car parts or hotel stays, a practice called “contra.”
Barry Hyman holds his grandson, Jackson, in 1998.
“We always joked that he could have built a Ferrari with all the car parts he got contra for,” Jackson said.
Mr. Hyman was already a diabetic with congestive heart failure when he was diagnosed with lung cancer early in 2016.
But his health didn’t really begin to deteriorate until an ill-fated trip to a tanning salon to treat his psoriasis.
The tanning bed left Mr. Hyman with a burn on his left foot no bigger than a quarter. The wound festered for nearly a year, despite every effort to heal it.
By October of 2016, doctors were talking about amputating his leg. Mr. Hyman instead chose to undergo a procedure in which surgeons bypassed a clogged leg artery that was keeping his foot from healing.
Ten days later he had a stroke, a known risk of the operation.
His mind was still sharp, but the stroke impaired his speech – a devastating blow for a man who adored the English language and insisted upon its correct use.
“This was a guy who read two papers a day and did the New York Times crossword,” Lola said, “And he no longer could do any of that.”
It was clear to Lola that her father could not keep living in his own apartment, as he had before the stroke.
The family’s first choice was the Louis Brier Home and Hospital, Vancouver’s only Jewish nursing home. But it was full.
Mr. Hyman during a portaging trip through the Northwest Territories in 1985.
Reluctantly, Mr. Hyman accepted a spot at St. Vincent’s: Brock Fahrni, a Catholic home where he shared a room with three other men.
Mr. Hyman and his family made a preliminary inquiry about assisted death with a doctor there, but it went nowhere.
When, in April of 2017, a bed in a private room became available at the Louis Brier Home, Lola leaped at the chance.
She knew that, like the Catholic home her father would be leaving, the Louis Brier did not permit assisted deaths on site.
She hoped that moving her father to a nicer place where he could live among his Jewish peers and Jewish culture would persuade him to abandon his talk of assisted death.
But Mr. Hyman wouldn’t let go of the idea. Although Lola didn’t want to lose her father, she was willing to help him fulfill his final wish.
On April 26, a week after moving to the Louis Brier, Mr. Hyman and Lola met Dr. Wiebe at her office.
A few hours later, Dr. Wiebe e-mailed Lola to say her father’s constellation of health problems made him eligible for an assisted death.
Dr. Ellen Wiebe sits in the room where she helps those wanting medically assisted deaths at the Willow Women’s Clinic in Vancouver.
When the Supreme Court of Canada struck down the Criminal Code prohibition on physician-assisted dying in February of 2015, the judgment made it clear that invalidating the law would not compel doctors to help their patients die.
The court was silent, however, on whether entire health-care organizations could bow out of medical aid in dying.
Parliament passed a law that was silent on the question, too, even though a special joint committee of the House and Senate had recommended that Ottawa work with the provinces to ensure all publicly funded health-care facilities provide medical assistance in dying.
Jay Aubrey, a lawyer with the British Columbia Civil Liberties Association, the group that helped topple the ban on assisted dying, predicted that a legal challenge against an objecting religious health-care facility such as the Louis Brier Home would be straightforward.
The home is 67-per-cent publicly funded and is therefore “acting in the shoes of government,” she said. “That’s why they’re bound by the Constitution.”
Ms. Aubrey sent a letter to the Louis Brier Home last May making that case on Mr. Hyman’s behalf.
But Richard Moon, a University of Windsor law professor and an expert in religious-freedom cases, said past precedents suggest public funding alone is not enough to saddle a third-party like a nursing-home operator with the constitutional duties of a government.
On the contrary, he said, religious health-care organizations could try – and might succeed, under the right circumstances – to claim they are entitled to the same Charter-protected religious freedoms as individuals, allowing them to rebuff government orders that breach their beliefs.
Prof. Moon said there could be a simple way around that: Provincial governments could withhold funding from health-care organizations that do not allow assisted dying, so long as they applied the rule without discrimination.
“It’s a matter of nerve here, isn’t it?” he said. “Is the government really willing to withdraw funding from these organizations? Are these organizations really willing to risk the loss of funding?”
So far, everywhere outside Quebec, the answer is no.
Grievously ill patients are instead being transferred out of non-participating institutions in numbers that are difficult to determine at a national level.
British Columbia’s five regional health authorities together logged a total of 61 transfers as of the beginning of December. Alberta has recorded 42; Saskatchewan is aware of at least 11; Manitoba has recorded eight.
The Maritime provinces say they are either not aware of any such transfers or are not tracking them.
The outlier is Ontario. Not only has Kathleen Wynne’s government declined to track transfers, it passed a law exempting hospitals, nursing homes and hospices from freedom-of-information requests about medical aid in dying, a move the province’s privacy commissioner denounced.
The blackout, which a spokesman for Ontario’s Ministry of Health and Long-Term Care said was enacted to protect health-care workers and institutions that provide assisted dying, makes it impossible to say how many hospitals in Canada’s most populous province are refusing to allow the practice.
But ministry officials have hazarded a guess: As many as 27 publicly funded Ontario hospitals – one out of every five in the province – would “potentially object to [medical aid in dying] based on their stated religious/ideological values,” according to an internal briefing note that Dying with Dignity obtained through a freedom-of-information request.
“There are 7 cities/towns in Ontario with potentially objecting hospitals that have no alternative hospitals within 100 km. Moreover, there are 4 other cities/towns with only one neutral hospital for the whole region.”
In Vancouver, when patients are looking for an alternative location to receive an assisted death, one option is Dr. Wiebe’s Willow Women’s Clinic on the 10th floor of a downtown high-rise.
The space has much to recommend it, according to Dr. Wiebe: wheelchair access, a separate waiting room for family and, in the larger of the two rooms she reconfigures for assisted deaths, a spectacular view of the mountains.
Still, there’s a makeshift feel to the arrangement. Patients take their last breaths on a bedsheet-draped patio recliner, the same piece of furniture on which the clinic’s regular clients recover after having an intrauterine device inserted.
In one “dreadful” case, a man who wanted to die without his family present was transferred from a Catholic facility and mistakenly left outside by a medical transportation service, next to the pounding of jackhammers, Dr. Wiebe said.
“We need to get to [the government] and say, ‘This is completely unreasonable – you can change it with the stroke of a pen,'” Dr. Wiebe said of the B.C. NDP’s decision to continue allowing publicly funded faith-based institutions to opt out of assisted dying.
B.C. Health Minister Adrian Dix declined an interview request for this story.
A spokeswoman for the Ministry of Health emphasized that all of the regional health authorities in B.C. have care co-ordination services that help smooth the transition for patients who have to move from one place to another for an assisted death.
She said the provincial government has “no plans to terminate” a long-standing agreement that allows members of a group called the Denominational Health Association (DHA) to refuse to provide services that are inconsistent with their religious values.
The DHA represents 44 health-care facilities in B.C., including the Louis Brier Home, where Barry Hyman wanted to die.
The entrance to the Jewish faith-based Louis Brier Home and Hospital in Vancouver.
A few weeks after meeting Dr. Wiebe, Lola Hyman e-mailed David Keselman, the chief executive officer of the Louis Brier Home, to formally ask that her father be allowed to die on site, despite the home’s policy.
Mr. Keselman sent his formal reply to Lola on May 25. “Quite some time ago,” he wrote, “the governing board, along with the leadership of Louis Brier, decided that Louis Brier will provide care and services to the residents according to the Orthodox Jewish stream.”
The home was willing to allow eligibility assessments, he continued, but not assisted death itself.
“Lola I realize that this may not be what you would have liked or have wanted to hear,” Mr. Keselman wrote. “If so I regret this.”
For weeks afterward, Lola weighed her options. She didn’t like the idea of sending her father to die at Dr. Wiebe’s office or an unfamiliar seniors’ home suggested by the care co-ordination service at Vancouver Coastal Health.
“The thought of doing my father’s provision in a clinical setting [with a bed] that looked like a dentist’s chair was so unsettling for me,” she said. “I didn’t share it with my father. I did not burden him with any of the logistics. I just said, ‘When you want it to happen, Dad, it will happen.'”
Mr. Hyman ultimately decided to die on June 29.
Leah and her wife, Tori, drove up from their home in Oregon that day to be with Lola and Jackson in Mr. Hyman’s room.
Early in the evening, Lola went to the front door of the nursing home to welcome Dr. Wiebe and a nurse as though they were old friends paying a visit.
They hid their medical equipment and lethal drugs in oversized bags.
Dr. Wiebe, her nurse and Lola went in to Mr. Hyman’s room and shut the door. Leah, Tori and Jackson stood guard outside.
When a nurse from the home came by to try to give Mr. Hyman his regular medications, Leah offered to deliver the pills, shooing the nurse away with a forced joke or two as though she were not minutes away from watching her father die.
“It was rough,” she recalled, crying. “I was not the best daughter. We just didn’t communicate well. We loved each other and we knew each other and we were there for each other. But this was the one thing I was going to make sure that we did, that we followed through on. He was going to go the way that he wanted to go.”
When Dr. Wiebe was ready to begin injecting the medications, Leah, Tori and Jackson came in and joined Lola at Mr. Hyman’s bedside.
He died peacefully in about 10 minutes that felt much longer to his family. “I’ll never forget looking at the door all the time,” Leah said, “terrified that someone was going to come in.”
In the end, nobody interrupted Mr. Hyman’s death. Dr. Wiebe filled out the death certificate, gave it to Lola, and left.
About 20 minutes later, Lola approached the home’s nursing station and did something she instantly regretted: She told them her father had died, but didn’t say how.
“I was frozen,” she said. “If I could go back, I would have walked up to that nursing station and said, ‘Dad passed of [medical aid in dying],’ but I can’t imagine what I would have been bombarded with as Dr. Wiebe was getting into her car.”
The next morning, after Dr. Wiebe reported the details of the case to Vancouver Coastal Health, Lola sent the Louis Brier Home a copy of Mr. Hyman’s death certificate.
The aftermath of Mr. Hyman’s death was hard on the home’s staff, especially the front-line workers who were initially puzzled by his unexpected death, Mr. Keselman said.
“We had no opportunity to communicate with the staff, to prepare them, to explain anything,” he said. “It was very traumatic.”
Mark Rozenberg, the chair of the ethics committee of Louis Brier’s board, emphasized that the home makes no secret of its opposition to assisted dying.
“Anyone who comes here knows what our policy is,” he said. “And if they don’t like the policy, they should go somewhere else.”
The home has since filed a formal complaint against Dr. Wiebe with the College of Physicians and Surgeons of British Columbia, the regulator for doctors in the province.
The complaint does not faze Dr. Wiebe; she is confident the college will see she was fulfilling her patient’s wish to die at home. (A college spokeswoman declined to comment.)
But Lola is heartsick at the thought of Dr. Wiebe in trouble, just as she is heartsick about having upset the front-line staff at Louis Brier.
None of this – including the stress her family experienced on the evening of Mr. Hyman’s death – would have happened if the government compelled all publicly funded health-care facilities to allow assisted dying, Lola said.
“Everyone is entitled to their religious beliefs and traditions and customs,” she said. “But when it comes to somebody who is very sick and dying, we need to have a different approach.”
[D]ecisions about diabetes care can become harder as people age, and that may be especially true for those needing hospice care.
A new study has found that, among people getting hospice care in a nursing home, diabetes care may lead to higher rates of dangerous low blood sugar episodes, known as hypoglycemia.
That finding came from the researchers’ analysis of data on nearly 20,000 people with type 2 diabetes, all in nursing homes and receiving hospice care.
In 180 days, the time period covered by the study, about one in nine people experienced low blood sugar episodes. But, among those treated with insulin, about one in three had low blood sugar episodes, according to the study’s lead author, Dr. Laura Petrillo, an instructor in medicine at Harvard Medical School.
Low blood sugar can cause weakness, sweating, confusion, shakiness and dizziness, which can cause suffering and reduced quality of life. The researchers defined low blood sugar episodes as blood sugar levels under 70 milligrams per deciliter (mg/dL).
“Hospice is care focused on maximizing comfort at the end-of-life, and usually includes stopping treatments that are unlikely to have short-term benefits,” Petrillo said. “Patients with type 2 diabetes were experiencing hypoglycemia, which would be an indication that there was room for improvement in their diabetes care.”
The study also looked at high blood sugar episodes, defined as blood sugar levels over 400 mg/dL. High blood sugar — hyperglycemia — can cause excessive thirst and a need to urinate more frequently. During the 180 days, 38 percent of patients treated with insulin had low blood sugar, 18 percent had severe low blood sugar and 35 percent had high blood sugar.
Blood sugar levels were checked an average of 1.7 times a day for people on insulin and 0.6 times a day for those who weren’t given insulin, according to the report.
People in the study were receiving end-of-life care at Veterans Affairs nursing homes between 2006 and 2015. All were 65 or older, and nearly all — 98 percent — were men. About 83 percent died before 100 days.
The study findings bring up an important issue — the need for more specific guidelines for diabetes management in nursing home and hospice patients, according to Dr. Joel Zonszein, director of the Clinical Diabetes Center at Montefiore Medical Center in New York City.
Those institutions often “export guidelines for hospitalized patients, and end up continuing to use a lot of medications that cause hypoglycemia,” he said.
Zonszein noted that insulin isn’t the only medication that can cause low blood sugar levels. Some oral diabetes medications also can cause blood sugar levels to drop too low.
In addition to causing people to feel terrible, low blood sugar levels can also increase the likelihood of falls — a concern in hospice facilities and in nursing homes, he explained.
“If medications are not improving quality of life in hospice, it doesn’t make sense to use them,” Zonszein said. “There are many newer medications that don’t cause lows and control the highs. They cost more, but you don’t have to monitor patients as much,” so ultimately they’re likely cost-saving, he suggested.
Matt Petersen, managing director of medical information for the American Diabetes Association, said that the study adds to the understanding of end-of-life care for people with diabetes.
“Hypoglycemia is to be avoided for safety and quality of life, but severe hyperglycemia is also to be avoided for the same reasons — left to go too high, glucose levels can lead to catastrophic (and very unpleasant) metabolic crisis,” Petersen said. “In patients that may not be eating well, estimating insulin dosing to match food intake can be challenging.”
Petersen said it appears from the information provided that patients in the study were receiving individualized care based on their health condition, which is what the American Diabetes Association recommends for care.
“Care should involve a comprehensive consideration of what will ensure the best circumstances for the patient,” he noted.
The study authors pointed out that about one-quarter of people in the United States die in a nursing home, making this a problem many people might face.
What, then, can people do to ensure they or a loved one receives the right care for them in a nursing home, particularly as they near the end-of-life?
“Advocate for your loved ones,” Petrillo advised. “Ask for a medication review, and make sure that medications are geared toward providing comfort and that they’re not receiving anything that doesn’t have a short-term benefit.”
The study was published as a research letter in the Dec. 26 online edition of JAMA Internal Medicine.
In the season of giving, hospice grants patients’ end-of-life wishes
From left, Deborah Holmes, Leslie White and Lisa Price work with patients of all ages at Seasons Hospice. Their job is to provide comfort and love to a person in his or her last days, weeks and even months.
[D]eborah Holmes adjusted her glasses, eyes watering as she glanced up at the ceiling of Seasons Hospice’s family room.
“I’m glad I didn’t wear mascara again today, though none of us [nurses] do much because we cry so often,” she said, smiling as her voice cracked. “I’ve almost given up wearing glasses they fog up so much too.”
Steadying her voice, Holmes laughed — a mixture of sadness, humor and joy.
Though the holiday season is often thought of as an especially important time for giving and making wishes come true, for Holmes and her fellow employees at Seasons Hospice, every day is an important time to grant wishes to their patients, the overwhelming majority of who are dying.
Unlike hospitals, which mainly focus on curative measures for patients — even those who are terminally ill — hospices are intended to provide comfort and love to a person in his or her last days, weeks and even months.
Hospice workers give the gift of dignified end-of-life care daily, holiday season or not, Holmes said, which she added is the most rewarding part of her job.
“Seeing those patients be free of those acute symptoms — to not be writhing in pain, to have that hospice success, to see them share laughs and hugs and things with their grandchildren and their own children — that’s the best,” she said.
“At night when I lay down — and it’s me and God, that’s who I deal with — knowing that that family member made it for their son to come home from the military, for that nephew to come in from out-of-state, for that patient to have their cat on their lap or for them to eat lunch without their oxygen because that’s what they want to do and they don’t care how low their stats drop, it’s those things, just making sure they have what they need, that’s my measure of success.”
The success varies from patient to patient, though, who range in age anywhere from 18 to 98.
“We do get very young patients; usually 18 years old and up, though we do get a lot of 30s, a lot of early 40s and 50s [and] a lot of 60s,” Holmes said. “Usually, cancer is the culprit, unfortunately, and those are especially hard because the [patients] generally have young families and their parents are still with us a lot of times. To have that parent experience the loss of their child at such an early age is absolutely devastating.”
As she continues, Holmes’ smile fades, sadness beginning to cloud her coffee-colored eyes.
“I’ll be honest,” she said. “In my 25 years of nursing, fortunately and unfortunately I’ve been involved in quite a number of situations where you do kind of go numb after a while. When I meet these family members, too, they don’t know what hospice is and I think it’s because there’s not a lot of talk in the community about hospice.
She added: “We’re not here to take anybody’s lives; we’re here to enhance the time that is left, so I do comedy with them. I may crack a little joke and I kind of develop a little joke with each and every family member or patient and that’s what I keep thinking about. It just brings a smile to my face because you know that was a connection that you made with those people.”
It’s the connections, too, that hospice employees make with one another that lighten the nurses’ daily burdens, as well as family, friends and pets.
In Bulldog country, the University of Georgia’s recent SEC championship and the team’s January trip to Pasadena, Calif., where they’ll challenge No. 2 seed Oklahoma in the Rose Bowl Game, also helps, Holmes said.
Lisa Price, one of the facility’s social workers, smiled, half-whispering ‘Go Dawgs’ as Holmes paused, mid-sentence.
“That’s the thing about it,” Price interjected. “We’re a big team and none of us could do our job without the others and the families, too. We have a good social and psych support here, and we’re a team.”
That team is part of what keeps Holmes coming back to work every morning, good days and bad. Her patients, too, make the job worth it.
And, at the end of the day, Holmes said she also knows she can turn on her radio, cued to a Pandora comedy station, and just laugh.
“I have a really good sense of humor; I love to laugh and I love to crack jokes,” she said. “I think it’s real important to keep a good sense of humor because even patients who are terminal, they still like to laugh and joke and kid, and we really enjoy that part, too. It’s not all crying; it can be, some situations that’s just where you’re at, but it’s all about making this better.”
[T]wo state medical societies have dropped their opposition to medical aid-in-dying, a position that mirrors growing acceptance of the practice among many doctors.
The Massachusetts Medical Society on Saturday became the 10th chapter of the American Medical Association to depart from the profession’s long-standing opposition to physician-assisted dying, according to an organization announcement.
The Vermont Medical Society also recently joined the list of medical associations that have voted to take a neutral stance on physician-assisted death. Massachusetts and Vermont joined medical societies in California, Colorado, Maryland, Maine, Minnesota, Nevada, Oregon and the District of Columbia in dropping opposition to what was once called physician-assisted suicide. Supporters of legislation that allows doctors to write a prescription for a lethal dose of medication that terminally ill adults can use to end their lives now prefer the term medical aid-in-dying.
The shift in position is a new one, as nine of those medical societies adopted a neutral stance in the last two years, according to the group Compassion & Choices. The group praised the action by the Massachusetts physicians’ group, which it hopes will improve the chances for passing legislation in the Bay State to legalize aid-in-dying.
The society’s House of Delegates voted to adopt a position of “neutral engagement,” which it says will allow it to serve as a medical and scientific resource as part of legislative efforts that will support shared decision-making between terminally ill patients and their physicians. The change followed the release of a survey of the society’s members that showed they supported the aid-in-dying bill the state legislature is considering by a 2-1 margin, Compassion & Choices said.
Also applauding the decision was Roger Kligler, M.D., a retired doctor who has stage 4 metastatic prostate cancer and filed a lawsuit against the state seeking the right to die using self-administered medication. Compassion & Choices and a fellow physician, who wants the right to prescribe medications to help patients die without fear of prosecution, have joined in that lawsuit.
“I am excited about this decision because the legislature greatly respects the medical society’s positions on healthcare issues and its previous opposition to medical aid-in-dying was a serious roadblock to passing legislation authorizing this end-of-life care option. I’m extremely grateful for the society’s change of heart,” Kligler said in the group’s announcement.
The Massachusetts society’s vote came after considerable discussion, as aid-in-dying raises ethical questions for many physicians.
Six states, including California, Colorado, Montana, Oregon, Vermont and Washington, as well as the District of Columbia, have explicitly authorized medical aid-in-dying
In Vermont, the medical society’s action caught up with existing law. The society dropped its opposition to the state’s 2013 death with dignity law, adopting a resolution at its annual meeting that says doctors have a right to decide if they should assist their patients in ending their lives.
While some physician groups have changed their stance, others have held firm. The American College of Physicians published an updated position statement in September reaffirming its opposition to legalization of what it still calls physician-assisted suicide.
[O]ncology nurses are in the perfect position to implement ideal care for their patients via the use of the family meeting in palliative and end-of-life care. This type of meeting provides an opportunity to coordinate the responsibilities of caregivers and clinicians with patient needs, according to a study by Myra Glajchen, DSW, director of medical education, MJHS Institute for Innovation in Palliative Care, New York, and Anna Goehring, MD, palliative care physician, MJHS Hospice and Palliative Care, New York.1
Oncology nurses usually spend more time with patients than other staff and are able to answer patients’ questions about their medical conditions and discuss end-of-life issues with patients when they are ready to do so. They are also in a good position to evaluate caregivers’ condition and determine how involved caregivers want to be in helping patients make crucial decisions. These decisions are often difficult, yet Ms Glajchen and Dr Goehring write that end-of-life communication skills are not emphasized in the nursing literature.1 They note that the role of the oncology nurse in family meetings is not clear and that there has been little guidance on evaluating and managing caregiver distress.
Family caregivershave their own obligations but often bear heavy, difficult caregiving responsibilities in addition to handling their own personal concerns. Nurses can evaluate the extent to which their caregiving burdens go beyond their skills to cope and provide what their ill family member needs. Oncology nurses also are responsible for assessing the strength of the relationship between patients and their caregivers. A satisfying relationship correlates with a better commitment on the part of the caregiver, although this must be balanced with other activities to avoid caregiving becoming fraught and burdensome.
There must also be a balance with other family members; the researchers stress that a diagnosis of cancer for one family member affects the entire family. Caregivers for patients who are being actively treated for disease are in better physical and emotional health than caregivers for patients receiving palliative and end-of-life care. Oncology nurses should use family meetings to evaluate and structure caregiving situations for patients, caregivers, and their families.
The Meeting
There are a number of reasons for healthcare teams to request a family meeting. Often such meetings are about a decline in a patient’s medical condition or another change in the patient’s prognosis that requires making decisions about new treatments and different options for advance care planning. Meetings may also be called for specific purposes such as completing living wills, do not resuscitate (DNR) and do not intubate (DNI) orders, or to discuss mechanical ventilation, artificial hydration, and nutrition. The nurse’s role is key in these decisions. Oncology nurses are qualified to understand medical information, which they can easily interpret for patients and their families at these meetings. For this reason, it is important for oncology nurses to obtain and review all updated information from the patients’ clinicians prior to the meeting.
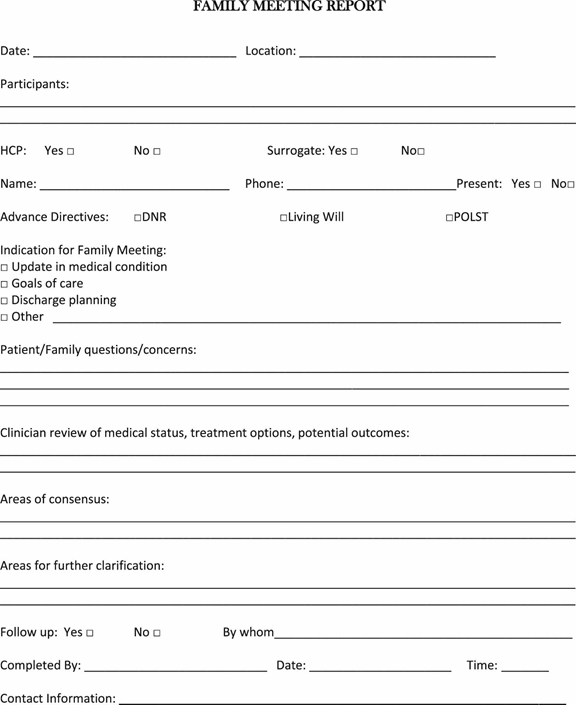
With the oncology nurse at the meeting, other clinicians only need to attend if doing serves a specific purpose.1 However, the participation of involved staff from other disciplines concerned with the patient’s care is helpful. Caregivers the healthcare team or patient wants to invite should attend the meeting, although the researchers caution there should be more caregivers than staff present so as not to overwhelm the family at this difficult time. The care team leader should explain why the meeting was called, provide a clear agenda, and should request all attendees to mute their cell phones and pagers during the meeting. A member of the healthcare team should take notes; the investigators suggested using the Family Meeting Report (Figure 1) and documenting the meeting in the electronic medical record.1
A family meeting takes time; at least an hour for preparation, an hour for the actual meeting, and half an hour to an hour for follow-up is required.1 Despite the work-intensive nature of a palliative care family meeting, the oncology nurse can be a true asset, lowering stress and offering information, realistic hope, supportive care, and comfort to patients, caregivers, and other family members.
Americans are living longer with heart disease, managing it as a chronic condition. But there are few rules for these patients as they near the end of life.
Ricky Hurst, whose heart is failing, was told by doctors to get his affairs in order as his condition worsened. More patients like him are living longer with heart failure, but there are no widely accepted guidelines for care as they near death.
[R]icky Hurst’s doctors told him last year that there was nothing more they could do. His heart was failing and he should get his affairs in order. The end was coming.
His family gathered. He spoke to his pastor and resigned himself to death. “If it was meant to be, it was meant to be,” he said.
But. Mr. Hurst, 56, a former ranger and school football coach in Jackson, Mich., is still alive, although his heart continues to weaken. And patients like him are raising a new dilemma for doctors.
Heart disease once killed ruthlessly and quickly; patients like Mr. Hurst succumbed to heart attacks and sudden death from cardiac arrest. But with improved medical care and implanted devices that bolster the heart, a growing number of heart patients survive for years, even decades, coping with a chronic, progressive condition punctuated by crises and hospitalizations.
Their disease at that point is called heart failure — their weakened heart cannot pump enough blood to supply the body’s needs. The number of Americans with heart failure increased to 6.5 million in 2011-2014 from 5.7 million in 2009-2012, according to the American Heart Association.
More than 10 percent of those over age 80 have heart failure, and more patients are living longer with advanced disease. Even as the death rate from heart attacks is falling, the figure for heart failure is rising.
Yet there are no widely accepted guidelines for dealing with these patients as they near death. Cancer specialists regularly move their patients to hospice at the end of life, for instance, but few cardiologists even think of it. Heart patients account for just 15 percent of hospice deaths, while cancer patients make up half, according to a recent study.
Mr. Hurst carries a battery-powered and surgically implanted heart pump.
That paper, published in the Journal of the American College of Cardiology, reviewed a number of ways in which heart patients are let down at the end of life. Implanted defibrillators often remain activated until the very end, for example, even for those in hospice.
A fifth of heart patients with defibrillators get shocked by them in the last few weeks of life, and 8 percent get shocked minutes before dying. Most patients are never told that they can ask that the defibrillators be turned off.
“Getting shocks at the end of life is not really helping patients live longer or better,” said Dr. Larry Allen, a heart failure specialist at the University of Colorado and an author of the study.
“We shouldn’t have a single one of these cases happening,” said Dr. Haider Warraich, a cardiology fellow at Duke University and first author of the study.
Experts often focus on the strides made in preventing and treating heart disease. Its incidence has declined by 70 percent in the past 50 years. People have heart attacks later in life than they used to, are more likely to survive them, and often live for years afterward with few or no symptoms.
“We are very proud” of that progress, said Dr. Patrice Desvigne-Nickens, a medical officer at the National Heart, Lung and Blood Institute.
Still, she added, cardiologists and their patients should be discussing end-of-life options and palliative care earlier in the course of heart failure.
“Everyone is uncomfortable with end-of-life discussions,” she said. “The field of cancer may be ahead of us. We should learn from looking at their example.”
But cardiologists thrive on the dramatic saving of lives, said Dr. Michael Bristow, a cardiologist at the University of Colorado Denver. They devote their professional lives to rescuing patients having heart attacks and bringing them back from the brink.
End-of-life care is not typically their focus; neither do they spend much time pondering what some of their patients may experience in the future. “Those who go into cardiology are not necessarily ones who want to deal with death and dying,” Dr. Bristow said.
The very nature of end-stage heart failure makes it all the more difficult to prepare.
“Very few patients understand the trajectory of the disease,” said Dr. Lynne Warner Stevenson, a heart failure specialist at Vanderbilt University. The path has peaks and valleys, but as the patient declines, each peak is a little lower than the one before.
And often doctors do not tell patients what to expect.
“Unfortunately, when you have patients with a chronic illness like heart failure, everyone thinks someone else will talk about it,” Dr. Stevenson said. “Too often, no one takes ownership of the last stage of the journey with the patient.”
Dr. Ellen Hummel of the University of Michigan, one of a small number of doctors specializing in cardiology palliative care, said the typical patient with cancer will usually experience a “fairly predictable” decline.
“They will be less able to take care of themselves,” she said. “They will be more symptomatic and come back to the hospital more frequently. And once this starts, it will probably continue until they die. Most people can see the end coming.”
But patients with end-stage heart failure are more likely to have wild swings, Dr. Hummel said, veering from feeling better to being terribly ill.
“It is confusing to both the patient and provider. Are they actually dying, or can we rescue them from a particular episode of worsening?”
Dr. Harlan Krumholz, a cardiologist at Yale University, agreed: “The issue is knowing who is really at the end of life.” For patients with heart failure, seesawing between good periods and bad, it can be very difficult to make the call.
Dr. Allen recently discussed all this with a patient, Ed Harvey.
Mr. Harvey, 75, has an implanted defibrillator, and his heart is weakening, pumping progressively less blood. Dr. Allen gave him medications that helped for a while, but, Dr. Allen said, “we have maxed out on what can be done.”
He can’t say with any certainty how long Mr. Harvey has. But now is the time, Dr. Allen told him, to talk about the end of life.
Mr. Harvey still feels pretty good, but “when you have congestive heart failure and it is not getting any better, you know that day is going to come,” he said.
He has been living with heart failure for more than a decade, and fears becoming a burden as his heart gets worse. It is now so weak that the only medical option left is an implantable pump. He knows that soon he will need full-time care.
“I have elected that if it got to that point,” he said, “put me in a hospice and let me go.”