Samuel LeBaron, MD, PhD, is a family medicine specialist and Stanford Medicine professor emeritus who now faces the situation he guided patients through during his career: navigating terminal lung cancer. In his memoir, Ordinary Deaths, published in July, LeBaron weaves personal stories with vignettes that illuminate the patients whose lives he’s witnessed.
Throughout his career as a family medicine doctor, hospice care provider and technician in a medical examiner’s office, LeBaron jotted down stories of his patients, intent to one day share them with his inquisitive children who asked what he did every day. He chose his words carefully, creating a repository of clinical experience, much of it from a time before hospice existed.
I asked LeBaron to share more about his career and the stories he’s said were a salve in coming to terms with his own mortality.
You’ve talked about how you saw death as a child. What does that mean?
Up until about 5 years old, children have not yet adopted the notion of cause and effect. By the time we’re in the third or fourth grade, we’ve learned we live in a world of rules. So we think the way we live our lives determines how our lives end. One might think that a happy person would feel a bigger loss when they’re facing death. That seems logical. But I’ve personally experienced the opposite. I think of it as a phrase: “I could die happy now.” If we have time to accept our death as the end of a happy life, we’re much more ready to accept it.
The title describes death as “ordinary.” How can death bring meaning to our everyday lives?
The book title was partly ironic because every death I witnessed was extraordinary. On the other hand, they are ordinary deaths in the sense that this happens to everyone in some form or another. Put another way, there is really nothing extraordinary about waves. They just wash up and down the shore, but we love them all the same. And they may help create an extraordinary experience. We may go to the ocean to shed our tears and feel a little bit of comfort from that gentle, constant roll in and out. Our deaths are similar in that way: ordinary and extraordinary at the same time.
What guidance can you share with doctors offering end-of-life care? What have you done for patients in their last hours that you think made the biggest difference to them?
What loosens the tongue faster than anything is a safe, sympathetic environment. There are two basic prompts you need to know: Tell me about yourself and tell me more. Ask questions. Invite the exploration of the question and give a response to let them know they’ve been heard: “I can imagine that was very difficult. I really appreciate you letting me into that story.”
It helps the patient feel heard and valued.
The great tragedy is that for the most part, American physicians — the sweetest, most jolly, most interesting people you could want to meet — are on a treadmill, often seeing too many patients to have time for deeper connection.
What value does writing bring to your life, especially as you face your own illness?
Writing is incredibly meaningful in my life. When I was 14, I found it difficult to communicate the way I wanted. I went from a gregarious, playful kid to a reticent teenager.
I also became distant with my brother. But then something quite remarkable happened: We began to write little stories and sometimes letters to each other. They were all about adventure; some of them were entirely fiction, all of them outrageous, and they entertained us and made us laugh. There were times when we would stay up all night, doing nothing but writing stories. It was so much fun, and it drove my parents crazy.
And then, in my 40s, it occurred to me that all the knowledge gleaned from my patients could disappear if I didn’t write any of it down. Since then, it’s been a process of reintegration after feeling like a bomb went off in my house when I learned of my diagnosis.
My wish is that these stories and lessons be used as a guide — to show people how to be present and supportive, how to let people know you hear them and help them get what they need.
There are two schools of thought among clinicians at end of life: aggressive care, which focuses on treating the illness or condition, and supportive care, which focuses on pain and symptom management.
In this publication, researchers demonstrated how the term aggressive care — used loosely by clinicians to describe care that can negatively impact quality of life for patients with serious illness — is often used to inappropriately label the preferences of African American patients.
“Our motivation through this article was to bring in not only the perspectives of African American Christians, but also to share the biblical and historical backdrop that can be instrumental in shaping their serious illness and end-of-life wishes,” said Shena Gazaway, Ph.D., assistant professor in the UAB School of Nursing and lead author of the study. “In collaboration with our wonderful medical colleagues, we wanted to acknowledge the origins of aggression and discuss how the labeling of care as aggressive with patients and their families can negatively impact care conversations.”
For patients with serious illness such as advanced cancer, dementia and terminal illnesses, the term aggressive care is used to describe courses of treatment that could potentially cause increased physical distress and psychological stress and a decreased likelihood of experiencing a “good death.” The Institute of Medicine defines a good death as “one that is free from avoidable death and suffering for patients, families and caregivers in general accordance with the patients’ and families’ wishes.”
“The data is clear — a larger proportion of African American families reported that their loved one did not receive care that is in accord with what they requested in the final days of their life,” said Ronit Elk, Ph.D., associate director for the UAB Center for Palliative and Supportive Care, and professor in the UAB Division of Geriatrics, Gerontology and Palliative Care and co-author. “We hope this article provides a careful explanation of why these values are so important to the African American Christian community and will strike a chord in many clinicians about the importance of respecting these values and not dismissing the beliefs that these patients and their families about hope and the miracles of God.”
In this article, researchers discuss how many Black Christian adults share a belief in miracles that shapes their end-of-life care decisions. The article states that this belief in miracles combined with an overall distrust in the health care system — due to a history of medical experimentation and centuries of health care disparities — have led many African Americans to depend on their belief in God’s healing power to perform miracles and heal family members who are seriously ill.
The UAB Center for Palliative and Supportive Care offers the African American Communities Speak program to clinicians. This skills-based training incorporates videos created by the African American community to train clinicians on the community’s cultural values, lived experiences and recommendations for care. Self-reflection and active learning techniques provide participants the foundation needed for changed behavior and improved communication with patients and caregivers.
This trust in God, belief in miracles and distrust of clinicians may lead to a seriously ill African American Christian patient to request life-sustaining medical interventions even when recommendations call for supportive care. When facing terminal illness, this hope in miracles often influences the patient’s medical decisions and fuels a desire for life-sustaining interventions. The paper states that these decisions are also rooted in a belief that God ultimately decides the outcome of life, not the health care system.
Researchers say the key to goal-concordant care is for clinicians to allow these patients to process clinical information through their preferred spiritual lens and to allow them time to have critical conversations with those in their network.
“We are hopeful that clinicians will read this article and take away the importance of religious and cultural belief systems in this particular patient population,” said Moneka Thompson, staff chaplain in the Department of Pastoral Care and co-author. “Specifically, we want everyone to understand how the values and beliefs of this particular population may impact their end-of-life preferences and decision-making. This article is the combined effort of five very different women from quite different backgrounds. Our collective goal was to create a think-piece towards movement of health care for this population in a meaningful and more equitable direction. At the end of the day, we want to support health care equity as much as possible.”
Thompson says that there are a few steps clinicians can take to help ensure they are providing goal-concordant care to their patients.
“First, we encourage clinicians to be aware of their own biases towards this patient population that may fuel incongruent care,” Thompson said. “Second, we hope that clinicians will utilize communication practices that encourage cultural sensitivity, humility and curiosity. Finally, we want clinicians to be fully present to the variety of religious and cultural beliefs that this population will present without feeling the need to obtain this value system for themselves or compromise their own.”
— More than half of Medicare beneficiaries are diagnosed with dementia during their lifetime and, of those diagnosed who receive intensive end-of-life care, most are from racial and ethnic minority groups, according to a new study.
“While people with dementia received intensive services less often than people without dementia, those with dementia who did receive intensive services were more likely to be from racial or ethnic minoritized groups,” says Elizabeth Luth.
Intensive treatment includes mechanical ventilation, intubation, feeding tube initiation, and new dialysis.
Researchers have known that race and ethnicity play a role in the intensity of medical care at the end of life, but the difference is more pronounced among individuals with dementia, they say.
“Dementia appears to have a multiplicative effect,” says Elizabeth Luth, an assistant professor in the family medicine and community health department at Rutgers University and lead author of the study published in the Journal of the American Geriatrics Society.
“This difference is not problematic if it reflects patient preferences for intensive services,” says Luth, who is also a faculty member at Rutgers’ Institute for Health, Health Care Policy & Aging Research. “However, additional research is needed to understand whether these differences may be attributable to other factors, including systemic racism, discrimination, poor physician communication, and other barriers to accessing health care.”
To measure the role of race and ethnicity in end-of-life care for people with dementia, Luth and colleagues calculated total medical costs for 463,590 Medicare beneficiaries nationwide. Using claims data, the researchers tallied inpatient, outpatient, carrier, skilled nursing facility, and hospice expenditures for patients’ final 30 days of life. Higher costs indicated greater care intensity.
In addition to determining 51% of Medicare patients die with a dementia diagnosis claim, the researchers made another discovery: Race and ethnicity may influence how people with dementia live out their final days.
“While people with dementia received intensive services less often than people without dementia, those with dementia who did receive intensive services were more likely to be from racial or ethnic minoritized groups,” Luth says.
The magnitude of this effect differed by dementia status. For example, among people without dementia, compared to non-Hispanic Whites, Asian American, and Pacific Islanders had 73% higher odds of intensive care at the end of life. However, among persons with a dementia diagnosis, Asian American and Pacific Islanders had 175% higher odds of receiving intensive procedures.
The findings should prompt efforts to improve end-of-life care and outcomes for people with dementia, Luth says. Medicare reimbursements for physician-led advance care planning conversations could help, she says, as would end-of-life care counseling for all hospitalized patients.
“In the absence of a designated decision maker, the default approach in end-of-life care is to provide intensive services,” Luth says.
“If there isn’t anybody advocating either way, whether it’s the family or the patient themselves, the default is always more hospitalization, which might not be the type of care the patient wants or needs.”
Writing for the New York Times, Daniela Lamas, a pulmonary and critical-care physician at Brigham and Women’s Hospital, explains how doctors and loved ones “navigate death” in cases where “it becomes clear that the life that we can offer is not one that would be acceptable to the patient.”
Making the decision to ‘transition to comfort’
Many people believe that ICU doctors can easily determine whether a patient is going to die, but that’s not always true. “Our medicines and machines extend the lives of patients who would otherwise have died,” Lamas notes.
When a patient is fully relying on these measures—and it has become clear that they are not actively dying but are not improving either—doctors and family members must figure out how to “navigate death when it is not imminent and unavoidable but is instead a decision.”
During Lamas’ medical training, death unfolded in one of two ways: either in a moment of crisis, with doctors rushing into the room, trying to save a patient’s life, or in a quiet room, with loved ones gathered for the patient’s final breaths.
However, Lamas contends that there is a third form of death “when it becomes clear that the life that we can offer is not one that would be acceptable to the patient,” she writes. According to Lamas, this kind of death is planned for, occurring only after the medicines and machines keeping the patient alive are withdrawn.
“It is a strange thing to plan a death, but I have come to understand that this is part of our work in the I.C.U.,” Lamas adds.
For instance, Lamas recently cared for a cancer patient who had been intubated after experiencing a flare-up of underlying lung disease. Before the patient was put to sleep, she instructed her son to “Give her a chance to get better, but if that failed, she did not want a tracheostomy tube for a longer-term connection to the ventilator or months at a rehabilitation hospital,” Lamas recalls. “Her cancer was progressing, and that was not the way she wanted to spend the last year of her life.”
Lamas told the patient’s family that they would continue intensive interventions for two weeks, in “a time-limited trial of critical care.” According to Lamas, if the patient was not breathing on her own after two weeks, she would never be able to breath without a tracheostomy tube and extended rehabilitation—a best-case scenario the patient had already deemed unacceptable.
The day before the time-limited trial was supposed to end, the patient’s son and daughter told Lamas that they wanted to take her off the machines that evening if she was not going to improve.
“There is something uncomfortable about these conversations, where it feels as though we are asking family members to plan the end of a life,” Lamas writes. “It begins with a moment in the family meeting, when we have made the decision to ‘transition to comfort,’ and family members ask me what comes next.” However, “What they are asking, really, is how their loved one will die,” Lamas notes.
The ‘principle of double effect’
After loved ones have made the decision to “transition to comfort,” Lamas explains the next steps. “I tell them that when they are ready — as anyone really can be for any of this — we will stop the medications and the tubes that are prolonging life,” she writes.
In addition, Lamas explains that the bedside nurse will administer other medications to ensure that the patient does not experience pain. “Sometimes they ask if this medication will hasten death, and I explain that it can, but that our primary goal is always to relieve discomfort,” she adds.
Doctors refer to this balance as the “principle of double effect.” According to Lamas, doctors “accept the risk of a negative consequence like hastening death, so long as our intended outcome is to help the patient by alleviating symptoms.”
Ultimately, the pain-relieving drugs doctors administer during this process do not cause a patient’s death. Instead, they ensure that patients are as comfortable as possible while dying from their underlying disease.
We gathered as a medical team in front of my patient’s room early one Saturday. She was one of the sickest patients in the intensive care unit. Her lungs were destroyed by cancer and a rare reaction to her chemotherapy, and her condition worsened each day, despite aggressive interventions. It was clear that there was nothing more that we could do. Except to keep her alive until Monday.
Struggling to come to terms with this reality, her family had begged us to continue our interventions through the weekend. So we would keep her intubated, deeply sedated and, we hoped, pain-free, performing the rituals of intensive care until the family was ready to say goodbye.
There is a largely unacknowledged moment in critical care when doctors and nurses shift from caring for the patients in front of us to caring for their loved ones. Often these two aims are not inconsistent: Even when family members like these are not ready to stop life-prolonging interventions or ask for a treatment that is unlikely to work, they are speaking on behalf of the patient. But increasingly I wonder if it is possible to go too far to accommodate family. When a patient is at the end of life, what is our responsibility to those who will be left behind?
On another recent shift, I received a call from a colleague at a different hospital. He was caring for a patient in his 60s with severe respiratory failure after a coronavirus infection. The patient’s family was desperate for him to be transferred to our hospital, a larger institution with greater resources. But intensive care unit beds were a scarce resource, and there was no clear medical reason for the transfer. His team had already done everything that we would do, and the simple act of transferring someone so sick could be catastrophic. I was the critical care doctor on call, charged with accepting transfer requests, and it would have been easy to say no. But then there was the matter of his family.
The patient arrived overnight, just as sick as we expected. His oxygen levels had dipped in the move and never recovered. Standing outside his room the next morning, his wife asked me if I thought the transfer had been a mistake.
Maybe it was. Not because his numbers were worse; that was inevitable, regardless of the transfer. But because I had made the choice to bring someone to our hospital in large part so that his family members would believe they had done absolutely everything. Of course, family request alone is not a sufficient reason for a hospital transfer. And though I suspected that we would have nothing more to offer in terms of medical interventions, that was not possible to know with absolute certainty when the other hospital called. But perhaps even more important, I did not want his family to wonder what might have been.
And so the transfer was an act of caring for him, too, to leave his family without regret. I do not believe that we went against his wishes, sacrificed his dignity or caused him pain. When he died a few days later, it was peaceful, with his family at the bedside.
But that’s not always the case. Not infrequently a family will demand that doctors perform chest compressions and shocks if someone’s heart stops, even though we are nearly certain it won’t help. I used to find myself infuriated by these conversations. On occasion I have used hospital policy to take the decision away from the family altogether. But maybe that is not the only response.
Some years ago, Dr. Robert Truog, a critical care doctor and ethicist at Harvard, published a provocative essay arguing that there may be a role for cardiopulmonary resuscitation if it is necessary for the family, even if it will not directly benefit the patient. He told the story of a chronically ill child with a dismal prognosis whose parents were unwilling to stop aggressive measures. During one hospital admission, the child’s heart stopped, and at the parents’ behest, the team moved forward with attempts at cardiopulmonary resuscitation. When the efforts ended and the child had died, the parents entered the room, surveyed the detritus of the cardiac arrest, the lines and the tubes, and surprised the medical team members by thanking them for doing everything. Dr. Truog wrote that even if it was futile from a medical perspective, what he had come to realize was that the procedure let the family members know that the doctors had tried. That was the way to give them a narrative they could live with.
I am still not sure what to make of this argument. We would not resuscitate patients against their stated wishes, regardless of what their loved ones want. But in these moments, we are so often making decisions for both the patients in front of us and the people who will carry their story forward. And so maybe resuscitation attempts can be for a family just as much as or even more than they are for a patient. Maybe in some cases, that is justification enough.
But at the same time, I worry that even if my patients are beyond pain, there is also a cost to those who are forced to perform emergency efforts that are just that: a performance. I wonder, too, whether this very scenario means that doctors have failed. Perhaps if we were clearer communicators, no family members would choose for their loved ones to undergo intensive treatments that only postpone the inevitable.
That Saturday in the I.C.U. passed quietly for my cancer patient. But when I returned on Sunday, I learned that her blood pressure and oxygen levels had started to teeter when the nurses turned her, as they did every few hours to prevent bedsores. The daily activities of critical care were beginning to cause harm. We had planned to wait until Monday to readdress goals with the family, but was that the right choice? I hoped my patient was pain-free but could not guarantee it. And perhaps it was unkind to allow her family to spend another day hoping she might improve when we knew that to be impossible.
We called in her adult children and told them that their mother was dying. They cried and questioned, and I asked myself whether I should have waited, but they ultimately understood. If there was no way that doctors and nurses could make their mother better, then they would focus on her comfort. They gathered by the bedside. We waited for a chaplain. And late that night, in the last of our many rituals, a nurse disconnected my patient from the ventilator, ensuring she had enough medications so that she would not struggle. It was a final act of compassion, at once for the patient, her family and for us, too.
Health and social systems around the world are failing to give appropriate, compassionate care to people who are dying and their families. According to a new Lancet Commission, today’s current overemphasis on aggressive treatments to prolong life, vast global inequities in palliative care access, and high end-of-life medical costs have lead millions of people to suffer unnecessarily at the end of life.
The Commission calls for public attitudes to death and dying to be rebalanced, away from a narrow, medicalised approach towards a compassionate community model, where communities and families work with health and social care services to care for people dying.
Bringing together experts in health and social care, social science, economics, philosophy, political science, theology, community work, as well as patient and community activists, the Commission has analysed how societies around the world perceive death and care for people dying, providing recommendations to policy makers, governments, civil society, and health and social care systems.
“The COVID-19 pandemic has seen many people die the ultimate medicalised death, often alone but for masked staff in hospitals and intensive care units, unable to communicate with their families, except digitally”, says Dr. Libby Sallnow, palliative medicine consultant and honorary senior clinical lecturer at St Christopher’s Hospice and UCL (UK) and co-Chair of the Commission, “How people die has changed dramatically over the past 60 years, from a family event with occasional medical support, to a medical event with limited family support. A fundamental rethink is needed in how we care for the dying, our expectations around death, and the changes required in society to rebalance our relationship with death.”
The Commission focuses primarily on the time from when a person is diagnosed with a life-limiting illness or injury, to their death and the bereavement affecting the lives of those left behind—it does not cover sudden or violent deaths, deaths of children, or deaths due to injustice.
Death and dying have become over-medicalised, hidden away and feared
Over the past 60 years, dying has moved from the family and community setting to become primarily the concern of health systems. In the UK for example, only one in five people who require end of life care are at home, while about half are in hospital (table 2).
Global life expectancy has risen steadily from 66.8 years in 2000 to 73.4 years in 2019. But, as people are living longer, they are living more of these additional years in poor health, with years lived with disability increasing from 8.6 years in 2000 to 10 years in 2019.
Prior to the 1950s, deaths were predominantly a result of acute disease or injury, with low involvement from doctors or technology. Today, the majority of deaths are from chronic disease, with a high level of involvement from doctors and technology. The idea that death can be defeated is further fuelled by advances in science and technology, which has also accelerated the over-reliance on medical interventions at the end of life.
And, as healthcare has moved centre stage, families and communities have been increasingly alienated. The language, knowledge, and confidence to support and manage dying have been slowly lost, further fuelling a dependence on health systems. Despite this, rather than being viewed as a professional responsibility for the doctor, and a right for all people and families who wish it, conversations about death and dying can be difficult and uncomfortable and too often happen in times of crisis. Often they don’t happen at all.
“We will all die. Death is not only or, even, always a medical event. Death is always a social, physical, psychological and spiritual event and when we understand it as such we more rightly value each participant in the drama,” adds Commission co-author, Mpho Tutu van Furth, priest, Amstelveen, Netherlands.
Worldwide, too many people are dying a bad death
While palliative care has gained attention as a specialty, over half of all deaths happen without palliative care or pain relief, and health and social inequalities persist in death.
Interventions often continue to the last days with minimal attention to suffering. Medical culture, fear of litigation, and financial incentives also contribute to overtreatment at the end of life, further fuelling institutional deaths and the sense that professionals must manage death.
Dr Libby Sallnow and Dr M.R. Rajagopal call for radical rethink of how society cares for dying people. Today’s current overemphasis on aggressive treatments to prolong life, vast global inequities in palliative care access, and high end-of-life medical costs have lead millions of people to suffer unnecessarily at the end of life. The Lancet Commission on the Value of Death provides recommendations to policy makers, governments, civil society, and health and social care systems. Credit: The Lancet
Untreated suffering, vast inequalities, and aggressive medical treatments have come at a high cost. A disproportionate share of the total annual expenditure in high income countries goes towards treatment for those who die, suggesting that treatments at the end of life are being provided at a much higher threshold than for other treatments.
In high income countries, between 8% and 11.2% of annual health expenditure for the entire population is on the less than 1% who die that year (table 6). Care in the last month of life is costly and, in countries without universal health coverage, can be a cause of families falling into poverty.
“Dying is part of life, but has become invisible, and anxiety about death and dying appears to have increased. Our current systems have increased both undertreatment and overtreatment at the end of life, reduced dignity, increased suffering and enabled a poor use of resources. Healthcare services have become the custodians of death, and a fundamental rebalance in society is needed to re-imagine our relationship with death,” says Dr. Richard Smith, co-Chair of the Commission.
A fundamental change to society’s care for the dying is needed
The Commission sets out five principles of a new vision for death and dying:
1. The social determinants of death, dying and grieving must be tackled, to enable people to lead healthier lives and die more equitable deaths.
2. Dying must be understood to be a relational and spiritual process rather than simply a physiological event, meaning that relationships based on connection and compassion are prioritised and made central to the care and support of people dying or grieving.
3. Networks of care for people dying, caring, and grieving must include families, wider community members alongside professionals.
4. Conversations and stories about everyday death, dying, and grief must be encouraged to facilitate wider public conversations, debate, and actions.
5. Death must be recognised as having value. “Without death, every birth would be a tragedy.”
The Commission recognises that small changes are underway—from models of community action to discuss death, national policy changes to support bereavement, or hospitals working in partnership with families. While wholescale change will take time, the Commission points to the example of Kerala, India, where over the past three decades, death and dying have been reclaimed as a social concern and responsibility through a broad social movement comprised of tens of thousands of volunteers complemented by changes to political, legal, and health systems.
“Caring for the dying really involves infusing meaning into the time left. It is a time for achieving physical comfort; for coming to acceptance and making peace with oneself; for many hugs; for repairing broken bridges of relationships and for building new ones. It is a time for giving love and receiving love, with dignity. Respectful palliative care facilitates this. But it can be achieved only with broad-based community awareness and action to change the status quo,” says co-author Dr. M.R. Rajagopal, Pallium India, India.
To achieve the widespread changes needed, the Commission sets out key recommendations for policy makers, health and social care systems, civil society, and communities, which include:
Education on death, dying, and end of life care should be essential for people at the end of life, their families and health and social care professionals.
Increasing access to pain relief at the end of life must be a global priority, and the management of suffering should sit alongside the extension of life as a research and health care priority.
Conversations and stories about everyday death, dying, and grief must be encouraged.
Networks of care must lead support for people dying, caring, and grieving.
Patients and their families should be provided with clear information about the uncertainties as well as the potential benefits, risks, and harms of interventions in potentially life-limiting illness to enable more informed decisions.
Governments should create and promote policies to support informal carers and paid compassionate or bereavement leave in all countries.
Researchers conducted an international survey to determine what constitutes good end-of-life care and which countries are the best at providing it.
They scored 81 countries, most of which earned a grade of “C” or below for their palliative care. The United Kingdom ranked first. The U.S. ranked 43rd.
Higher income, universal health coverage, and wide availability of opioids for pain relief were generally associated with better scores.
Death is an inevitable part of life — a mysterious climax that all humans face, evoking wonder and trepidation. That’s why dependable end-of-life care is so vital. While only some of us break bones, develop cancer, or catch an infectious disease, we all die eventually. To depart with dignity in relative comfort shouldn’t be a rare privilege.
Regretfully, new research published in the Journal of Pain and Symptom Management shows that many countries do not offer their citizens a good death.
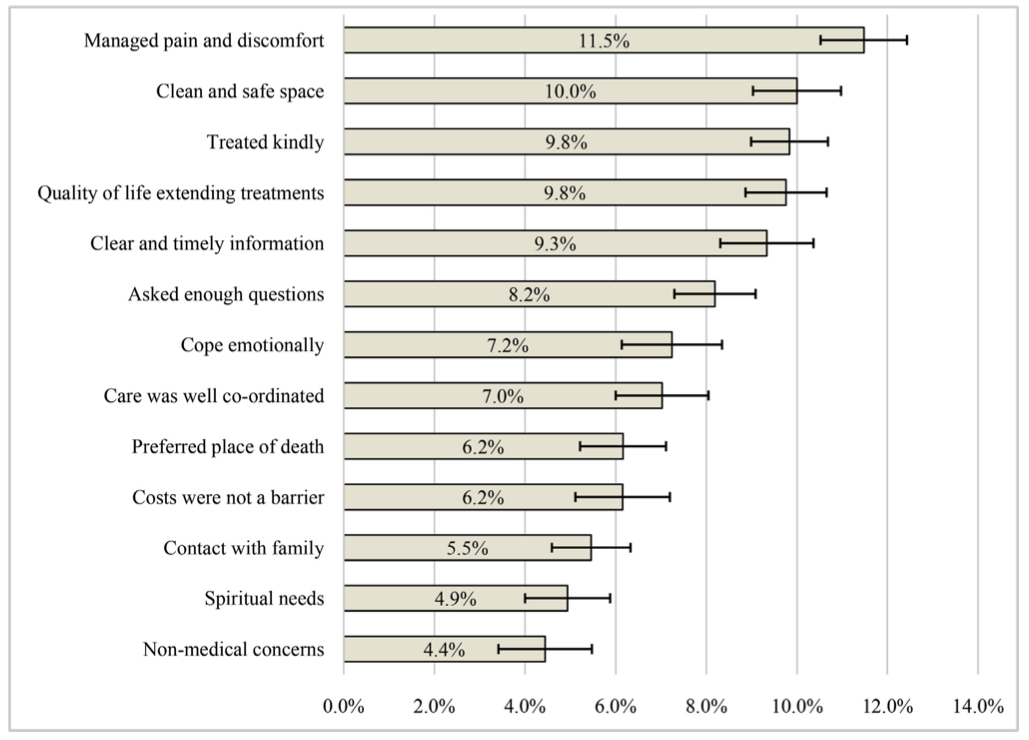
Eric Finkelstein — a professor of health services at the Duke-NUS Medical School, Singapore, and the Executive Director of the Lien Centre for Palliative Care — led an international team of researchers to conduct a sweeping analysis of countries’ end-of-life (palliative) care. Finkelstein and his colleagues first set out to characterize quality end-of-life care, reviewing 309 scientific articles to determine the factors involved. A few that they identified included:
The places where health care providers treated patients were clean, safe, and comfortable.
Health care providers controlled pain and discomfort to patient’s desired levels.
Health care providers provided appropriate levels and quality of life extending treatments.
Costs were not a barrier to a patient getting appropriate care.
The researchers settled on 13 factors in total. They then surveyed 1,250 family caregivers across five different countries who had recently looked after a now-deceased loved one to ascertain the relative importance of each indicator. Here’s how the factors ranked:
Credit: Finkelstein et al. / Journal of Pain and Symptom Management
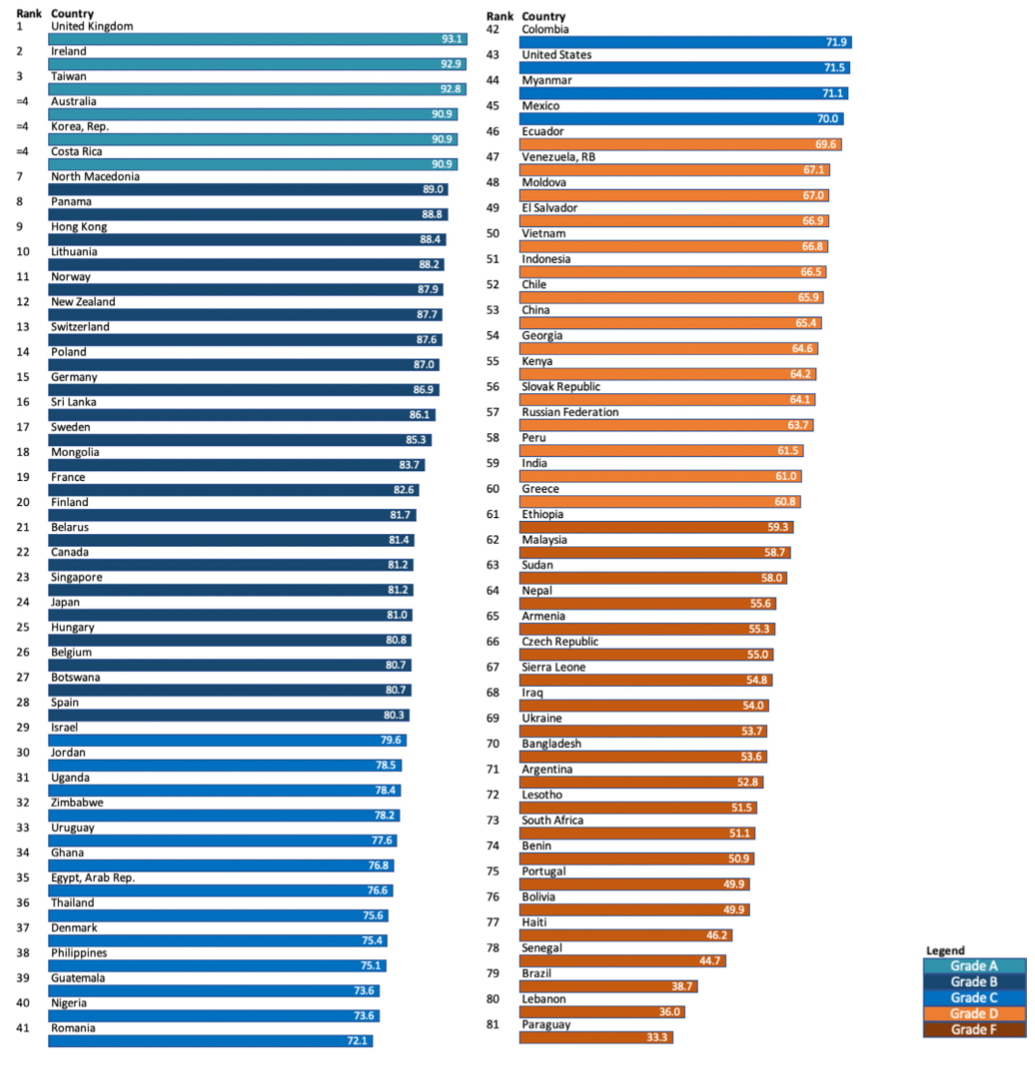
Finally, the researchers sought out hundreds of experts from 161 countries to rank their respective country’s end-of-life care based on these weighted factors, asking them to “strongly disagree, disagree, neither agree nor disagree, agree, or strongly agree” with whether their country’s healthcare system generally met each palliative need. To be eligible, experts had to be “either 1) a representative of the national in-country hospice-palliative care association or similar national professional association with an established leadership role, 2) a health care provider (physician, nurse) involved in provision of palliative care, or 3) a government employee or academic with knowledge of palliative care in the country.”
At least two experts were required to respond from a specific country for the researchers to consider the nation’s score valid. In all, 81 countries comprising 81% of the world’s population ended up being ranked.
Credit: Finkelstein et al. / Journal of Pain and Symptom Management
The United Kingdom earned the highest score in the study, followed closely by Ireland, Taiwan, Australia, South Korea, and Costa Rica. These were the only countries to earn an “A” grade, scoring 90 or above. Ukraine, Argentina, South Africa, and Lebanon were a few of the 21 countries to merit an “F” grade, scoring 60 or below.
Finkelstein found the results disheartening.
“Many individuals in both the developed and developing world die very badly – not at their place of choice, without dignity, or compassion, with a limited understanding about their illness, after spending down much of their savings, and often with regret about their course of treatment,” he said in a statement.
Higher income, universal health coverage, and wide availability of opioids for pain relief were generally associated with better scores.
Of note, the United States earned a “C”, ranking 43rd of the 81 countries with a middling score of 71.5. Commenting on why the U.S. ranked so poorly, especially compared to other high-income countries, Finkelstein said that Americans often spend tons of money on excessive, often futile treatments and surgeries aiming to extend life at the dusk of one’s existence — sometimes just for weeks or months — rather than focusing on ensuring quality of life at the end.
A key drawback of the study is that each country’s ranking was determined by an average of only two experts. While the researchers made clear that these experts are quite knowledgeable and respected, it seems hardly fair to rate an entire country’s end-of-life care system based on the opinions of just two individuals, each of whom is undoubtedly biased by their own experiences.
The experts were also asked for their thoughts on what facilitates good end of-life-care in a country. Collectively, they suggested that investment from the national government, patient-centered, integrative care, and universal healthcare with free access to palliative care services contributed greatly.