In recent months, I read a very powerful piece in The New York Times that detailed the last day in the life of President George H. W. Bush. It described how in the last week of the president’s life he had stopped eating and was mostly sleeping.
His longtime friend and colleague, James Baker visited him frequently in his last days, and was there when he passed away. Baker described how, at the end, he held Bush’s hand and rubbed his feet.
The former president died in his home, surrounded by several friends, family members, doctors and a minister. As the end neared, his son George W. Bush, also a former president, who was at his own home in Dallas, Texas, was put on speaker phone to say goodbye.
He told his father that he had been a “wonderful dad” and that he loved him. “I love you too,” Bush told his son. And those were his final words.
Bush’s doctor described how everyone present knelt around the president and placed their hands on him and prayed for him. It was a very graceful and gentle death, accompanied by loved ones who gathered in the intimacy of his home in Houston.
For almost four years now, I have been privileged to visit nursing homes, assisted living facilities and private homes to sing and play music for people in hospice under the title of my role as “Chords of Comfort.” I also make visits as a hospice chaplain.
On some days, my patients are alert and able to converse with me. On others, they lie in bed unable to speak and sometimes sleep.
On such occasions, I sit by their bedside and just keep them company. Sometimes a family member or two is present when I visit.
Several years ago when I arrived to visit a certain patient, I was surprised to find members of her family singing and playing guitar while the patient, who could not speak, moved her head rhythmically back and forth.
One of her youngest grandchildren had flown all the way from San Francisco, Calif. to New Jersey just to sing for her great grandmother. It was obvious that the singing and playing brought great comfort and pleasure to her.
When the family asked me to join in with my guitar, it became clear to me that we all were feeling spiritually uplifted by the beautiful music that we created together.
There is a rabbi who directs a Jewish-end-of-life care/hospice volunteer program. As part of his training program, the rabbi asks the volunteers to reflect on a moment when they were in need of someone to be present for them.
One man related the story of his bicycle accident when a stranger sat silently with him on the curb until the ambulance arrived. Another volunteer described how her grandmother sat knitting in the corner of the hospital’s delivery room throughout her three-day-long labor.
What both of these stories have in common is the power of someone simply being present for another person.
Chaplaincy – spiritual care – is all about accompanying another person while being fully present. It is all about trying to ensure that there will be times during the day when a patient is not left alone and has someone by their side.
Even when someone’s life is transitioning, healing of spirit is possible until the very last breath. It is especially at these times when our very presence can raise their spirits, which not only benefits them, but also us.
Being present and ensuring that no one is left alone is an incredible act of kindness and a supreme act of holiness. In the Jewish faith, it is considered a “mitzvah,” a religious obligation.
I hope that you will consider ways that you can help reduce isolation for those who are alone and provide them with “accompaniment.” Let us continue to find ways to be fully present for members of our own family and for those in the wider community who will benefit from our companionship and just “being there for them.”
Perhaps you may wish to consider committing to one specific act of accompaniment each month that will lift the heart and brighten the spirit of someone else – and probably do the same for us.
Images of sandy beaches, sun-kissed swimming pools and azure blue skies gleam from the window and walls of what appears to be a new travel agent opening in a London shopping centre. But browsers may be surprised by the destination, for it is a journey every one of us will one day take: death.
Look more closely at the posters and it becomes clear that the words are all about “passing away” (half of British adults prefer to avoid the word “death”, apparently). The Departure Lounge, in Lewisham, south London, is the brainchild of the Academy of Medical Sciences, whose mission is to promote biomedical and health research. Death, it turns out, is one of the most under-researched areas in healthcare, accounting for less than half of 1% of money spent.
The idea of the Departure Lounge, explains the academy’s president Professor Sir Robert Lechler, is to enable visitors to ask any questions they might have about the dying process, and also to collect ideas and experiences that could inform future research. “The best time to have conversations about death probably isn’t when you’re confronting it, but well before,” he said. Which is why a shopping centre was deemed an appropriate location – the hope is that the Departure Lounge will attract people who might not be regular visitors to science museums.
Death has been a zeitgeist subject for some years now – witness the Death Café phenomenon, the growth of conferences and books on dying and TV series like the recent Ricky Gervais Netflix comedyAfter Life. But, says Lechler, the conversation is becoming more urgent. Put simply, there’s more of it about. “Between now and 2040 we’ll see an increase of 25% in the number of deaths per year,” he said. And it’s more than numbers: the run-up to dying is different. “We’re living longer, and the context of death is changing. Longer life means we accumulate more long-term conditions, and people tend to be frail for longer,” he said. “The risk is that people are going to die badly, as opposed to dying well.”
Dr Katherine Sleeman, a palliative care consultant at the Cicely Saunders Institute at King’s College London and a member of the advisory group behind the Departure Lounge, says patients often want to talk about death. “People call it the last taboo, but that’s not my experience. Healthcare professionals can be fearful about raising the subject, but I find patients are often relieved when it’s mentioned. They know they’re dying, and they want to talk about it.”
Also much misunderstood, she says, is that palliative care, far from spelling the end, can mean much better outcomes. “Research shows that when provided early, palliative care is associated with fewer hospital admissions, better pain relief and lower financial costs to the NHS,” she said. “I always say that my aim isn’t to help you live longer, it’s to help you live better.”
On hand will be guides including Yvonne Oakes, a former palliative care nurse who now works as a “soul midwife” or end-of-life doula, supporting patients and their families. In her experience, many people have had negative experiences of death with relatives, and assume that when their time comes isolation, pain and discomfort will be inevitable. That, she says, simply isn’t true. “There is definitely such a thing as a good death. It comes mostly, I believe, from accepting death rather than struggling against it.” And The Departure Lounge, she hopes, will enable people to start to think about acceptance of death, “in a non-threatening, and unforced, way.”
Research into dying, says Sleeman, really matters and can make a real difference. “Many people, and that includes doctors and academics, say: what’s the point of research if it’s not going to prolong life? But that isn’t the point. Quality is crucial: research is quite clear that most people would choose quality of life over length of life.”
The Departure Lounge is supported by the Health Foundation and Wellcome Trust; more information at departure-lounge.org
Top tips for a good death
Remember this is your death: it’s OK to think about what you really want and don’t want, and be clear about it.
Don’t be afraid to ask for help, and to accept help if it’s offered and you want it. You don’t have to struggle on alone.
Make amends for past hurts and disappointments. Some people write letters – you don’t have to post them.
Consider making a death plan, which is the life-end equivalent of a birth plan. Where would you like to die? Who do you want with you – and who do you not want there? Would you like music to be playing? Do you want to avoid attempts to resuscitate you?
Be aware that death involves loss, so there is inevitably going to be emotional pain, both for you and for those you love. But that doesn’t mean you can’t look for the joys in life, even as your health deteriorates. Life can have meaning and enjoyment right up to the end.
Anne Brescia sits in the room of her only child, Anthony Gabriel Brescia-Connell, who died of cancer in 2011. The hospital sent him home so he could die there with his family.
By Melissa Bailey
Anne Brescia sat beside her only child, Anthony, as he lay unconscious in a hospital bed at age 16. Just a few months before, he was competing in a swim meet; now cancer was destroying his brain. Brescia couldn’t save her son. But she was determined to bring him home.
Anthony Gabriel Brescia-Connell was not conscious for his voyage from Boston Children’s Hospital to his home in Medford, Mass., where he died on March 3, 2011, surrounded by his family and beloved stuffed animals. He may not have heard the parting blessings before a doctor turned off his portable ventilator and let him die naturally.
But having the choice to take Anthony home, away from the beeping hospital monitors, “meant the world to me,” his mother said.
Anthony’s journey was made possible through swift and unconventional efforts by the hospital staff, including a critical care transport team accustomed to rushing kids to the hospital to save their lives, not taking them home to die.
The experience galvanized Harriett Nelson, a nurse on that team who helped arrange the trip. It inspired her to conduct pioneering research on and advocate for “pediatric palliative transport” — a rare but growing practice that aims to give families choice, control and comfort at the end of life.
Palliative transport lets families move critically ill children from the hospital intensive care unit to their home or hospice, with the expectation they will die within minutes to days after removing life support.
It means “having parents go through the hardest thing they’ll ever know — in the way they want to do it,” Nelson said. Boston Children’s has sent 19 children to home or hospice through palliative transport since 2007, she said.
These final journeys — also offered by the Mayo Clinic, Children’s Hospital of Philadelphia and Kentucky Children’s Hospital — can involve elaborate planning, delicate transfers and even long helicopter rides. In some cases, families took a child far from home for a last-ditch effort to save their lives.
At the Mayo Clinic, palliative transport has helped culturally diverse families carry out end-of-life wishes for their dying children. In one case, a newborn girl rode 400 miles by ambulance to return to her Amish community, where she was extubated and died in her parents’ arms, in the company of her 11 siblings. In another, an 8-month-old Native American girl traveled 600 miles by air and ground ambulance to her rural tribal reservation, where she could participate in end-of-life rituals that could not be done in the hospital.
These trips, which can cost thousands of dollars, are typically offered free to families, paid for by hospitals or charities. Most children are taken home, where they transition to receiving care from hospice staff. Some go instead to hospice facilities.
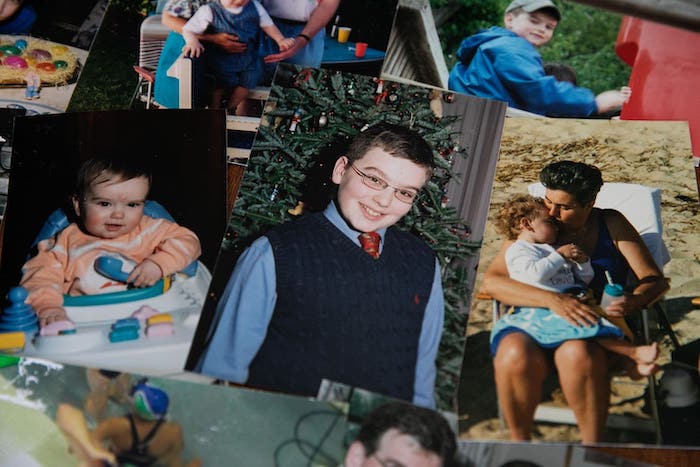
A collection of photos of Anthony Gabriel Brescia-Connell, who was 16 when he was transported from Boston Children’s Hospital to his home in Medford, Mass., where he died on March 3, 2011, surrounded by his family and beloved stuffed animals.
Megan Thorvilson, a pediatrician and palliative care specialist at Mayo, said palliative transport aims to address a gap between families’ preference and reality.
Most parents of terminally ill children would prefer that their child die at home, but most of these children die in the hospital, most commonly in the intensive care unit. Most pediatric ICU deaths happen in a controlled way, following the removal of life support, she said. That means there may be time to move the child to an alternative location to honor a family’s wishes.
Transporting children on life support is risky. At a palliative care conference, a nurse from Children’s Hospital of Philadelphia described the difficulties staff faced in trying to fly a 10-year-old girl home to Michigan. After she was rolled on her side several times to be transferred between vehicles, the child died before the plane could take off.
And dying at home is not what every family wants.
“We do sometimes overly romanticize the death at home,” Thorvilson acknowledged. Some parents would much rather have a child die in the hospital, with familiar nurses at the bedside for medical and emotional support. Some would rather keep this traumatic experience away from where they live.
Brescia, however, said she couldn’t bear to return home without her son.
A biologist who used to run an electron microscopy lab, Brescia wasn’t sure whether she and her husband, Brian Connell, would ever have children. Fertility treatments didn’t work. But on June 23, 1994, seven days before Brescia turned 44, she gave birth to a baby boy.
“Anthony is the love of my life,” said Brescia, who is now 68. “The OB/GYN put him on my chest and I really thought that my heart was going to burst.”
The mother-son bond was especially close: Brescia home-schooled her son for most of his life. Anthony grew to be 6 feet tall, full of curiosity. He loved identifying mushrooms, studied Arabic and oceanography, and aspired to go to MIT. He was an avid swimmer, competing on a team in Belmont, Mass.
One day in late 2010, while racing the backstroke, he became disoriented in the pool and was disqualified.
A neurologist prescribed rest. But over the next two weeks, Anthony grew only more tired and began to lose his balance. On Dec. 20, he was taken to Boston Children’s Hospital and diagnosed with a brain tumor.
The disease “came out of nowhere,” Brescia recalled. “He went from looking incredibly healthy and swimming like a healthy kid” to living at the hospital. At his bedside, she told him she’d bring him home to celebrate Christmas and eat stuffed shells.
His condition deteriorated quickly. The tumor could not be surgically removed. Anthony pushed through radiation and chemotherapy with the hope of going home, but the treatments failed. By late February 2011, the tumor began pressing on his brain stem, and fluid was building up in his brain.
Anthony was unconscious, relying on a ventilator to breathe. Brescia connected with the hospital’s palliative care team.
“I want to bring him home tomorrow,” Brescia told staff.
“I was scared to death he was going to have another incident,” she recalled. “I didn’t want them to do any more invasive procedures to reduce the pressure on his brain.”
Staff from the ICU, palliative care and transport teams scrambled to honor her request. The critical care transport team arranged for the use of its ambulance, a mobile ICU the size of a small bus.
The night before the trip, Brescia said goodbye in the privacy of Anthony’s hospital room.
“I don’t want to lose you,” she told him, holding his hands. “I’m going to let go. I want you to go where you need to be.”
On March 3, 2011, Brescia and her husband boarded the bus along with Anthony, a chaplain, two doctors, Nelson and a nurse from the ICU. They rode 10 miles to the family’s home, where Anthony was laid on a hospital bed in his living room, surrounded by his stuffed animals, on his favorite flannel sheets.
A pastor held a service for Anthony, and close family gathered to say goodbye. Then Brescia signaled for a doctor to disconnect the ventilator.
Anthony seemed to be at peace, Brescia said. After he died, she climbed into the bed with her son and held onto him for a while.
The death was still traumatic. But “it was really a gift to bring him home,” she said. “It was a significant act of compassion and kindness and love on the part of the Children’s staff.”
After Brescia’s experience, Nelson was inspired to offer the choice to more families.
First, she interviewed Brescia and other parents about whether palliative transport had a positive effect. All nine parents said it had. One family described holding a celebration when they brought their newborn baby home, even though he was about to die. They took family photos and used the nursery they had set up, establishing a brief sense of normalcy for four days before he died.
In her 14 years on Boston Children’s critical transport team, Nelson has found that parents benefit from palliative transport for various reasons: At home, they’re away from the noise of the hospital. They have control over who can visit. They feel more comfortable. And they don’t feel rushed after their child dies.
Nelson created a protocol that allows the hospital to offer palliative transport in a more routine way. Now, when children come to any of the hospital’s four ICUs, Nelson said, “we have the power to say, ‘You have a choice when it comes to the end of life.’ ”
The practice appears to be spreading.
After Lindsay Ragsdale, the physician who is director of the palliative care team at Kentucky Children’s Hospital in Lexington, presented her protocol for palliative transport at a conference last year, staff from 20 hospitals asked her to share her checklist, she said.
Mayo’s Thorvilson, who has worked closely on a half-dozen palliative transports, said it’s possible these last-minute trips from ICU to home could be avoided by earlier referrals to hospice, which might get kids home sooner. But when children with complex illnesses get sick, she said, “sometimes it’s hard to know whether this is just another bump in the road, or whether this is the natural end of the child’s life.”
“There’s something really unique about a child dying,” she said. “Everyone’s heart breaks, and we want to be able to do all that we can to be able to support the family in the midst of the tragedy.”
Eight years after Anthony’s death, his bedroom remains untouched, his socks still folded in his top drawer, swimming trophies on the cabinet, slippers under his chair. Pictures of him adorn every room in the house — on the fridge, the kitchen table, the living room stereo.
Looking through photos one recent morning of her son fishing and blowing out birthday candles, Brescia struggled to hold back tears.
“I couldn’t cure him,” she said. “I failed to protect him from a tumor — that’s how you feel. They did all they could. It wasn’t enough. Bringing him home was the best I could do.”
In his three-volume collection of Essays (1580), the French thinker Michel de Montaigne (1533–1592) famously declared that the best way to prepare for death was to think about it constantly. “Let us have nothing so much in minde as death. At the stumbling of a horse, at the fall of a stone, at the least prick with a pinne, let us presently ruminate and say with our selves, what if it were death it selfe?” Montaigne advised that we must contemplate death at every turn and in doing so, we make ourselves ready for it in the most productive way possible. On a more personal note, I managed to achieve this by spending four years writing a Ph.D. thesis on Montaigne’s work, a task which forced me to contemplate death every single day.
Arguably every Ph.D. dissertation carries with it a certain amount of doom and gloom at some point or other, especially during the last few months of writing up. But studying time in Montaigne’s work meant being constantly steeped in his musings and recollections on how ancient philosophers viewed suicide, or the history of funeral practices in Western Europe. By the time I had finished, I was sure Montaigne was wrong, and that in fact I should never think about death again. The stress and anxiety surrounding my submission date meant that the words of a 16th century nobleman concerning the nature of death were low on my list of priorities. And yet on reflection, thanks to Montaigne and his open and honest approach to mortality, thinking about death has actually taught me a lot about how to live.
Thanks to Montaigne and his open and honest approach to mortality, thinking about death has actually taught me a lot about how to live.
Despite what many of us may think in today’s society, talking about death on a regular basis doesn’t have to be scary or morbid. In fact, it can actually make us feel a much deeper connection to the natural world that simultaneously puts the little things into perspective. After all, mortality is a key feature of pretty much everything that exists in Nature, human beings included. The sun, stars, plants and animals — nothing lasts forever, and Montaigne constantly argues in his writing that this is most evident in the mutable physical processes that occur around us: “The world runnes all on wheeles. All things therein moove without intermission.” Winter storms and snows give way to summer sun, flowers wilt and perish. Even the Sun will disappear one day. As humans we fit perfectly into this cycle; we regularly define our lives in terms of birth, aging and death. Montaigne describes his own aging body using seasonal imagery: “I have seene the leaves, the blossomes, and the fruit; and now see the drooping and withering of it [his body].” However, in the natural world, death always gives way to new life. Leaves fall from trees and die before the arrival of new shoots that burst forth in the spring. When human beings die, their bodies decompose and mingle with the Earth, or sail along the breeze as specks of dust, ready to become part of something else.
Thinking about death in this way really helped me to understand that our lives are only one small piece of a much bigger picture — and the bigger picture doesn’t care about how many Twitter followers a person has, or how much money they earn, or where they buy their clothes. It’s easier to put trivial things to one side when we think about how our death actually confirms a meaningful, physical connection to the world around us — we are natural beings who arguably exist for a certain length of time before returning back to the Earth in some form or another. If you’re a fan of The Sopranos, this attitude is perhaps best summed up by the old Ojibwe saying that Tony finds in his hospital room — “Sometimes I go about in pity for myself, and all the while a great wind carries me across the sky.” The end of our life doesn’t mean the end of Nature’s great cycle. As Montaigne remarks, we can find comfort in the fact that our death is merely one part of a much greater plan: “your death is but a peece of the worlds order, and but a parcell of the worlds life.” His tone is so self-assured in the expression of these ideas that his writing becomes living proof of our ability to master any fear we might have about death. Instead we can allow ourselves to return to Nature.
And yet, talking and writing about death constantly is an approach towards our own mortality that often seems completely alien to modern Western cultures. (Eastern cultures are way ahead and can be looked to as an example.) Nowadays it’s relatively rare to engage in an open conversation with friends or family about how we want to be buried, or what happens to the soul after we die. Often these discussions are relegated to funerals or college philosophy tutorials, or they simply don’t happen at all. But Montaigne states time and again that such avoidance is unhealthy and impractical; instead he declares “let us have nothing so much in minde as death” and regularly draws on ancient philosophy to back up his ideas on confronting death head-on. For example, he uses the Stoic philosophy of the Roman emperor Marcus Aurelius (26 AD — 180 AD) to argue that we should relish spending our leisure time in contemplating the meaning of death. Like Montaigne, I believe it is possible to gain a huge degree of contentment from life through attempting to understand death. As well as feeling closer to Nature, death encourages a greater awareness and enjoyment of the present moment. In a strange way, acknowledging that death is certain actually allows us to adopt a more practical attitude towards the time that we do have on Earth. In her book Natural Causes: An Epidemic of Wellness, the Certainty of Dying, and Killing Ourselves to Live Longer, Barbara Ehrenreich encourages us to appreciate life “as a brief opportunity to observe and interact with the living, ever-surprising world around us.” Personally, I’ve found myself feeling extremely grateful during times that I have experienced intense happiness, as well as reaching an understanding during periods of sadness that — like everything else — this too shall pass.
By way of contrast, the death-defying attitude of Silicon Valley in recent years provides an interesting case study in 21st-century conversations about mortality. Rather than acknowledging death, a growing number of tech giants are now actively trying to eradicate it. Social commentators argue that modern society is sometimes guilty of believing in its own immutability, as though certain scientific and technological advances give human beings an absolute right to live on forever. Indeed, the cycle of Nature that I described at the beginning of this essay is currently being overturned in order to make way for advances in 3D organ printing, nanobots that can replicate immune systems and even blood injections that supposedly extend our lives. Peter Thiel, one of the co-founders of PayPal, has admitted that he is ‘against’ the idea of death and aims to fight it rather than accept it. The National Academy of Medicine is currently running a “Grand Challenge in Healthy Longevity” which will award $25,000,000 to anyone who can make a major scientific breakthrough in delaying the aging process. Many of the project’s investors want aging to be stopped completely. Meanwhile, Google’s highly secretive Immortality Project was launched in 2014 and aims to treat aging as a disease that can be cured.
There is a distinct air of confidence surrounding these endeavors; for many tech giants it is not a matter of if immortality can be achieved, it is simply a matter of when. Speaking to Tad Friend of The New Yorker, Arram Sabeti of the food tech start-up ZeroCrater once stated, “The proposition that we can live forever is obvious. It doesn’t violate the laws of physics, so we will achieve it.” The “we” in this context is questionable, since many of these projects are being supported by tech giants and celebrities who will undoubtedly be the only people able to afford an immortality cure if it ever becomes available in the future. These advances are being energetically pursued by people who head up large corporations with arguably little thought or respect for death itself, only the right to continue existing. This isn’t accepting death or preparing for it, this is trying to abolish it in the unhealthiest way possible — surrounded by secrecy, with little thought for the long-term effects on society. Such measures do nothing to cure fear of death, they only try to stop it at all costs, which is really just a form of denial.
What would the author of the Essais have made of these developments? Montaigne was famously suspicious of doctors during a time when modern medicine simply didn’t exist. He often complained that doctors were desecrating the natural duration of the human body and interfering with what he considered to be Nature’s work. Even in an age before painkillers or anesthesia, Montaigne (who famously suffered from excruciating kidney stones) was proud of his ability to withstand illnesses and diseases ‘naturally’: “We are subject to grow aged, to become weake and to fall sicke in spight of all medicine.” Therefore it’s very hard to describe the horror Montaigne would have felt upon being confronted with the idea of death-defying technological advancements such as nanobots and 3D organ printing. Not only are these inventions a human attempt to subvert death by artificial means, they also pose other problems too. For millennia, one of the most positive aspects of death originally proposed by Stoic philosophy (and later adopted by thinkers such as Montaigne) was the idea that death comes for everyone. In other words, it doesn’t care about social class — the rich human being dies just like the poor human being and thus reminds us that deep down we are all equals. Will that be true in the future as well or not? Cryogenic preservation is becoming more and more popular, but it currently costs as much as $200,000 to freeze the entire body. We have to imagine that a drug or injection to cure mortality will be ten times as costly. This means that immortality will most likely be for the few, not the many.
So what can we as human beings do to respond to death in a practical and healthy manner? Alongside the popular take-up of meditation and mindfulness (which psychologists have already noted can greatly improve our attitude towards death), a younger generation of advocates — most notably Caitlin Doughty — are heading up an increasingly popular “death-positive” movement. This trend encourages an enquiring approach towards death and funerary practices that draws on the type of calm, reasoned manner that Montaigne would have been proud of. Doughty’s website, The Order of the Good Death, states that the death-positive movement believes that “the culture of silence surrounding death should be broken through discussion, gathering art, innovation and scholarship.” This mission resounds with the philosophy of Seneca the Younger (4 BC — 65 AD), a thinker Montaigne turned to repeatedly when he wanted to understand fear of death. Seneca believed that approaching death through contemplation, mindfulness and discussion was one of the key virtues of wisdom; pursuing such an open and honest attitude towards death would eventually allow an individual to patiently wait for death, as one of nature’s operations. Therefore talking about death, studying philosophy, meditating, and even creating or appreciating art around this theme are all excellent ways to prepare for life’s end.
Talking about death, studying philosophy, meditating, and even creating or appreciating art around this theme are all excellent ways to prepare for life’s end.
We can also make sure to engage in practical preparations surrounding our funeral arrangements, wills and life insurance. Rather than becoming a depressing chore, instead we can appreciate that it brings peace of mind to family and friends, as well as ourselves. If we’re lucky enough to be dying in a bed somewhere, surrounded by loved ones, at least we can rest assured that these same people have been taken care of. In the Essays Montaigne praises the practical act of constructing your own grave — many of his friends prepared elaborate tombs, sometimes with their own death masks attached. Montaigne says that looking on a replica of your own dead face is an excellent way to prepare for the inevitable reality of the future and also shows you have taken the time to leave the world in an organized way. Incidentally, this is just one example which demonstrates that in the past, Europeans were far more attentive to the idea of preparing for death in a practical manner. Admittedly this may have something to do with the fact that death was far more visible in everyday life thanks to mass graves and public executions, not to mention the high rates of mortality, particularly amongst infants. Thankfully all of these things are in the past, but death still lingers in society, it’s just slightly more hidden away than it used to be. Whilst we can’t all afford a good death mask, it would be comforting to see a resurgence in openly discussing or enacting any kind of practical preparation for death, an attitude which has clearly been written out of European society in the last few hundred years.
In the Essays, death is natural. It forces us to realize our humble place in the great cycle of mutability that constitutes the workings of Nature. In the meantime, talking, writing and thinking about death can radically improve our quality of life by helping us to gain a greater enjoyment out of our time as one of the living, as well as helping those people we will eventually leave behind. I don’t want to start investing in cryogenics or constructing my own coffin just yet, but talking about death from time to time? That’s something we can all start doing right now.
In a pivotal scene of the documentary End Game, we listen in as a team of palliative care professionals discusses Mitra, a 45-year-old woman who is dying of cancer. Should they approach her about hospice? The hospital chaplain urges the group not to bring it up. She had spoken to Mitra’s mother, who told the chaplain that to Mitra, hospice means death. Dr. Steven Pantilat, a palliative care specialist, agrees with her assessment, noting: “Healthy people want to talk about how they want to die. Sick people want to live.”
This exchange in End Game (available on Netflix) captures human nature, and the delicate dilemma doctors and patients face at the end of life, under the best circumstances. Filmed in the serene hospital rooms and corridors of the University of California San Francisco Medical Center and the recently-closed Zen Hospice Project, situated in a tastefully-appointed Victorian house, we see firsthand the inner workings of hospice and palliative care.
We also see clearly how important it is to talk about these matters before we might need them.
Considering Palliative and Hospice Care
Though palliative and hospice care can greatly ease suffering, they are not easy to talk about or decide on for many patients. Some of the people in the 40-minute documentary are not ready to check out and seem to feel that accepting hospice care would mean accepting death. Their family members don’t want to let them go either.
Mitra’s husband hopes each new treatment will bring a miraculous recovery. Her mother knows her daughter will never walk again, much less recover from cancer and thinks her daughter is suffering. In one scene early in the movie, which is doubtless replicated in many hospital rooms every day, Pantilat asks Mitra’s husband and mother if they want to continue treating the cancer.
“If she were clear in her thinking and seeing herself in her bed the way she is right now, what decision would she make?” Pantilat asks. The question hovers in the air.
When Mitra’s sister flies in from Switzerland, initially there is jubilation over the reunion and we rejoice vicariously with the family. In the next scene, however, we see the sister collapsing in her mother’s arms in the hallway, weeping. Later, we see Mitra’s mother literally staggering down the hallway under the weight of her sorrow. We witness Mitra’s husband’s heart breaking, and their 8-year-old son playfully massaging his mother’s bald head.
There is joy, sorrow, love. The camera captures it all, but there is no narration. We witness the family’s struggles as they go through them in real time. This is part of the film’s power: It is easy to identify with the subjects. Viewers might feel they are losing their own family member.
The Filmmakers’ Vision: Bring Death Out of the Closet
The 40-minute film, directed by Rob Epstein and Jeffrey Friedman, was nominated for an Oscar in the category of Documentary Shorts.
The filmmakers, who won an Oscar in 1985 forThe Times of Harvey Milk, wanted to raise awareness about how palliative and hospice care can give us the right care at the right time. As Friedman explained, birth and death are universal life passages, and of those, death is the one we have the option of facing consciously.
“Most of us avoid thinking about it until it’s too late. By doing that, we set ourselves up to lose control of our life story when we’re at our most vulnerable,” Friedman says. “Couple that with medical technology so advanced that we can keep nearly everyone ‘alive’ using machines — but without taking the time to talk about what the quality of that life will be. The result is that far too many people are getting care they don’t understand and don’t want.”
“End Game is about choices we make about how we want to live, when we know our time remaining will be brief,” Epstein adds. “One of our goals in End Game was to inspire conversations — not only about facing death, but about how we want to live, right up to the end.”
End-of-Life Care Explained
According to Pantilat, author of Life after the Diagnosis: Expert Advice on Living Well with Serious Illness for Patients and Caregivers, “Palliative care focuses on improving the quality of life for people with serious illness (whatever the prognosis). It alleviates symptoms like pain, shortness of breath, fatigue and nausea. It’s also about having patients communicate preferences and values, so the care team can attend to their psychological, spiritual and emotional support when they are sick.”
In the United States, hospice is a service to provide palliative care to people, largely at home. For hospice, the eligibility criteria include a prognosis of no more than six months of life and patients and loved ones who have agreed the focus will be comfort care. Hospitalization, generally, will be avoided.
“Most of the time, hospice is not a place, but a service, although there are facilities focused only on hospice care (as Zen Hospice Project was). All hospice is palliative care, but not all palliative care is hospice,” Pantilat explains.
Many people have the misconception that once you choose palliative care, you’re not getting any other treatment for your illness. “That’s not true at all,” Pantilat says. You could have palliative care alongside chemotherapy, bone marrow transplant and many other serious illnesses. In fact, palliative care might help you live longer.
“There’s never been a study that showed that people who receive palliative care live less long. And there are studies that show that people who receive [palliative care] for the illness live longer. It’s an unmitigated good.” Pantilat says.
Help for the Family, Too
There’s another important feature of palliative care: It also attends to a dying person’s loved ones. The palliative care team will talk to family members and offer them comfort, options and counsel.
Pantilat notes: “When people ask, ‘When should my family come?’ I always say come now. If they get better and live for another six months or year or two, no harm, no foul. It’s one more visit. But if you try to time it when they’re really sick and on death’s door, they might be too sick to have a meaningful interaction or you might miss the opportunity. Things can happen suddenly.
“We try to have these conversations in advance and understand what’s really important,” Pantilat continues. “If visiting with your sister or seeing your daughter get married is the most important thing to you, now’s the time to do it. Maybe you shouldn’t wait 10 months for a wedding, because you may not make it. Instead, could your daughter move the wedding up to next month?”
And speaking of not waiting, the doctor has a message: “If you or a loved one has a serious illness, you should have palliative care. Don’t take no for an answer. Because it will help you live better and may even help you live longer.”
This year marks the 200th anniversary of Walt Whitman‘s birth. To celebrate, the New York Public Library and the Grolier Club are hosting exhibits, both of which will include samples of Whitman’s actual hair. Yes, hair.
In the Victorian era, jewelry made with hair was all the rage. In 1854, the novelist Wilkie Collins wrote that bracelets made of human hair were “in England one of the commonest ornaments of woman’s wear.” Ten years later, Charles Dickens wrote that a man’s watch fob made of hair was the real mark of middle-class respectability.
Victorians on both sides of the Atlantic were particularly mesmerized by the hair of the dead. Victorian literature scholar Deborah Lutz explores “the materiality of death and its artifacts” of the era, finding antecedents in the Christian reliquary tradition, when body parts of saints were considered magical. Protestantism and secularization shifted this fascination toward the sought-after body parts of royals and the very famous (like Napoleon, whose penis is supposedly now in New Jersey). By the middle of the nineteenth century, this long Western tradition had become “increasingly secular, personal, and private.” And concentrated on hair.
Loved ones and relatives could give hair as tokens of love and friendship. Family members or lovers could twine their hair together. After a person’s death, their hair remained; as the Whitman exhibits show, well-preserved hair can last a long time. Hair was a tangible keepsake of a life, and of a body. Perhaps it imparted a sense that you might meet again.
Lutz writes that such relics “work as traces of a life and body completed and disappeared, in this sense something like last words, by they also serve as frames or fragments of the moment of loss.” These present reminders of those who have died speak of a “desire to see death as not permanent, in that material remains might be proof that the loved one still exists somewhere, somehow.” Relic worship also shows a willingness “to dwell in and with the moment of loss itself, to linger over this evidence of death’s presence woven into the texture of life at all turns.”
Romanticism, the Evangelical revival of the 1830s-40s, and Spiritualism’s rise in the 1850s-1860s, all contributed to this “after-death narrative” and the mid-century popularity of “hairwork.”
Lutz reminds us of the passage in Emily Brontë’s Wuthering Heights (1847) when Heathcliff switches his rival Linton’s hair from the locket around the dead Catherine’s neck and replaces it with his own. “Rather than gathering a memento of Catherine for himself, Heathcliff sees to it that a material fragment of his body will go down into the grave with Catherine’s corpse, to intermingle with her flesh.” The notion of the “good death” merges here with the palpable eroticization of death. Of course, Heathcliff’s plans are foiled by Nelly Dean, who twines Linton’s lock around Heathcliff’s—opening “the possibility of a postmortem storm of jealousy.”
Fiction mirrored the times. After her husband’s death in 1861, Queen Victoria had at least eight pieces of jewelry made that incorporated Prince Albert’s hair. The Victorians “found in relic culture a means to respect the irreducible self.” Such a culture, Lutz says, “sees death, and the body itself, as the beginning of stories, not their end.”
“Everyone knows loss in one way or another. This song is about that,” Marcus Mumford says of Delta track
A young boy watches over his dying mother and fantasizes about better times with her in the video for Mumford and Sons’ new Delta single “Beloved.” The son and mother, who’s still wearing a hospital gown, run around, go shoplifting and ride horses on a beach. “Before you leave, you must know you are beloved,” Marcus Mumford sings against a serene backdrop of synths and guitars, “and before you leave, remember I was with you.” It all builds to an emotional finale.
“Everyone knows loss in one way or another,” Marcus Mumford said in a statement. “This song is about that. I’d never sat with anyone as they died before, and it had an effect on me. As it does everyone I know who has experienced it. But there’s wildness and beauty in it as well, and a deep honoring, that became the beginnings of this song that we worked up called ‘Beloved.’ I feel determined for people to take whatever they want from it, and not to be emotionally prescriptive.”