“The Good Death” by Ann Neumann. Cover photo courtesy of Beacon Press
“Religion is most prevalent around the deathbed in our country,” Neumann, 47, said in a phone interview from her home in Brooklyn, N.Y. “That is where it is resoundingly proven that we are not a secular nation.”
“The laws, medical practices and corporate regulations that surround death and dying continue to be strongly influenced by religion, whether it is in the delivery of health care through Catholic hospitals, whether it is in the rituals that medical practice is infused with, or whether it is simply in the language that we find acceptable around the dying.”
If “The Good Death” is anything, it is a call for people to examine their own wishes around end-of-life issues and decide what role religion — either theirs or that of their caregivers — will play. Religion, she holds, influences our ideas of quality of life and how far we are willing to go to preserve it.
Neumann has spent time around the dying. Her first up-close experience as a caregiver was with her father’s difficult, drawn-out death from cancer that left her worn-out and overwrought.
In the aftermath, unmoored by her own grief and seeking a way to cope with the death she knew would someday come for her and her loved ones, she decided in 2007 to become a hospice volunteer. Her descriptions of her visits with her patients are among the most moving in the book.
Newmann, reared a Mennonite and now a Catholic, looks at how quality of life is often sacrificed for sanctity of life, often for religious reasons, by health care providers, families and religious leaders.
“We must examine the inequality and the discrimination that the church has built into its position on health care,” she said. “The Catholic Church is so good at managing hospitals, at addressing patient care that we cannot say it is bad on the whole and yet the discrimination against women, the lack of autonomy provided to elders or to individuals like to Terry Schiavo — these families that are put in these difficult positions should be supported by their church. They should be able to make their own decisions.”
Ann Neumann is a visiting scholar at the Center for Religion and Media at New York University, where she is a contributing editor to the Revealer. Her articles have appeared in the New York Times, Bookforum, the Nation, and Guernica. This is her first book.
But what about hope? In the book, Neumann echoes the writing of Adrienne Martin, a professor at the University of Pennsylvania, who writes that hope is not always a good thing. It can lead to pain and suffering, both physical and emotional, and result in stretching out an illness in the hope for an unlikely positive outcome.
“It was an area of research that fascinated me because it did question the hands-down understanding we have that hope is always good,” Neumann said. “Hope can be sustaining. It can get us out of bed. But it can also result in the very painful treatment of patients and lead to denial.”
What’s a country with a rapidly aging population to do? The U.S. Census Bureau predicts that by 2050, one in five Americans will be 65 or older and have diverse ideas about end-of-life issues. A Pew Forum survey in 2013 found two-thirds of Americans believe there are some situations in which patients should have a right to end their own lives, while 31 percent say doctors should do everything they can to prolong life.
Start conversations with your loved ones, make your end-of-life wishes clear and know your rights, Neumann said.
“A good death is whatever a patient wants,” Neumann said. “It is not up to me, to their legislators, to their priests, to their families. That is true informed consent. A good enough death is as close as we can get because humans are not perfect. We can get so much closer, but we will never have a perfect death.”
Jon Henley with his father, mother and son in 2003
My father spent 10 days dying.
He was 84 and he had lost his wife – my mother, whom he adored, and without whom he felt life was a lot less worth living – three years earlier. He died of old age, and it was entirely natural.
The process, though, did not feel that way at all, at least not to me. Dad had been bedridden for months and was in a nursing home. He stopped eating one day, then started slipping in and out of consciousness. Soon he stopped drinking.
For 10 days my sister and I sat by his bedside, holding his hand, moistening his lips. Slowly his breathing changed, became more ragged. During the last few days, the tips of his fingers turned blue. His skin smelled different. His breath gradually became a rasp, then a rattle.
It sounded awful. We were sure he was in pain. The doctor reassured us he wasn’t; this was a human body dying naturally, shutting down, one bit at a time. We had not, of course, talked about any of this with Dad beforehand; we had no plans for this, no idea of what he might have wanted. It would have been a very difficult conversation.
The doctor said he could give him something that would make him at least sound better, but it would really be more for us than for my father. “My job,” the doctor said, “is about prolonging people’s lives. Anything I give to your father now would simply be prolonging his death.”
So we waited. When it finally came, death was quite sudden, and absolutely unmistakable. But those 10 days were hard.
Death is foreign to us now; most of us do not know what it looks, sounds and smells like. We certainly don’t like talking about it. In the early years of the 20th century, says Simon Chapman, director of policy and external affairs at the National Council for Palliative Care, 85% of people still died in their home, with their family.
By the early years of this century, fewer than 20% did. A big majority, 60%, died in hospital; 20% in care homes, like my father; 6% in hospices, like my mother. “Death became medicalised; a whole lot of taboos grew up around it,” Chapman says. “We’re trying now to break them down.”
The reports all, in fact, conclude pretty much the same thing: the need for end-of-life care that is coordinated among all the services, focused on the dying person’s needs and wishes, and delivered by competent, specially trained staff in (where possible) the place chosen by the patient – which for most people is, generally, home.
“It’s not just about the place, though that’s important and things are moving,” says Chapman: the number of people dying in hospital has now dropped below 50%.
“The quality of individual care has to be right, every time, because we only have one chance. It’s about recognising that every patient and situation is different; that communication is crucial; that both the patient and their family have to be involved. It can’t become a box-ticking exercise.”
Dying, death and bereavement need to be seen not as purely medical events, Chapman says: “It’s a truism, obviously, but the one certainty in life is that we’ll die. Everything else about our death, though, is uncertain. So we have to identify what’s important to people, and make sure it happens. Have proper conversations, and make proper plans.”
All this, he recognises, will require “a shift of resources, into the community” – and funding. Key will be the government’s response to What’s Important to Me, published last February by a seven-charity coalition and outlining exactly what was needed to provide full national choice in end-of-life care by 2020. It came with a price tag of £130m; the government is expected to respond before summer.
In the meantime, though, a lot of people – about half the roughly 480,000 who die in Britain each year – still die in hospital. And as an organisation that has long focused on curing patients, the NHS does not always have a framework for caring for the dying, Chapman says.
But in NHS hospitals too, much is changing. There has been a specialist palliative care service – as distinct from end-of-life care, which is in a sense “everyone’s business”, involving GPs, district nurses and other primary care services – at Southampton general hospital and its NHS-run hospice, Countess Mountbatten House, since 1995, says Carol Davis, lead consultant in palliative medicine and clinical end-of-life care lead.
People die in hospital essentially in five wards: emergency, respiratory, cancer, care of elderly people and intensive care, she says: “Our job is about alleviating patients’ suffering, while enabling patients and their families to make the right choices for them – working out what’s really important.”
Palliative care entails not just controlling symptoms, but looking after patients and their families and, often, difficult decisions: how likely is this patient get better? Is another operation appropriate? What would the patient want to happen now (assuming they can’t express themselves)? Has there been any kind of end-of-life planning?
Of course many patients in acute hospital care will not be able to go home to die, and some will not want to, Davis says: “Some simply can’t be cared for at home. If you need two care workers 24/7, it’s going to be hard. Others have been ill for so long, or in and out of hospital so often, they feel hospital is almost their second home. So yes, choice is good – but informed choice. The care has to be feasible.”
In 2014, the report One Chance to Get it Right [pdf] identified five priorities in end-of-life care: recognise, communicate, involve, support, and plan and do. (“Which could pretty much,” says Davis, “serve as a blueprint for all healthcare.”) The first – recognise, or diagnose – is rarely easy. How does a doctor know when a patient is starting to die?
“There are physical signs, of course,” says Davis. “Once the patient can’t move their limbs, or can no longer swallow.” But, she says, “we have patients who look well but are very ill, and others who look sick but are not. In frail elderly people – or frail young people – it can be hard to predict. Likewise, in patients with conditions like congenital heart disease, where something could happen almost at any moment.”
Quite often, Davis and her team face real doubts. “Right now,” she says, “I have a patient in intensive care, really very ill. They probably won’t pull through, but they might. I have another doing well, making excellent progress – but they’ve been in hospital for three months now. They’re very, very weak, and any sudden infection … You just can’t predict.”
Which is why communication, and planning, and involving the family – all those difficult and painful conversations that we naturally shy away from – are so very important.
It could well be, for example, that my father would actually have wanted his death to be prolonged: he certainly clung on to life with a tenacity that startled my sister and me. We will never know, though, because we didn’t talk about any of it.
“It is our responsibility – all of our responsibility – to find the person behind the patient in the bed,” Davis says. “One way or another, we have to have those conversations.”
During a car ride, Peter brought up to his two twentysomethings what his end-of-life wishes would be: No heroic measures, because he wouldn’t want to suffer and wouldn’t want his family to endure it. One of the boys took this in stride, but the other became very upset, asking: “Why are you talking about this? It’s horrible that you’re so calm about death.”
Death comes to us all, but in the 21st century, it comes later than ever for most people. Because of medical advances, life expectancy has stretched to record highs, and in the United States and other countries most people can expect to live into their 70s or 80s. Perhaps for this reason, we generally prefer to ignore death and avoid talking about it, even when we’re in our 60s or older. And our young-adult children, certain of their own immortality, may also prefer to think of their parents as living forever. Bringing up our mortality may provide a rude awakening to grown children of any age.
But we ignore it at our peril, or rather, at the peril of those we love. They may not want to hear us talk about the inevitable visit from the Grim Reaper, but if we neglect the responsibility to prepare for our death — and to prepare them for it — we do them a disservice and leave them with a stressful mess when the time comes. That’s a legacy few of us would wish.
So, here are three crucial issues to make sure you address and discuss:
1. Make a Will
You need to have a will, and once you do you need to make sure your loved ones know about it. Because we tend to prefer to think of death as many years away no matter what age we are, many of us fail to fulfill the basic responsibility of making a will. Various surveys indicate that about 50 percent of American adults have not had one drafted. The percent who have made a will rises with age, but even among 55- to 64-year-olds, 40 percent have no will.
Here’s the problem with that: If you die without a will, the state takes over your estate and makes the decisions about who gets what. Who would want that?
So, no excuses: If you haven’t prepared a will yet, do it as soon as you’re done reading this post! There are many inexpensive online options or you can hire anestate planning attorney if your estate is complex or you’d like the assurance that all the legal steps have been taken correctly.
2. Make Funeral Plans
Figure out plans for your funeral and burial or cremation and make sure family members know what ,and where, the plans are. We’re not crazy about talking about this aspect of death, either, but again, wouldn’t you rather decide on this now, rather than leaving it to your grieving family members to handle hastily after your death? You may find consolation, too, in the thought that the post-death commemoration will be done as you would have wished, even though it is a party you will not be able to attend.
3. Make Your End-of-Life Plan
You also should come up with your end-of-life plan and make sure your loved ones know about it. Medical interventions are extremely effective at keeping us alive at the end of life, even after any prospect of restoring us to consciousness, much less good health, has passed. People vary in how they view this issue, from those who want all possible steps to be taken to those who would prefer not to prolong the inevitable.
Ask your doctor how to make an “advance directive” that will contain your instructions or look up the instructions online from a reputable source like AARP or state government websites (each state has its own laws concerning end-of-life care).
Don’t assume your loved ones will know what to do; they probably won’t, and you don’t want them to have to make those decisions amid the stress and sadness of losing you.
Difficult as these conversations and plans may be, for your children’s sake and for your own peace of mind, discuss them now, while you are lucid and healthy. Your children may not thank you today, but they will appreciate the guidance when the time comes. That’s one last gift of love you can give them after you’re gone.
Greater control: Compassion in Dying said too few people are planning for how they want to be treated at the end of their lives
A website which allows people to declare how they wish to be treated in the final weeks of their lives is set to launch this week.
Compassion in Dying, a charity that supports people to exercise their rights over end-of-life treatment, said MyDecisions.org.uk will give people greater control over their death.
The group said the website was created in response to fears not enough people were planning for how they want to be treated in the advanced stages of their life.
A statement on the MyDecisions.org.uk homepage reads: “You might not like to think about it but there might come a time when you’re too unwell to tell those caring for you – like your family or a doctor – what you do and don’t want to happen.”
Anyone visiting the site can fill out an “advance decision” where users can refuse any drugs or medical treatments that may be given to them at some time in the future.
The document, also known as a living will, is legally binding meaning any healthcare professional that ignores it risks going to court.
The website also allows people to make an “advance statement” to declare preferences, wishes and beliefs for those who might have to make choices for them should they lose the capacity to make their own decisions.
According to research commissioned by the charity, only 4 per cent of Britons made a record of their preferences last year.
We did a survey in 2013 which found that “90 percent of people say that talking with their loved ones about end-of-life care is important yet only 30 percent of people actually have done so.” Clearly, knowing the importance of a conversation or behavior doesn’t always mean we’ll do it. How many diets and half-marathon training programs have begun in this vein? We know all the excuses a person is likely to tell themselves to avoid the conversation. Any of these look familiar?
“I know my loved one well enough to make the right call.”
There are plenty of reasons to have the conversation with your loved one beyond your belief that you know what they would want. Having a specific conversation about they would prefer could bolster your confidence, strengthen their trust and reward you with a new sense of intimacy. The conversation could really surprise you. You might discover something about your loved one that you never expected.
“I don’t need to have the conversation. I’m healthy and young.”
The Conversation Project is an initiative to encourage people to have these conversations before they are sick or terminal. If you’re healthy and well, it’s the perfect time to have the conversation. As we say, it’s always too soon, until it’s too late.
“If my loved one wants to have a conversation, they can come to me.”
This excuse is extremely powerful. It allows you to believe you’re up for the conversation while simultaneously avoiding it.. Don’t fall victim to this one. Your loved one might be thinking the same thing, trapping you both in a game of chicken, in which neither of you have important conversations about your health, your finances and your future because you’re waiting for the other to initiate it.
“I’ll just decide based off what I would want.”
This excuse provides false comfort. No need to have the conversation because you know what you would do for yourself. Right? But this method of avoidance leads to an improbable and unrealistic scenario. Even if you are the designated health care proxy that doesn’t mean you’ll be the only one who cares about the outcome. You might find yourself having to explain your choices to other family members, friends and caretakers. This might open up a disagreement between family and loved ones who believe the person in question wouldn’t want that. And you’d be surprised how many decisions you might have to make. Imagine what happens when you need to make a decision and you don’t know what you would want.
“It makes me uncomfortable.”
The thought of having The Conversation can make a lot of people uncomfortable. Understandably. You do have the right to live your life with minimal discomfort, but consider this: we’ve heard from a lot of people who wished they’d had the conversation, rarely those who wished they hadn’t. Knowing what a loved one prefers can give you A LOT of comfort during a time when you most desperately need it.
“I don’t want to encourage my death by talking about it.”
We work with many diverse communities of various beliefs, cultures, and faiths. Each has their own history, experience and theological lens through which they view death. Our mission is to ensure that your fears aren’t holding you back from a very real and human experience.
“I don’t want to offend my loved one.”
Death doesn’t have to be an offensive topic, and if your loved one perceives it to be so, maybe you can start the conversation there. Ask them why they find death so offensive. A simple question can lead into a complex and profound conversation.
“I don’t need that kind of negativity in my life right now.”
Having the conversation doesn’t have to lead to a negative experience. Many people who had the conversation describe it as a positive, freeing experience rather than a negative one.
“I don’t even know what my career path will be let alone what I prefer about my end-of-life care.”
If you’re in your twenties or thirties, it can be particularly difficult to focus on your end-of-life care. You’re focusing on surviving the hardship of life post-college. We know the #TheStruggleIsReal. But while it’s hard to relinquish the coziness of childhood irresponsibility, you must. Get your affairs together: start that 401K, use sunscreen, stop eating take-out every night, and have the conversation with your loved ones.
“Why do we need to have a conversation? Can’t my loved one just write everything down?”
Modern medicine is helping individuals live longer than ever before, and with that extended time on earth comes increased medical complications and a lot more decisions to be made at the end-of-life. People will often say, ‘if I am ever like that – pull the plug,’ but there is often no proverbial plug to pull. Instead, there is a number of cascading decisions left for your loved ones to make. Talking through your values with your family can give them the guidance to navigate the health care options presented to them. Questions like: “What matters most to them at the end of life?” “Do they want to be at home or in the hospital?” “Do they mind visitors?” “Who do they want to make sure is there?” “Is there a book they might want read to them?” “Do they want music playing or a ball game on in the room?” These are the questions you might find yourself considering. Conversations are organic; they are interactive. This conversation isn’t just about answering a set of medical questions, but exploring all the avenues you didn’t think were possible.
So really, what are you waiting for? Check out our Conversation Starter Kit and have the conversation today.
During the health reform debate, the Oregon congressman pushed a provision that would reimburse doctors for helping Medicare patients draw up advance care directives.
Blumenauer’s proposal quickly became the most politically toxic section of a law rife with contested projects and programs. It’s the part of Obamacare that Sarah Palin termed “death panels.” In August 2009, amidst ugly skirmishes at angry town halls, legislators relented. They left the end-of-life planning provision on the cutting-room floor.
“It was very difficult, in part because of the lingering death panel cloud”
But Blumenauer was undeterred. He quickly began lobbying the Obama administration to create the advance care benefit through regulations that Congress wouldn’t have to approve.
“It was very difficult, in part because of the lingering death panel cloud,” Blumenauer told me in a recent interview.
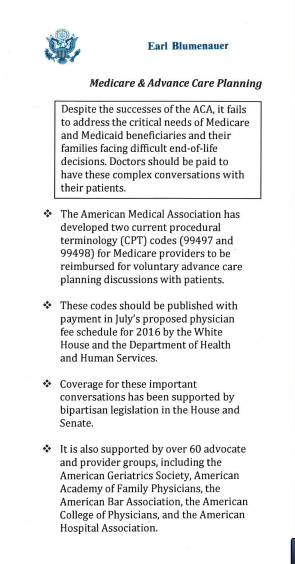
The pocket card Rep. Blumenauer would hand out to White House officials.
Since 2009, Blumenauer has doggedly — and unsuccessfully — badgered any Obama administration member who might listen to his cause. But the White House, for five years, wouldn’t budge. Every year, it would put out the list of services Medicare would reimburse. And every year, advance care planning would not be on it.
Blumenauer recalled once attending a picnic at the White House — and pestering administration officials to take small cards he’d had printed up to summarize his case.
“At this year’s White House picnic, around the Fourth of July, there was some indications it could go our way,” he says.
On November 2, Blumenauer finally won: The White House finalized rules that will allow doctors to be paid for every discussion they have with patients about creating an advance directive.
The United States has — quietly and with little fanfare — begun to do something quite remarkable. We’ve started to have a more sane conversation about death, something that just this spring, as I wrote in a lengthy essay, seemed near impossible. That has allowed for significant policy changes that will, starting in 2016, begin to revamp the way Americans plan for the inevitable.
I’ve spent much of the past month asking legislators, doctors, government officials, and advocates about how that happened. They say health care became a much less heated topic. Doctors and patients, meanwhile, began to take a bigger leadership role. And the White House, cognizant of Obama nearing the end of its term, appeared to see a last moment for action — and decided to seize it.
“As a country, we’re more willing to have a conversation around the end of life,” says Kim Callinan, chief program officer for the end-of-life advocacy group Compassion and Choices.
Medicare spends billions on end-of-life care. But patients aren’t getting the care they want.
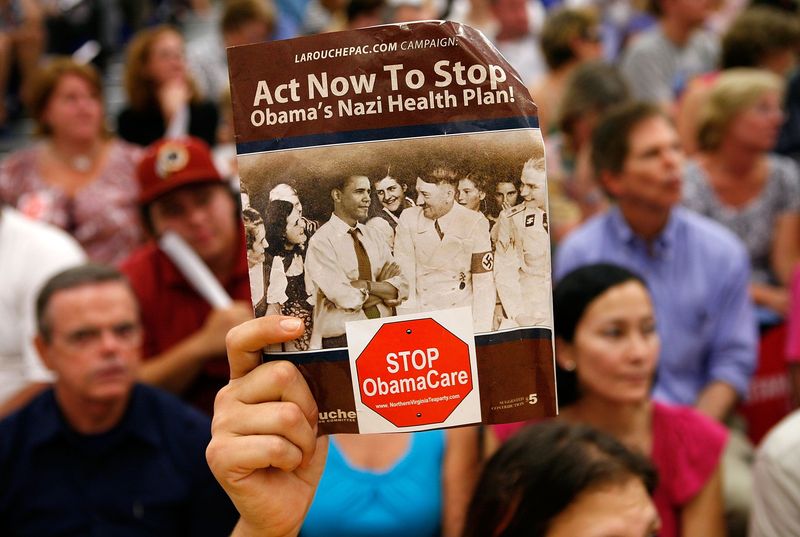
Fierce protests over end-of-life care broke out at 2009 congressional town hall meetings.
Dying in America is expensive. The 6 percent of Medicare patients who die each year typically account for 27 to 30 percent of the program’s annual health care spending. Medicare spent an average of $33,500 for beneficiaries who died in 2011 — four times the amount it spent on the seniors who lived.
Health care providers often make heroic efforts to save patients’ lives in their final days and weeks. The average Medicare patient who dies from cancer spends 5.1 days of his or her last month of life in the hospital. A quarter of these cancer patients are admitted to the intensive care unit over the same time period.
But surveys of patients with terminal disease suggest this isn’t what they actually want. One survey of 126 patients facing near death found they had five priorities at the end of life — and prolonging life was not actually among them.
Patients told researchers they wanted their pain controlled, a sense of control over their care, their burdens relieved, and time to strengthen relationships with loved ones. They also specifically did not want the “inappropriate prolongation of dying.”
A 2012 paper found that cancer patients who have less intensive care at the end of life — who have fewer hospitalizations and intensive care unit visits in their last week of life — report the best quality of life at the time of death.
In Washington, something so costly that leads to worse patient outcomes would be, in other public health programs, a no-brainer. But with end-of-life care, the opposite tends to be true: We can’t talk about the cost of dying because it sounds like a discussion about rationing. Taking cost into account feels callous and inappropriate in the context of death. For years now, that’s made end-of-life care an unapproachable topic on Capitol Hill.
That the already-polarizing health reform law included policy changes for end-of-life care certainly did not help matters.
“This was toxic for a while because of the gross mischaracterization of what we wanted to do,” says Sen. Mark Warner (D-VA), who has worked on end-of-life care legislation.
Warner, like many other legislators who work on the issue, had his own personal story of attempting to care a loved one — in his case, his mother, as her Alzheimer’s worsened.
“I was someone who was relatively informed; I was the governor of Virginia,” he says. “We knew something was coming, but we never had the conversation within our family that we needed to. This is an issue that has touched every family, and touched all the ups and downs of the health care debate.”
How 2015 changed the way America talks about death
The first two attempts to pay doctors to talk about death started in Washington. And both were abject failures.
The first attempt touched off the “death panel” outcry during the summer of 2009.
The second came in the winter of 2010, when the Obama administration tried quietly slipping the new benefit into regulations that outline how much Medicare doctors get paid for various procedures. That approach seemed to work — until an eagle-eyed New York Times reporter noticed the regulatory bombshell and wrote a story for the paper’s front page. Within days, the Obama administration retreated.
“We were, to put it mildly, disappointed when the administration changed course at the end of 2010,” says Blumenauer. “Any poor soul who happened to be the secretary of Health and Human Services or high ranking at the Center for Medicare Services has heard from me about it.”
Any federal proposal to change the way Americans die was met with immediate skepticism and framed as a government takeover of health care.
This last successful attempt didn’t start in the White House. It didn’t even begin in Washington. It began far outside the Beltway, at the 2012 meeting of the Illinois State Medical Society.
That’s where two doctors from the DuPage Medical Society — which covers the county just west of Chicago — brought to the floor a resolution to ask the American Medical Society to create a billing code for advance care planning discussions. Somewhat confusingly, the AMA creates all the billing codes that Medicare uses, while the government decides how much to pay for each code.
“This was the voice of doctors saying, ‘We want this,'” says Scott Cooper, executive director of the Illinois Medical Society. “Because it came from physicians and was based on clinical experience, and not some policy wonk who had some idea in Washington. It’s an easier sell when you have the voice of the medical community.”
The resolution passed — and a handful of Illinois State Medical Society members flew to an AMA meeting in 2013 to deliver their request in person. They were successful, and the AMA created two codes.
“It’s not every day you just create a new procedure for Medicare,” says Cooper. “We’d never done it before. But this was relatively seamless and easy. It didn’t face any pushback.”
After that 2013 meeting, the billing codes existed — but Medicare never attached any money to them. If a doctor had tried to bill for an end-of-life planning discussion, no reimbursement would show up. Advocates pushed delicately on the issue, knowing that Medicare was a massive agency they had to work with on countless other issues.
“It’s not every day you just create a new procedure for Medicare”
“You don’t want to be put in this awkward position of pushing too hard against an administration or executive branch that has largely been doing many positive things,” says Peter Hollmann, a board member of the American Geriatric Society and a practicing physician in Rhode Island.
Medicare sat on the codes for two years. But in early 2015, rumors started to ripple through Washington’s health policy circles: This would be the year that Medicare started paying for end-of-life discussions.
The timing made sense: This was, arguably, the last moment the Obama administration had to create the benefit. If the administration waited until 2016, it would be making the change mere days before the presidential election — a risky time for any policy change. Late 2015 appeared to be the Obama administration’s last shot.
“People felt this was the last chance to do this,” Hollmann says. “No one knows what can happen in an election year, with the potential for shenanigans.”
On July 8, Medicare published draft plans to pay doctors to talk about death (about $80 for the first 30 minutes, and another $75 for an additional half-hour). The agency invited comments, which came back near universally positive.
“I am a healthcare professional in palliative care and advance care planning is critical to patients and their loved ones,” one doctor from California wrote in.
“Patients and families deserve to have realistic information provided by their doctors, rather than relying on their assumptions often fed by the popular media about what ‘life support’ and ‘rehabilitation’ can actually look like,” another in Oregon commented.
“Please add the codes below,” another Tennessee doctor requested, “so end-of-life suffering can be minimized.”
There was no outcry, and no doctors objecting to the new Medicare benefit. On October 30, Medicare made the decision official: Beginning in January 2016, it would pay doctors to talk about death.
“It’s a terrible, terrible way to die”
Brittany Maynard on her wedding day.
Much like in Washington, bills that changed end-of-life policy never had much luck in California before.
Advocates there, however, wanted to go much further: They had pushed legislation that would allow doctors to prescribe lethal medication to terminally ill patients — in other words, physician-assisted suicide.
But efforts failed in 2005 and 2007, as the California legislature rejected the proposal. Only small, decidedly liberal states like Vermont and Oregon seemed willing to pass those laws.
That all changed with Brittany Maynard, a 29-year-old who died in late 2014 from a rare brain cancer called glioblastoma multiforme. It’s a fatal disease that typically causes massive cognitive decline in the last months of lives. Patients can become unable to remember their own last names or to distinguish between a trash can and a toilet.
“My glioblastoma is going to kill me, and that’s out of my control,” Maynard told Peopleat the time. “I’ve discussed with many experts how I would die from it, and it’s a terrible, terrible way to die.”
Maynard looked at that future and made a firm decision against. She moved to neighboring Oregon, which allows doctors to prescribe lethal medications to terminally ill patients like her. Maynard used that law to take her own life on October 30, 2014.
Before her death, Maynard also recorded a series of videos imploring California’s legislature to pass a similar law — which would allow other Californians to choose the same death without moving hundreds of miles north. She recorded testimony that was presented to the legislature in March 2015 — five months after her death.
“Brittany helped normalize the discussion around end-of-life care,” says Kim Callinan of Compassion and Choices. “Here was this beautiful 29-year-old woman whom we could really relate to. Her coming forward helped transform the conversation that was taking place already, and raised the issue’s visibility.”
Compassion and Changes ran its largest-ever campaign for a state bill, putting a half-dozen organizers on the ground throughout the state. It had a watershed moment when the California Medical Association, which had opposed previous aid-in-dying bills, agreed not to take a stance on the new legislation.
Maynard’s illness caused the group to “start taking a look at our historical positions,” California Medical Association spokesperson Molly Weedn told me over email. “The decision was made to remove any policy that we had on the books that outright opposed aid in dying. We wanted to ensure that it was a decision made between a physician and their patient and determined around individual instances.
On October 5 — 340 days after Maynard’s death — California Gov. Jerry Brown signed Assembly Bill 12 into law. In one fell swoop, Brown tripled the number of Americans who live in states where doctors can prescribe lethal medications to patients whom they expect to live six or fewer months. In his signing statement, he cited the letters he’d read from Brittany Maynard’s family.
“I do not know what I would do if I were dying in prolonged and excruciating pain,” Brown wrote. “I am certain, however, that it would be a comfort to be able to consider the options afforded by that bill. And I won’t deny that right to others.”
A saner approach to death in 2016?
In some ways, the 2015 changes to end-of-life policy in America were large. Medicare didn’t pay doctors to talk about death. Now it does. This year, 13.7 million people live in places where it’s legal for physicians to help terminally ill patients end their lives. Next year, that number will jump to 52.2 million people.
But in other ways, these changes are still quite small. Data from Oregon suggests that the number of people who use the California law, for example, will be relatively small. And advocates for end-of-life care planning see much work to do when it comes to ensuring that Americans’ preferences for care at the end of life are met.
Lee Goldberg directs Pew Charitable Trusts’ improving end-of-life care project, and he sees the new Medicare benefit as a first step rather than an end goal. There’s work to be done to ensure that doctors are equipped to have these conversations — and that patient preferences that do get recorded are easily accessible when patients have emergency situations.
“The odds are no better than chance right now, so that’s a big challenge, making sure this patient data is available when it’s needed,” he says.
Goldberg and others see 2015 as something akin to a proof of concept: proof that the American political system and state governments can pursue changes to end-of-life care policy without getting shouted down about death panels and rationing. This doesn’t guarantee future change but at least allows for the possibility. Because in 2015, it wasn’t impossible for Blumenauer to get the administration to pay attention to his pocket cards.
“It does wear you down sometimes,” he says of sticking with the issue for so long and seeing so little progress until now. “How many times do you answer the same questions on something that seems so compelling, and every year have the answer be no? But every year the case became stronger, and that’s more difficult to say no to.”
We all know the cost of care at the end of life (EOL) tends to be needlessly wasteful. And we know that, too often, the wishes of patients are ignored, or worse, unknown. As the healthcare system adopts a patient-centered approach, it is important we ask every dying patient and their family what they want. When we do, we find that most would say they want less care and more quality of life in their final days. This is especially pressing today for three reasons
1. There is heightened emphasis on palliative and EOL care, in part, because of Institute of Medicine’s report last year, Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life1. In it, experts on death and dying made bold recommendations about how hospitals and healthcare professionals should address palliative and EOL care.
2. Officials from the federal Centers for Medicare & Medicaid Services, Baltimore, said, in July, it would pay physicians to conduct EOL counseling and start a pilot project to pay for hospice care and treatment instead of one or the other. At the end of the four-year project, CMS will evaluate whether it’s better to continue the current form of reimbursement or pay for both.
In this new program, 150,000 dying patients on Medicare will be allowed to choose hospice care to manage pain and suffering, get EOL counseling and medical treatments – including hospitalization – to help them battle illnesses, according to The New York Times2. Research shows that patients, who get palliative care and traditional medical care, have better quality of life and less intense medical care, resulting in lower costs, the newspaper reported.
It’s likely that CMS officials know that providing appropriate care for dying Medicare patients could control some of the steep EOL costs when the healthcare system does what it normally does: provide heroic measures to keep patients alive whether they want or need that.
In a study published in Health Affairs3, researchers at the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai, New York, showed considerable savings when patients with terminal illness are enrolled early in palliative and EOL care programs.
If 1,000 Medicare beneficiaries are enrolled in hospice within 15 to 30 days before death, CMS could save more than $6.4 million and those patients would be spared 4,100 hospital days. If 1,000 dying Medicare patients enrolled in hospice within 53 to 105 days before death, the savings would be more than $2.5 million, adds the study.
3. Brittany Maynard put the importance of end of life care into the news last year. The 29-year-old newly married teacher and resident of California became interested in assisted suicide after her diagnosis with terminal brain cancer in 2013. Under California law, this option wasn’t available. So, she and her husband rented a home in Oregon, which allows assisted suicide. A year later, at least 13 states are pursuing what is called “death with dignity” legislation. Oregon, only Montana, New Mexico, Vermont, and Washington State currently have such laws.
Given these significant developments, it may be more important than ever for healthcare professionals to ask what patients want in terms of palliative and EOL care. When we fail to ask, we are, by definition, no longer providing patient-centered care. Instead, we’re doing what the healthcare system has always done: provide lots of care whether it meets patient needs or not and wasting precious resources in the process.
Fixing this problem shouldn’t be that difficult. We simply need to make sure we’re delivering patient-centered care. To do that, we need to ensure the patient and family are fully engaged in care delivery. But, as we have seen in the past, members of the care team may not be prepared to talk about death and dying. After all, most went to school to learn to care for the living and keep them alive.
Has the care team talked with the patient about what he or she wants? If there was such a conversation, was the family included? Did the care team discuss what the patient wants without the patient being present?
The patient-engagement step is easy to overlook. Healthcare providers, not trained to talk about death and dying, don’t know how to do it; or believe it’s someone else’s job. So, the first step is to ensure that someone lets the hospital or health system know what the patient wants. In many facilities, this falls to the case manager or social worker who ensures the patient gets what he or she needs from the health system.
James McGregor, MD, an expert in palliative and end of life care and senior medical director for Sutter Health, Sacramento, Calif., says, “Addressing the full spectrum of psychosocial, emotional, physical and spiritual needs helps to raise patient and family satisfaction and prolong life. Patients and family members often have questions about palliative and EOL care and need someone to answer them.”
Those who work in palliative and EOL know the value of engaging patients and their families to guide them through these difficult times, explaining an illness and planning. And, they are likely to create a more sustainable healthcare system.