California assisted suicide patients are mostly white, well-educated
Amanda Friedland, left, adjusts her friend Betsy Davis’ sash as Davis lies on a bed during her “Right To Die Party” surrounded by friends and family, in Ojai. At the end of the party, the 41-year-old woman diagnosed with ALS took a cocktail of lethal drugs and died, becoming one of the first California residents to take life-ending drugs under a new law that gave such an option to the terminally ill.
By Hattie Xu
[C]alifornia residents choosing legal assisted suicide are disproportionately white and well-educated, new figures show.
Since California’s End of Life Option Act went into effect on June 9, 2016, hundreds of terminally ill patients have weighed the decision to end their own lives.
In 2016, 111 individuals died from ingesting aid-in-dying drugs, according to the California Department of Public Health. Ninety more had been prescribed drugs but ultimately did not take them, while a total of 258 individuals had begun the end-of-life option process.
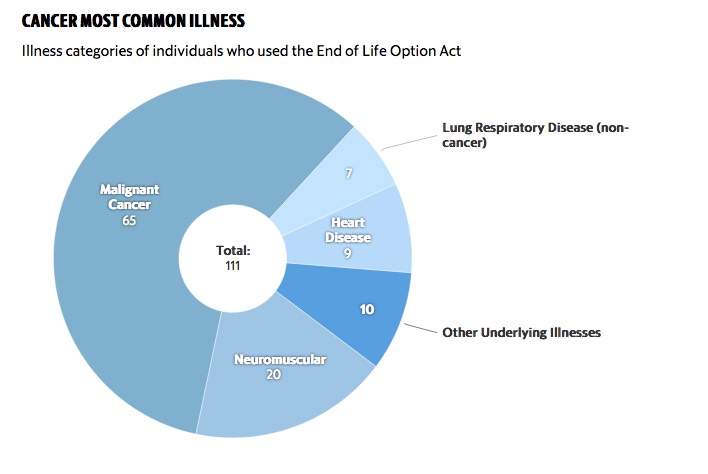
Over half of the participants had cancer, with the most common type being lung cancer. Participants also suffered from neuromuscular diseases, heart disease and non-cancer lung respiratory disease, among others. At least 84 percent were already enrolled in hospice or palliative care.
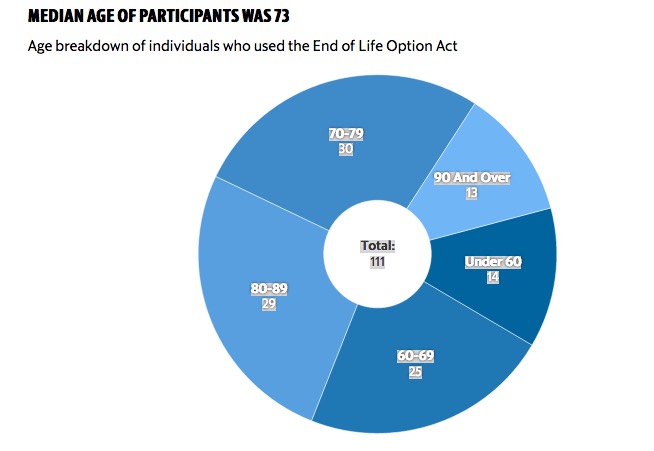
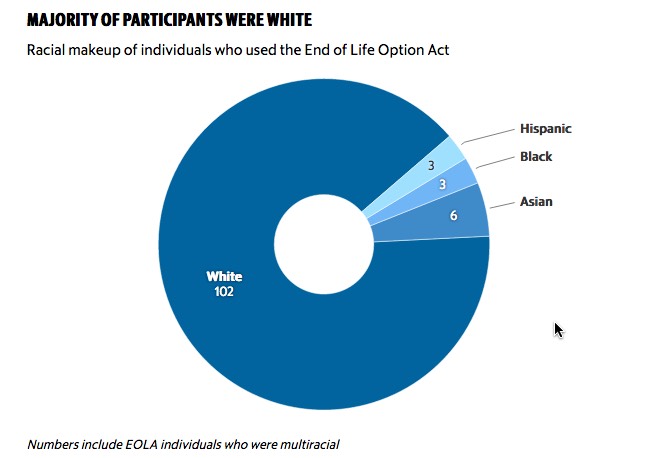
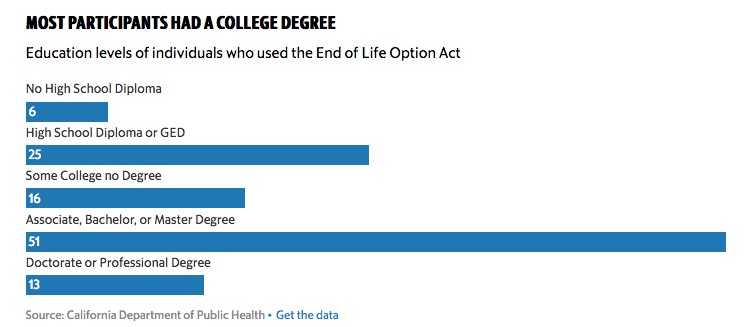
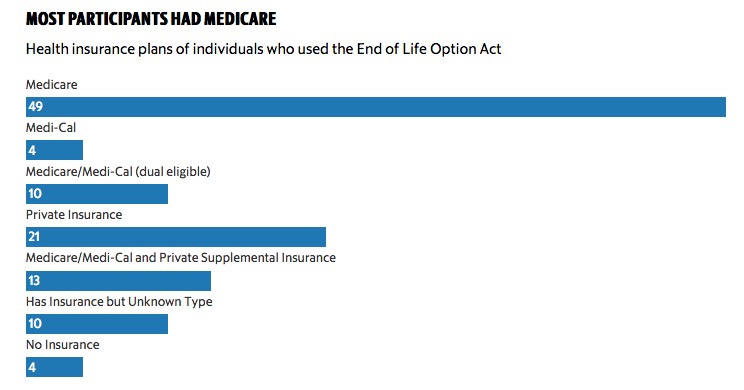
Of the 111 individuals, 87 percent were at least 60 years old and 44 percent relied solely on Medicare for health insurance. Participants were also overwhelmingly – 89 percent – white. Additionally, 58 percent had attained an associate degree or higher level of education. Highly educated whites tend to have higher household incomes.
While these proportions are similar to those in Oregon’s 2016 Death with Dignity Act report, they do not reflect the demographics of California’s population. This is a sign of a deeper sociological and anthropological cause, said Lael Duncan, medical director of consulting services for the Coalition of Compassionate Care of California, an advocacy group for quality end-of-life care.
“I suspect it has to do with cultural and community norms and higher acceptance of this practice among that demographic,” Duncan said, though she hopes future research will shed more light on the situation.
To be eligible for participation, patients must have a terminal diagnosis, defined in the bill as an “incurable and irreversible disease that has been medically confirmed and will, within reasonable medical judgment, result in death in six months,” according to the bill. They must be determined to be able to make their own medical decisions and self-administer the aid-in-dying drug.
Patients begin the process by orally requesting an aid-in-dying drug two times at least 15 days apart and submitting a written request to their doctors. After discussing alternative options for care with their attending physician, they must also consult another doctor who can confirm the terminal diagnosis and their medical decision-making capacity.
Drugs used to aid in dying have changed throughout the years as more states have authorized the procedure, Duncan said. Common prescriptions are for mixes of various drugs, such as narcotics, benzodiazepines and cardiac medications, that can be taken orally. The exact combination and dosages of these drugs are adjusted to the patient, as individual tolerances and metabolisms vary. This multi-drug regimen costs several hundred dollars depending on the drugs used. Medicare does not cover these costs, so many patients must pay out-of-pocket for the procedure.
After ingesting the drugs, patients enter a deep comatose state in roughly 15 minutes and die about 30 minutes to a few hours later, Duncan said.
Physicians are not mandated to participate in aid-in-dying, and facilities can also opt out of the practice. But a list of participating doctors does not currently exist, according to the Coalition of Compassionate Care of California’s website. Only a small proportion of all physicians in California are willing to prescribe aid-in-dying drugs, complicating patient access to the procedure, Duncan said.
“The first year, it’s been a bumpy road,” Duncan said. “Access has been incredibly challenging even for patients who are being cared for in organizations and institutions where they are participating.”