[O]ncology nurses are in the perfect position to implement ideal care for their patients via the use of the family meeting in palliative and end-of-life care. This type of meeting provides an opportunity to coordinate the responsibilities of caregivers and clinicians with patient needs, according to a study by Myra Glajchen, DSW, director of medical education, MJHS Institute for Innovation in Palliative Care, New York, and Anna Goehring, MD, palliative care physician, MJHS Hospice and Palliative Care, New York.1
Oncology nurses usually spend more time with patients than other staff and are able to answer patients’ questions about their medical conditions and discuss end-of-life issues with patients when they are ready to do so. They are also in a good position to evaluate caregivers’ condition and determine how involved caregivers want to be in helping patients make crucial decisions. These decisions are often difficult, yet Ms Glajchen and Dr Goehring write that end-of-life communication skills are not emphasized in the nursing literature.1 They note that the role of the oncology nurse in family meetings is not clear and that there has been little guidance on evaluating and managing caregiver distress.
Family caregivershave their own obligations but often bear heavy, difficult caregiving responsibilities in addition to handling their own personal concerns. Nurses can evaluate the extent to which their caregiving burdens go beyond their skills to cope and provide what their ill family member needs. Oncology nurses also are responsible for assessing the strength of the relationship between patients and their caregivers. A satisfying relationship correlates with a better commitment on the part of the caregiver, although this must be balanced with other activities to avoid caregiving becoming fraught and burdensome.
There must also be a balance with other family members; the researchers stress that a diagnosis of cancer for one family member affects the entire family. Caregivers for patients who are being actively treated for disease are in better physical and emotional health than caregivers for patients receiving palliative and end-of-life care. Oncology nurses should use family meetings to evaluate and structure caregiving situations for patients, caregivers, and their families.
The Meeting
There are a number of reasons for healthcare teams to request a family meeting. Often such meetings are about a decline in a patient’s medical condition or another change in the patient’s prognosis that requires making decisions about new treatments and different options for advance care planning. Meetings may also be called for specific purposes such as completing living wills, do not resuscitate (DNR) and do not intubate (DNI) orders, or to discuss mechanical ventilation, artificial hydration, and nutrition. The nurse’s role is key in these decisions. Oncology nurses are qualified to understand medical information, which they can easily interpret for patients and their families at these meetings. For this reason, it is important for oncology nurses to obtain and review all updated information from the patients’ clinicians prior to the meeting.
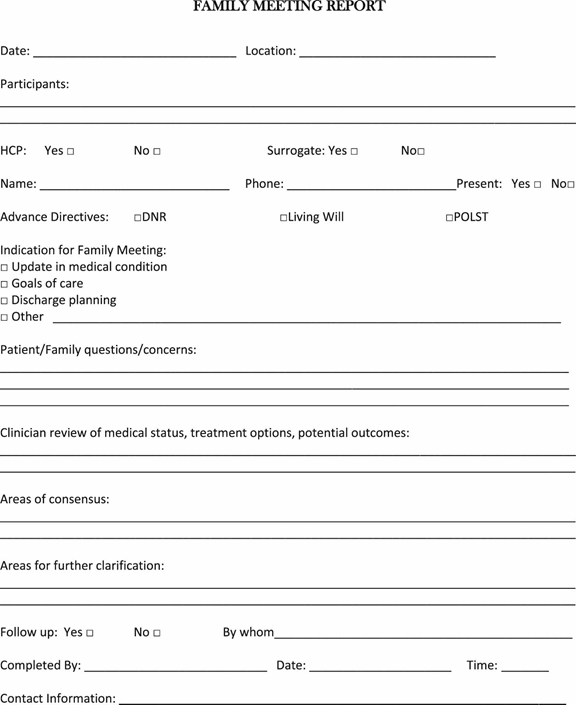
With the oncology nurse at the meeting, other clinicians only need to attend if doing serves a specific purpose.1 However, the participation of involved staff from other disciplines concerned with the patient’s care is helpful. Caregivers the healthcare team or patient wants to invite should attend the meeting, although the researchers caution there should be more caregivers than staff present so as not to overwhelm the family at this difficult time. The care team leader should explain why the meeting was called, provide a clear agenda, and should request all attendees to mute their cell phones and pagers during the meeting. A member of the healthcare team should take notes; the investigators suggested using the Family Meeting Report (Figure 1) and documenting the meeting in the electronic medical record.1
A family meeting takes time; at least an hour for preparation, an hour for the actual meeting, and half an hour to an hour for follow-up is required.1 Despite the work-intensive nature of a palliative care family meeting, the oncology nurse can be a true asset, lowering stress and offering information, realistic hope, supportive care, and comfort to patients, caregivers, and other family members.
David Wynn, 62, and Carolyn Lyon, 74, in Santa Ana, Calif., volunteer at a hospital where they accompany patients who are near death and don’t have loved ones to be with them in their final hours.
[W]hen patients are near death, and don’t have loved ones to be with them, David Wynn and Carolyn Lyon rush to the hospital.
“They have no one for various reasons, you know, they’ve outlived family, they’ve never married,” Lyon says.
For about six years, Lyon has been comforting patients in their final hours at St. Joseph Hospital in Orange, Calif.; for Wynn, it’s been about nine years.
“For some reason I always wonder about the person’s mother,” David Wynn says. “She saw him first, and I saw him last. It was her and me that are the bookends of this person’s life. So each time that I leave a patient who has died, there is this element of sadness.”
But this kind of work also has its rewards. Wynn remembers one man who was estranged from his family.
“I was sitting there with him and I heard somebody at the door. Turns out it’s his son,” Wynn says. “And he, I guess, felt a little bit uncomfortable, and so he asked me to stay.”
Then, the patient’s daughter came in. “These are people who hadn’t seen each other in maybe 10 or 20 years,” Wynn says.
While the family members exchanged apologies, Wynn recalls the daughter saying, “I don’t even know why I was angry at you, I don’t even remember.”
“And they said, ‘We’re going to try to be a family again,’ ” Wynn says.
“You know, we talk about the last senses to go would be the sense of touch and hearing,” Wynn says. “And I hope that there was enough left of the dad that he had some sense that this bad situation had been healed through his death.”
Wynn says he felt honored, simply to witness that reconciliation, at the end of the man’s life.
[I]n the hospital one afternoon, after unsuccessful surgery to remove her tumor, my mother drifted in and out of sleep. I sat on a sofa in her room with light from the window streaming in as I read email. My mother began talking to someone. I looked up.
My mother was an attorney. She dealt in realities. For most of my life, I knew her as a woman with few illusions. She did not kid herself, and she did not let me kid myself. She told my sister and me, when we complained about a situation, “Life isn’t fair.” So when she was diagnosed with pancreatic cancer, my mother approached it matter-of-factly because it was a matter of fact no one disputed. She researched pancreatic cancer online, came to terms with her odds and spent the next seven months maintaining as much control as she could.
Yet illusions sometimes came to her in those months. In that hospital room, she wasn’t talking to me but to people standing on the other side of her hospital bed, people invisible to me. They weren’t there, but she saw them. I couldn’t make out my mother’s words, only that there existed a pleasant back-and-forth going on. I was the first witness to her illusions.
I knew that, as a child, my mother had spent many days in the hospital for surgeries to correct bilateral club foot so she could walk. Her memories of that time included an imaginary friend whom she named after the model of hospital bed in which she had lain. As I watched her that day, I wondered whether John Standard had returned to her after all those years.
A few minutes later, my mother turned to me, fully alert. I asked whether she remembered the conversation she’d just had. Friends she hadn’t seen in a long time, she said, without going into detail. Then she tilted her head and added, “But they weren’t really here, were they?” I admitted that, no, they hadn’t been here. She said, “Well, it was a good conversation.”
My mother’s illusions were not delusions. She was not misled. The word “illusion” comes from the Latin “ludere” meaning “to play.” The word has longstanding negative connotations, as in a deception. But my mother’s illusions were her mind at play.
How different that was from my father’s delusions years earlier, when he was in the hospital undergoing cancer treatment. His gift balloon had become a spaceship, and he described to my mother a terrible war around him. He was caught up in it, afraid. One of the medications he’d been prescribed caused the delusions, and they subsided once it was stopped. But he said the scene had been so real that he couldn’t not believe it at the time. It still felt real after he knew it wasn’t. My mother could deal with anything in the physical world but couldn’t imagine how she would manage if my father lost his mind. By that, she meant his mind losing touch with reality. And she meant that his physical deterioration was enough for her to bear.
Later in her illness, at home, my mother began seeing medieval people on a hillside in her own bedroom. She enjoyed watching them, robed in their dresses and breeches, and she especially enjoyed the music they played. Flutes and mandolins. They even brushed large ostrich feathers and long veils over her skin. She didn’t know when these musicians would show up, but she welcomed them whenever it happened. She knew no one else saw these people or heard this music, and she didn’t care that it wasn’t real. I had some concerns but didn’t know what to do with them. I didn’t talk about these illusions in my book “Tumor” because I didn’t yet know how. There are so many concerns when someone is dying of cancer.
My mother and I talked with her oncologist about this new development, wondering whether such a thing was common in patients with cancer, perhaps the result of wasting or dehydration, two serious physical concerns at that point, or perhaps a side effect of one of the medications or chemo drugs. The oncologist asked several questions.
“No,” my mother said. “I’m not afraid of them. No, they don’t try to harm me. No, they don’t make me do things.”
The midsummer-night’s-dream people never talked to her and she never talked to them. She explained this arrangement as if such conversation would be crazy. Then, she said, “The music makes me happy.”
The three of us — my mother, her oncologist and I — decided this illusion was the least of our worries, that, in fact, medieval singers on a hillside were no worry at all. She had nothing to lose by listening, as long as she could hear the rest of us too. I was surprisingly relieved the oncologist did not want to treat this cognitive symptom because often physicians want to correct what deviates from the norm. He considered the larger context, the limited time, and told my mother to let him know if she stopped enjoying these visions.
This illusion, of course, might be considered a hallucination. The word “hallucination” comes from the Latin meaning “to wander in the mind,” originally akin to dreaming or allowing one’s thoughts to ramble. Hallucinations are now considered deceptions, not merely stray thoughts or daydreaming. To be sure, they can result from serious illness such as schizophrenia, dementia, epilepsy, Parkinson’s disease or migraines and make it difficult to function day to day. So hallucinations also came to be defined medically as distortions of sensory perceptions that the person experiencing them takes as real experiences. My mother, then, wasn’t really hallucinating because, though she accepted her experiences as real in her mind, she knew the people she saw and heard were not real in the world. She liked the touch of ostrich feather on her skin but didn’t think it existed in the world beyond her imagination.
Here was a woman who’d always shopped for a new outfit by picking what was paired on the rack because she was unable to imagine original combinations on her own. When my mother’s body weakened, when her body betrayed her, her mind said, “Let loose and enjoy the music.”
Even in that first observation of my mother’s conversation with friends who were not there, I was not upset that my mother was losing touch with reality or becoming less herself because she seemed at ease. Though they were unexpected and out of the ordinary, I became grateful for the odd joy my mother’s illusions gave her. What a practical thing for her mind to have done. I wish I knew how she did it. Any of us may someday face a similar illness. How fortunate my mother was able to conjure up happiness all on her own without denying the harsh reality of her condition. May we each find or conjure some music in our minds when we need most to hear it.
[O]nly a tiny percentage of Canadians who’ve received medical assistance to end their lives has chosen to self-administer a lethal drug cocktail.
But that could change now that secobarbital — the drug most commonly used for assisted suicide in other countries — is available in Canada.
Secobarbital is considered the best way for suffering individuals who want to control the manner of their death as much as possible, including administering the medication themselves.
“It’s kind of the barbiturate of choice because (its) quicker onset and duration is such that the dying period is reduced,” said Dr. Stefanie Green, president and co-founder of the Canadian Association of MAID Assessors and Providers.
“Much of the other recipes cause an extended dying period to happen, which is not always successful.”
Health Canada reports that from June 2016 to June 2017 — the first year in which medical assistance in dying (MAID) was legal in Canada — a total of 1,982 individuals received an assisted death. Of those, just five were self-administered deaths.
Green said the unavailability of secobarbital may, at least in part, explain the small number of self-administered deaths.
In general, orally ingested drug cocktails present some difficulties that are not associated with those injected intravenously: they taste bad, they can induce nausea and vomiting, the patient can fall asleep before the entire dose is consumed, which can ultimately cause it to be ineffective.
“You want to mitigate those factors as best as possible,” Green said. “So if you’re going to choose to use a barbiturate and an oral cocktail, this (secobarbital) would be the best one.”
Among other things, she said secobarbital is more soluble than other barbiturates, meaning it can be dissolved in a smaller volume of liquid, thereby reducing the risk that patients won’t consume the entire dose.
Green expects that self-administered deaths will increase somewhat now that secobarbital is available.
“There are certainly a significant amount of people who want to be the ones to have the control, who want to be the ones with the medication in their hand, who want to say, ‘I’m going to take this to my backyard and drink it when I darn well please, thank you very much,”‘ she said.
The drug may be particularly helpful in rural or remote areas where it may be difficult to find a nearby physician or nurse practitioner willing to provide an assisted death, Green added. Individuals in those areas may find it easier to get a prescription for a lethal dose of secobarbital that they can administer themselves.
Because it is fast-acting, secobarbital may also make the self-administration option more viable in a province like British Columbia, where Green practices and which requires a physician to be present throughout the assisted dying process, even when the patient self-administers the medication. That was not feasible when the barbiturates used could take hours, or even days, to work, she said.
Secobarbital, once widely used as a sedative decades ago, has not been available in Canada for years. That it is now is largely due to Jocelyn Downie, a professor of law and medicine at Dalhousie University and a passionate advocate of medical assistance in dying.
When she realized few people were using the self-administration option, Downie said she explored ways to make secobarbital available. She discovered that the cost and time required to get the drug approved for marketing in Canada was a big obstacle so she found “an alternate path:” persuading a pharmaceutical products company to provide the active ingredients for the medication that can be compounded, or mixed, by a pharmacist to produce secobarbital.
Since the company doesn’t want its name publicized, Green said her organization is acting as “the middleman.” It will provide the necessary contact information to health care providers and pharmacists who are helping patients who choose the self-administered death option.
“For those of us in the field, it’s good news, it’s very good news to be able to offer this extra option to our patients, some of which we know will take it and we’ll be happy to provide a better quality product for them,” said Green.
Think back to the day you received your diagnosis of cancer. How soon did thoughts about death or dying come to your mind? For me, thoughts about death occurred within seconds after I received the news I had prostate cancer.
What’s surprising to me is how often I think about death seven years later, even though my last PSA test came back undetectable.
I’m five years out and I think about it almost daily.
I don’t think about it any more often than before I was diagnosed with prostate cancer.
Most days.
Every day.
I think of death too often.
The first thing I noticed was the variety of answers I received. I expected everyone to say they thought about it multiple times every day.
The answers I received suggest there’s a wide variation in how often cancer survivors think about death and dying.
The frequency of thoughts about death and dying is less important than the conversation we engage in with ourselves each time we think about dying.
My initial thoughts about death were terrifying. I imagined spending months in agonizing pain that no amount of medication would successfully manage.
I imagined my life savings would be wiped out by high deductibles and out-of-pocket expenses. I was convinced I wouldn’t live long enough to walk my daughter down the aisle, become a grandparent, retire in good health or travel with my wife.
I have a long list of friends, family and acquaintances who died within the year of receiving their diagnosis. Therefore, the possibility of surviving cancer never entered my mind.
I expected to go down hill rapidly and die within the first year after I received my diagnosis.
Every time I engaged in self-talk about dying, it ended the same way. I’d feel distressed, fearful, pessimistic about the future and overwhelmed with grief and sadness.
I wanted to protect my wife, so I kept these conversations to myself. I believe she wanted to protect me from her fears, so we coped with our individual fears together, but alone. In doing so, we deprived ourselves of the comfort and support we had to offer each other.
There are healthy, life-affirming ways to think about your own death, but where can you find them?
The Bible helped me overcome my fear and pessimism. These three verses were life changing:
Teach us to number our days, that we may gain a heart of wisdom. (Psalm 90:12).
A diagnosis of prostate cancer taught me to number my days. Since then, every part of my life changed.
Before my cancer diagnosis, if you said to me, “You’re going to write two award-winning books, write articles and cut your work schedule down to three days a week.” I wouldn’t have believed you. Yet, that’s exactly what happened.
O death, where is thy sting? O grave, where is thy victory? (1 Corinthians 15:55)
This verse is a powerful reminder to me that death isn’t the last chapter of my life.
We are confident, I say, and willing rather to be absent from the body, and to be present with the Lord (2 Corinthians 5:8)
This verse reminds me of where and with whom I’m going to spend eternity.
I’m no longer distressed when I think about death and dying. I’m reminded to use my remaining time wisely. My relationships, my priorities, my values and how I use my time, skills and talents were all transformed.
Your thoughts, feelings, past experiences, attitudes, religious beliefs and your personal history coping with loss will all impact the way you speak, comfort or cause distress as you think about your mortality.
Anna Benton, of Milwaukee, left, Georgette Paxton, of Madison, center, and Jennifer Snow, of Waunakee, look over Heather Ockler, of Monona, who is playing the role of a dying person wrapped in a shroud during a home funeral demonstration. It was part of a death midwife class taught last month by Sharon Stewart, who helped aspiring death midwives practice skills such as washing and shrouding a body. Death midwives, sometimes called death doulas, are increasingly helping families prepare for and navigate the death of loved ones, in addition to or instead of hospice care and funeral homes.
[B]efore Valli Warren’s husband died last year after a long illness, the Stoughton couple knew they wanted a home funeral and green burial.
But they weren’t sure how to make those things happen. They turned to Sharon Stewart, who delivered ice packs to preserve the body, shared videos about how to wrap it in a shroud and taught pallbearers how to carry it out of the house on a board.
Stewart also helped Warren file paperwork, including a permit letting her transport her husband to Circle Cemetery, near Barneveld, where he was laid to rest without being embalmed or using a casket or vault.
“She walked me through every phase,” Warren said.
Stewart is a death midwife, a new kind of occupation that provides emotional, spiritual and practical support to families before and after death — in addition to, or instead of, hospice care and funeral homes.
The service, which has emerged around the country over the past decade, is analogous to what birth midwives do compared to obstetricians. Some who offer the assistance call themselves death doulas or end-of-life midwives.
‘Back to their roots’
Whatever the title, the providers say they help people “take back” the death process from hospitals and funeral homes. Services include leading family discussions about death planning, sitting vigil with people as they die, helping family and friends wash the body afterward and aiding in tasks such as selecting memorial cards, sending obituaries to newspapers and closing social media accounts. It often involves home funerals or green burials.
“We’re taking families back to their roots, the tradition of when we were born and when we died in our own homes,” said Stewart, a former detective who lives near Brooklyn, south of Madison. “We laid in honor in our parlors, and the community came together to provide care for the family.”
Liz Humphries, a former birth midwife and hospice nurse who recently added an end-of-life doula service to Seasons of Life, her senior care company in Middleton, said, “It’s about reclaiming a really sacred and beautiful human experience.”
Mary Paulauskis, a former hospice nurse from Madison, has added what she calls end-of-life transitions counseling to her business, Mindful Awakenings, through which she teaches meditation.
Paulauskis focuses on helping people think about who and what they want around them as they die. She also coaches loved ones on what to say to a dying person and how to interact — letting them know it’s OK to lie next to the person if they want to, for example.
“It’s creating a space of whatever the patient said they want,” Paulauskis said.
Many people don’t realize that there are several ways to dispose of bodies without embalming, including new, greener types of cremation, said Angie Buchanan, a death midwife in Waukesha who trains death midwives around the country. She informs clients of the options and guides them through their choice.
“We’re the water that runs between the rocks of the medical profession and the funeral industry,” Buchanan said.
Dr. Toby Campbell, chief of UW Health’s palliative care program and a board member of Agrace Hospice and Palliative Care in Fitchburg, said he understands why death midwives are catching on. He said hospice care typically includes two or three visits a week from a nurse or social worker, and an occasional call from a doctor.
“That leaves about 99 percent of the time you and your family are on your own,” Campbell said. “That’s a big space. There are giant gaps between the health care system and death, even including hospice.”
Jim Olson, president-elect of the Wisconsin Funeral Directors Association, said caring for a body after death and managing a funeral are big jobs. Most people will continue to seek help from funeral directors, he said.
Death midwifery is “another alternative for families, which we think is great,” said Olson, who owns Olson Funeral Home and Cremation Service in Sheboygan. “Am I afraid it’s going to affect my business? No, absolutely not.”
There is no licensure or government certification for death midwives. Experienced practitioners, such as Stewart and Buchanan, offer training, as does the New Jersey-based International End of Life Doula Association, which held a session in Madison last year.
Many training programs offer their own certification. The burgeoning field is in a similar situation to massage therapy in the 1990s, before doctors pushed for its regulation, Buchanan said. In Wisconsin, certification for massage therapists started in 2003, with licensure beginning in 2010.
Fees for death midwives vary. Buchanan said she charges $100 for a consultation and up to $2,000 for services covering the whole death process. Stewart has accepted donations of $100 or $200 from some clients, but she doesn’t plan to establish rates until she retires from her day job, at the state public defender’s office, and devotes more time to death midwife duties.
Paulauskis said she plans to charge $25 to $50 for a counseling session and negotiate rates for other services but let people pay what they can. An academic adviser at the UW-Madison School of Social Work, she plans to continue making her living in other ways.
Humphries, who started her end-of-life doula service last month, said she might charge $40 to $100 an hour but offer a sliding-fee scale for people with low incomes.
Humphries is also an organizer of Walking Each Other Home Madison, a group that started in 2014 to help people carry out home funerals and green burials. People can rent the group’s home funeral kit, which includes a body board, ice packs, soap, lotion, diapers, latex gloves and small bags of rice to place over the dead person’s eyes to keep them closed.
‘The personal touch’
Stewart, who has long volunteered at Monroe Clinic’s hospice program, said she saw the need for a more personal death service after her brother died in a car crash at age 19. She was 21.
Police came to the house in the middle of the night, told her mother her son was dead and left. Stewart wanted to see her brother’s body before he was embalmed, but the funeral director wouldn’t let her, she said.
“There had to be a better way,” she said.
Later, as a detective for the Lafayette County Sheriff’s Department in Darlington, Stewart tried to deliver death notifications with more sensitivity. But she wasn’t able to do all she wanted to help grieving families. After a shoulder injury forced her to retire, she discovered death midwifery.
“I thought, ‘This is it. This is the personal touch. This is the attention that families need,’ ” she said.
At a death midwife class she taught last month, Stewart told students to help dying people reconcile with others if they ask, separate arguing family members at the bedside if necessary and encourage loved ones to say goodbye and leave the room if the dying person wants to die alone.
“Your job as a death midwife is to be an advocate for that dying person,” she said.
When Laurie Larson’s husband, Dennis Presser, died suddenly from a heart attack at age 54 four years ago, Stewart helped Larson and her two teenage children navigate the chaos.
Stewart joined Larson when she met with a funeral director to plan the funeral, which took place at the funeral home.
She organized an intimate gathering for family and close friends at the crematorium, with candles, incense and music. As Presser’s body lay inside an open cardboard cremation box, people read poems, told stories and colored the box. Then they placed him in the chamber, and Larson hit the ignition switch.
“I would never have had the energy to create that beautiful ritual,” said Larson, of Madison. “Sharon helped me in so many ways that I never would have thought I needed to be helped.”
Warren’s husband, Spencer, died at 64 from amyotrophic lateral sclerosis, or ALS, also known as Lou Gehrig’s disease.
Stewart helped the couple carry out their wishes. His body remained at home for three days, instead of being whisked off to a funeral home. “I had time to be with him; it was very healing,” Warren said.
As family and friends came for the home funeral, volunteers changed ice packs beside his body as he lay on their bed for viewing. Warren drove him to Circle Cemetery, where gatherers sang and played guitar before shoveling dirt over his shrouded body.
“It was the most natural thing I’ve ever experienced,” Warren said.
Buddhist teacher Frank Ostaseski has been one of the leading voices in contemplative end-of-life care since the 1980s.
By Lion’s Roar Staff
[I]n this video, Ostaseski talks with Lion’s Roar’s Lindsay Kyte about the lessons he’s learned at the bedsides of thousands of dying people, his new book The Five Invitations, and the future of end-of-life care.