Although a dying person tends to spend more and more time asleep or unconscious, there may be a surge of brain activity just before death
By Denyse O’Leary
Wednesday was Ash Wednesday in the Western Catholic tradition. It marks the beginning of Lent, a season of reflection and repentance. A common custom is that, during the service, the priest traces the sign of the cross in ashes on the penitent’s forehead, saying “You are dust and you will return to dust” (Gen 3:19). It’s one of many customs worldwide that offer a sobering reflection on the inevitability of death for all of us — unless, of course, we are transhumanists who genuinely believe that technology can grant us immortality.
What does dying actually feel like?
Most human beings have always believed that the essence of a human being survives the death of the body though the outcome is envisioned in a variety of ways. But, assuming that pain and distress are controlled, what does dying actually feel like? Can science tell us anything about that?
At BBC Science Focus, palliative care doctor Kathryn Mannix offers a few thoughts from long experience, including:
A dying person spends progressively less time awake. What looks like sleep, though, gradually becomes something else: dipping into unconsciousness for increasing periods. On waking, people report having slept peacefully, with no sense of having been unconscious…
As dying progresses the heart beats less strongly, blood pressure falls, skin cools down and nails become dusky. Internal organs function less as blood pressure drops. There may be periods of restlessness or moments of confusion, or just gradually deepening unconsciousness…
Breathing moves from deep to shallow and from fast to slow in repeating cycles; eventually breathing slows and becomes very shallow; there are pauses; and, finally, breathing ceases. A few minutes later, the heart will stop beating as it runs out of oxygen.
Kathryn Mannix, “What does dying feel like? A doctor explains what we know” BBC Science Focus, February 10, 2024
Surge of brain activity just before death
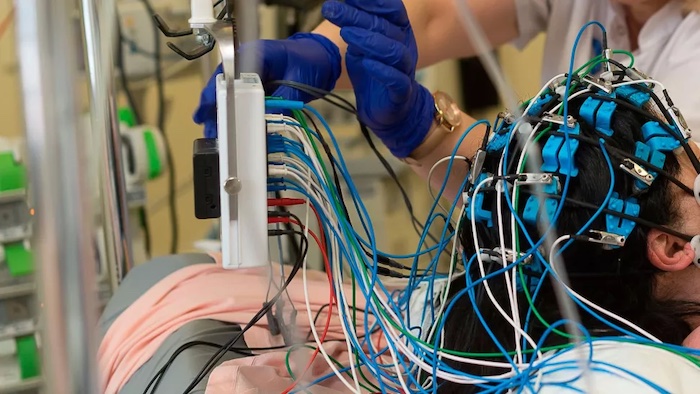
We are also learning that, contrary to what we might have expected, the brain does not necessarily just die down quietly. Researchers have recorded a surge of activity just before death:
To that end, the brain activity of four people who passed away in hospitals while being monitored by an EEG (electrogram) device was studied.
“The data generated, even though it’s only four patients, is massive, so we were able to only report a fraction of the features that it’s actually showing on the data,” Prof. Borjigin said.
At the time of death, brain activity was detected in the TPJ region of the brain — named because it’s the junction between the temporal, parietal and occipital lobes in the back of the brain.
Dan Gray, “Study finds evidence of increased brain activity in people right before they die,” Medical News Today, May 5, 2023. The paper is open access.
In any event, cells deprived of oxygen are doomed. But that does not mean that all of the body’s cells cease to function immediately when a person dies:
The brain and nerve cells require a constant supply of oxygen and will die within a few minutes, once you stop breathing. The next to go will be the heart, followed by the liver, then the kidneys and pancreas, which can last for about an hour. Skin, tendons, heart valves and corneas will still be alive after a day. White blood cells, which are more independent, can keep going for almost three days.
Luis Villazon, “When we die, does our whole body die at the same time? ”BBC Science Focus, nd.
So when a medic declares a person dead, that means that the death process is past the point of no return, not that every cell in the body is dead.
Terminal lucidity — getting in the last word
There are many stories through the ages of people near death suddenly waking up and saying something lucid. Researchers who study the phenomenon call it terminal lucidity. At Psychology Today in 2018, nurse educator Marilyn Mendoza noted regarding research to date::
So far, the response rate to the questionnaire he distributed has been limited. While the results are in no way definitive, out of the 227 dementia patients tracked, approximately 10 percent exhibited terminal lucidity. From his literature review, Nahm has reported that approximately 84 percent of people who experience terminal lucidity will die within a week, with 42 percent dying the same day.
Marilyn Mendoza, “Why Some People Rally for One Last Goodbye Before Death,” Psychology Today, October 10, 2018
As to why it happens, she offers,
There is as yet no logical scientific answer to this medical mystery. There is just not enough information to postulate a definitive mechanism for terminal lucidity. The fact that it occurs in people with different diseases suggests that there may be different processes occurring. Some speculate that this could be a spiritual experience or divine gift. It certainly is a gift for family members attending the death to have one last opportunity to be with their loved one and to say their last goodbyes. Both family members and caregivers who have been witness to this state that they feel changed by the experience.
Mendoza, “One Last Goodbye”
One interesting trend is this: Fifty years ago, slick media commentators expected to report that research into death and dying would explod all those myths about a soul or the hereafter or the human mind. But the opposite has happened. Topics like terminal lucidity and near-death experiences are conventionally researched now. And it’s just as clear now as it was fifty years ago that life is a journey and death is not, itself, the destination; rather, it’s a gateway to one.
Sherry Campbell, director of Welcome Home, stands with former resident Clint Jackson outside the hospice and medical respite home in Chattanooga, Tennessee, on April 2, 2023.
A few years ago, Mark Adams was diagnosed with colon cancer. His doctors didn’t want to operate, he said, because his recovery could be too risky without a clean place to recuperate. He was living on the street.
Soon, it was too late, his cancer too far along. That’s what they discovered after he moved into Welcome Home, a facility offering long-term medical respite and end-of-life care for unhoused adults.
Instead of getting better, he’ll likely live out the rest of his days there – one of a small number of places in the United States that offers unhoused people a comfortable and dignified option when they are terminally ill.
Sufficient end-of-life care in the United States is a growing problem for the general population, as America’s aging baby boomer generation needs more intensive and expensive help and supply isn’t keeping up. For many unhoused adults — who frequently lack a strong social safety net — long-term medical or hospice care are effectively inaccessible. In the absence of publicly funded solutions, private organizations and nonprofits are trying to plug the gaps, but the patchwork network of end-of-life care homes is far too limited to address the need.
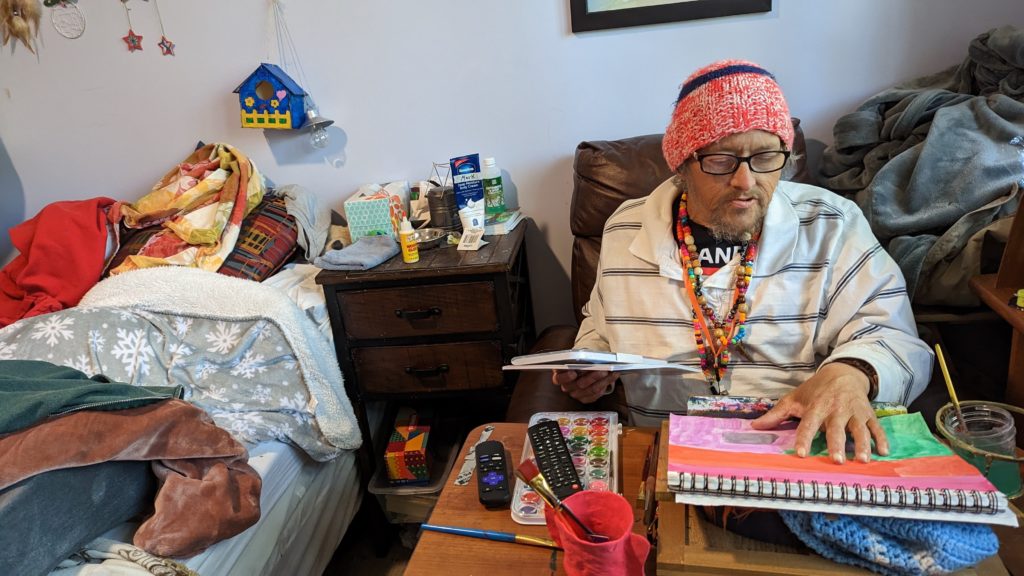
On a mild spring Sunday, Adams worked on a painting in his cozy, eclectic room – filled with vinyl records, potted plants and his own art – while his friend Clint Jackson relaxed nearby. Up the hill, Standrew Parker rested on a wrought iron chair in his yard, soaking up the early afternoon sun and chatting with his new roommate, Heidi Motley. Parker, 40, and Motley, 58, are staying there while undergoing treatment for cancer.
Mark Adams displays his artwork in his room at Welcome Home in Chattanooga, Tennessee, on April 2, 2023.
Across the country, there are a handful of facilities like Welcome Home, which sits on nearly five forested acres in Chattanooga, Tennessee. Some 1,300 miles west, there’s Denver’s Rocky Mountain Refuge for End of Life Care. Salt Lake City is home to The Inn Between, while Washington, D.C. has Joseph’s House. In Sacramento, Joshua’s House plans to open its doors this fall. Dozens more offer medical respite beds, generally for those undergoing long-term medical treatment. But outside of these organizations, experts told the PBS NewsHour that there are few other places where people experiencing homelessness can go for end-of-life or hospice care.
These facilities aren’t massive – Welcome Home has three medical respite rooms in addition to its four hospice beds, and is opening another house with an additional three rooms this month. Rocky Mountain Refuge, the smallest and newest of the group, has three beds solely for end-of-life care.
The need for those beds is great: People who are homeless are at far higher risk for many illnesses and conditions, such as heart disease. Medical research also shows that unhoused people’s bodies have often aged as if they were at least a decade older.
Being without a home is itself “a life-limiting diagnosis,” as Hannah Murphy Buc, a researcher who studies palliative and end-of-life care for people experiencing homelessness, wrote in the journal Caring for the Ages.
When someone is already in poor health, there are basic obstacles of living without a home – not having access to a fridge to store medications or the ability to secure narcotics for pain management, for instance. Some people without permanent addresses, like Adams, have reported they were denied treatment for their cancer due to the physical demands of recovery.
“Hospice and palliative care, but particularly hospice, is completely reliant on having a place to receive it,” Murphy Buc told the NewsHour.
For Adams, 51, living at Welcome Home has been life-changing, even though he often feels sick and he says he knows the cancer will likely kill him.
“I feel good here. I feel like I’m welcome here,” he said.
What we know about deaths among the unhoused
There is no official national data on where, when and how people experiencing homelessness die. According to an analysis by the National Health Care for the Homeless Council (NHCHC), at least 5,800 people died while experiencing homelessness in 2018. That’s almost certainly an undercount, and the report noted the actual number could have been anywhere between 17,500 and 46,500 deaths for that year.
With more people expected to become homeless and as that population ages, that mortality figure expected to rise, said Dr. Margot Kushel, director of UCSF’s Center for Vulnerable Populations and Benioff Homelessness and Housing Initiative.
“The truth of the matter is most of the country is entirely unprepared for this,” Kushel said.
An inspirational sign is displayed near a cookie jar in the kitchen of Welcome Home, in Chattanooga, Tennessee, on April 2, 2023. Residents gather nightly for dinners provided by volunteers as a way of fostering community.
Local reports can help explain what’s happening currently to those who can’t access end-of-life care. Across several months in 2021, deaths among unhoused people in San Francisco occurred primarily outdoors, in places like encampments, vehicles or on the street, a report from the NHCHC found. Others died in medical facilities; motel rooms, either rented by the person or as a shelter-provided space; other people’s homes; and homeless shelters.
Similarly, in King County, Washington, about half of the people experiencing homelessness who died in 2018 perished outdoors, according to a report from the council. Only 26 of the 194 deaths occurred in residences.
A 2022 report from the Colorado Coalition for the Homeless found that among the unhoused individuals who die of so-called “natural causes,” 30 percent died in hospitals or other medical facilities, and 25 percent died outside.
“That means under a bridge, on a sidewalk, behind a bush, in a tent,” said Brother James Patrick Hall, the executive director of Rocky Mountain Refuge.
While in prior decades people experiencing homelessness may have died from acute causes, such as violence or illness, the aging population of unhoused people is now living with the chronic conditions that plague many seniors, such as COPD, heart failure, strokes and cancer.
“These folks often need a lot of personal care. They have pain issues … It’s like a disaster, to be honest,” Kushel said. “What we found in Oakland is [that] a lot of folks just died on the street, short of breath, in pain, incontinent.” Others were admitted to hospitals, and some ended up at nursing homes or acute care facilities, “but it wasn’t where they wanted to be.”
When given a choice, people overwhelmingly want to die at home, according to Murphy Buc. Death at home can lead to healing in relationships and help soothe those left behind. But even when that’s an option, it can be draining for those doing the caretaking, she noted, even with hospice nurses visiting a few times a week.
In the U.S., “we don’t do death well,” Murphy Buc said.
The problem of older people dying on the streets, in motel rooms and in cars is the ultimate result of disinvestment in affordable housing, skilled nursing care and health care, experts at the NHCHC told the PBS NewsHour.
It’s not that people who become homeless are falling through the cracks, said Barbara DiPietro, senior director of policy at the NHCHC. Instead, people are often forced into “gaping caverns” where underfunded social safety nets, such as Medicaid and public housing, fail to catch them.
An older adult who has worked as a manual laborer her entire life might have a stroke and lose employment, be unable to pay rent and end up without a home, said Caitlin Synovec, senior program manager with the council’s medical respite team. Shelters frequently can’t help people with enhanced medical needs, so they have nowhere else to turn.
The unhoused population is also disproportionately vulnerable, low-income and people of color — all groups who have historically experienced disparities and may distrust the nation’s health care and social services systems.
In addition to that added barrier, people may just not know they have medical respite and end-of-life care options, Murphy Buc said. Many of the current residents of these facilities were referred there by health care professionals or social workers, but had not previously heard of them.
‘Health care isn’t housing’
Having a home, in and of itself, can be considered a form of health care, advocates say. Those who work or volunteer at care homes sometimes witness very sick people make dramatic recoveries simply because they have a safe, comfortable and stress-free place to live.
Though each facility operates slightly differently, these homes offer more than just a physical address, providing services like palliative care, case management and transportation. Volunteers and staff can remind residents to take medicine, ask how they’re feeling, and, crucially, drive them to appointments.
Before Standrew Parker lived at Welcome Home, he would have to travel to the hospital from his mother’s house to receive five days of cancer treatment every few weeks. In addition to being an unwelcoming environment, her house was about 45 minutes away by rideshare, which cost around $60 to $70, he said. To avoid the trip back and forth, he would instead often spend his days living outside the hospital.
“We didn’t have that money. So I was in and out, just like hanging out. If I had multiple appointments for days on end there, I just [stayed outside the hospital]. I would have to or I wouldn’t get the correct shots or the treatment,” Parker said.
Crystal Jones, nurse case manager at Joseph’s House in Washington, D.C., works at her desk on April 4, 2023.
Now, volunteers drive him to and from his treatments, and during his weeks off from chemotherapy, he recuperates in his room at Welcome Home. Beyond the care he receives, the empathy and compassion from staff and volunteers helped shift his entire perspective on healing.
“It’s like a world of difference between surviving and actually being able to get well,” he said.
A crucial goal of each facility is to establish a sense of normalcy for people whose lives have been thrown out of balance. Welcome Home serves dinner every night, where residents can gather and rib one another. People living at The Inn Between can join the resident council, which offers both community and a way to effect change, such as what times coffee is available. For the patients who recover enough, these homes can help them adjust to life outside of the facility so they can leave.
When NHCHC began their medical respite programs in the late 1980s, they were originally intended as short-term stabilization. However, some of the programs that specialize in medical respite have begun to consider incorporating end-of-life and hospice care into their models to fill the gap, said Julia Dobbins, director of medical respite at NHCHC’s National Institute for Medical Respite Care.
In contrast, patients without somewhere to go sometimes cycle between a hospital and the street, being readmitted when their problems are acute enough to warrant immediate care, and released when they’re stabilized, Murphy Buc said.
Sending still-sick people back to the streets is called “patient dumping,” and “it’s horrible,” Kushel said. But, she added, the solution can’t be that people live at a hospital for months on end until they die. That’s an inefficient use of resources, not to mention that it’s unlikely to be where a patient wants to spend the rest of her life.
Hospitals don’t want to deny people care, Kushel said. When she heard about Adams’ doctors refusing to treat his cancer while he was experiencing homelessness, she noted that his situation was not uncommon. Doctors worry about harming people who don’t have access to long-term, safe and clean care, but it doesn’t make it an easy decision.
“It happens all the time,” Kushel said. “And when you speak to the surgeons, they actually feel terrible about it.”
In the long run, even medical respite doesn’t solve the problem of where people can live, said NHCHC’s DiPietro.
“We often say housing is health care. Absolutely,” she said. “Unfortunately, health care isn’t housing.”
For many, providing medical respite or end-of-life care to people experiencing homelessness with their own limited resources can feel like a Sisyphean task.
For every person given a bed, there are countless others who need and can’t access one. Each organization can only serve their local community, leaving hundredsof people or more to dieon the street nationally each year.
Beyond what the organizations receive from state and local funding, there’s little — if any — government funding for long-term medical care or end-of-life care for people with no fixed address. These organizations’ funding models are largely reliant on grants and donations, without long-term stability.
“It’s local advocates who are seeing the suffering of their community members, and so they’re creating these programs that are funded by the good of people’s hearts, and that’s it,” Dobbins said.
Rocky Mountain Refuge, which opened its doors a little over a year ago, struggles to find enough funding to stay open, Hall said. That’s an experience echoed across the country.
“One of the stresses for us here is, every year, are we going to be able to keep our doors open because of the funding?” said Kowshara Thomas, director of Joseph’s House in Washington, D.C.
Founded in 1990 during the HIV/AIDS crisis, the three-story house in a quiet residential neighborhood has served community members dying of the disease for decades. This year, however, they lost a major grant that comprised 30 percent of their revenue, which worries Thomas. Other medical respites in the D.C. area receive Medicaid funding, and larger organizations are often better positioned to write grants and secure funding. But Thomas says Joseph’s House, with only eight beds, is too small to follow suit.
A memorial wall of former residents is displayed at Joseph’s House in Washington, D.C., on April 4, 2023.
The organization has largely, though not entirely, pivoted from end-of-life care to medical respite, something Thomas sees as both a result of better health among their community and a way for them to provide continuing care for people after they’re discharged. Joseph’s House has around 25 community members for whom they provide supportive services.
Thomas is also proud of the community that Joseph’s House anchors, with former residents coming back for meetings, social time and sometimes additional long-term or end-of-life care.
“Having a place where you can feel safe and get the support — the medical and the psychosocial support — is really what helps our community,” Thomas said. “Joseph’s House is, for some of our residents, the first time they’ve ever had family or felt like they belonged somewhere and they could just be who they are.”
— An increase in a certain kind of high-frequency wave in dying brains might be associated with last-minute conscious experiences, but scientists don’t know for sure.
In a new study, researchers recorded comatose patients’ brain activity as they died.
In their last minutes of life, some people’s brains generate a surge of surprisingly organized-looking electrical activity that may reflect consciousness — although scientists aren’t entirely sure.
According to new research, published Monday (May 1) in the journal PNAS (opens in new tab), this surge can sometimes occur after a person’s breathing stops but before the brain stops functioning. The activity pattern is somewhat similar to what is seen when people are awake or in dreamlike states, leading to speculation that perhaps these electrical surges reflect the otherworldly experiences reported by people who’ve had close brushes with death: A sense of looking at the body from the outside; a tunnel and white light; or a sense of reliving important memories.
However, since all the patients in the new study ultimately died, it’s impossible to know if they had such experiences.
“If you talk about the dying process, there is very little we know,” said Jimo Borjigin (opens in new tab), a neuroscientist at the University of Michigan Medical School who led the study. It’s rare for patients to have their brains continuously monitored as they die, Borjigin told Live Science. “This is maybe the first study to really show second-by-second how the brain dies.”
Near-death experiences
Some people who are brought back from the brink of death report seeing or hearing unexplained things during resuscitation or when they seem to be unconscious. The reason for these near-death experiences is unknown, and it’s not clear if they’re even specific to death.
International surveys suggest that only about half of what people call “near-death experiences” actually occur in life-threatening situations, said Daniel Kondziella (opens in new tab), a neurologist at the University of Copenhagen who was not involved in the new research. The other half occur during meditation or in scary situations that don’t endanger one’s health or impact the brain’s metabolism, Kondiziella told Live Science.
“The thing is, from the experience itself you cannot say if someone has had a cardiac arrest or syncope [a brief loss of consciousness] or near-miss traffic accident,” Kondiziella said.
Because the people who survive to report a near-death experience are inherently different from the people who die — their brains don’t permanently lose function, for one thing — it’s hard to determine whether those who actually die also have these subjective experiences.
In 2013, Borjigin and her colleagues measured electrical activity in the brains of rats (opens in new tab) that they euthanized via cardiac arrest. They found that for about 30 seconds after the heart stopped, the brain showed a surge in what are called gamma waves, which are the highest-frequency electrical oscillations in the brain. Gamma waves are correlated with conscious experience, but don’t necessarily prove that someone is conscious; they’re just one of many indicators that someone might be aware and alert.
In 2022, a separate group of doctors happened to be monitoring the brain of an 87-year-old man with an electroencephalogram (EEG), which detects electrical activity on the surface of the brain, when the man unexpectedly died. Similar to Borjigin’s rats, the man’s brain showed a surge in gamma activity in the 30 seconds before and after his heart stopped.
‘Reading’ the dying brain
In their new paper, Borjigin and her team made a deliberate effort to use EEG to capture what the brain looks like during death.
The researchers got permission to monitor dying patients in intensive care whose breathing support had been removed after treatment proved futile. The study included four patients total, all of whom were comatose after cardiac arrest.
In the 30 seconds to two minutes after their ventilators were removed, two of the four patients’ brains showed surges in gamma waves. Interestingly, this gamma activity seemed organized, in that the gamma waves in one portion of the brain were associated with predictable activity patterns in other regions.
The temporoparietal junction, a brain region where the temporal and parietal lobes meet, toward the back of the brain behind the ear, was particularly active with gamma waves. This region is known to be activated when people have out-of-body experiences or dreams, Borjigin said.
The new findings echo what was seen in the 87-year-old patient who unexpectedly died, said Raul Vicente (opens in new tab), a neuroscientist and data scientist at the University of Tartu who co-authored the 2022 study but was not involved in Borjigin’s work. “It’s very nice to see a confirmation,” he told Live Science.
“The more consistent findings we have, the more evidence it is that this likely is a mechanism happening at the time of death and if we can pinpoint this down to one location, even better,” said Ajmal Zemmar (opens in new tab), a neurosurgeon at the University of Louisville Health who also co-authored the 2022 study.
Zemmar and Vicente are optimistic that these signals could be signs of conscious experience at the moment of death. But reflecting the debate in the field, Kondziella is more skeptical.
“We know when you die a cardiac death as opposed to a brain death, that takes time,” he said. Minutes pass between the heart stopping and brain cells dying, he said. “It shouldn’t be a big surprise during those minutes, you will see aberrant electrophysiological activity in the brain.”
Some people may experience something like near-death experiences in these moments, Kondziella said, but we may never know for sure. And again, these experiences may not be unique to death — a more likely explanation for near-death experiences that encompasses both life-threatening experiences and non-life-threatening experiences, he said, may be “REM sleep intrusion into wakefulness,” a situation in which the brain blends waking and dreaming states. (REM sleep is marked by dreaming and brain activity patterns that are very similar to waking, including gamma waves and other, lower-frequency waves.)
Borjigin’s team is still collecting end-of-life data, hoping to add to the evidence that the dying brain may generate predictable gamma-wave patterns. Already, other research groups have attempted to use artificial intelligence to identify objects that people saw in their dreams (opens in new tab) based on their brain activity — similar mind-reading may be possible with unconscious and dying patients, Vicente said.
“This opens an opportunity at some point, if we gather enough data, to be able to decode what people in different coma states are thinking,” Vicente said.
— It can be difficult to know exactly when someone is going to die, or has died. This page details some of the most common signs.
The following symptoms are often a sign that the person is about to die:
They might close their eyes frequently or they might be half-open
Facial muscles may relax and the jaw can drop
Skin can become very pale
Breathing can alternate between loud rasping breaths and quiet breathing.
Towards the end, dying people will often only breathe periodically, with an intake of breath followed by no breath for several seconds. This can be upsetting to witness as the person seems to stop breathing only to start again. There might be one or two last gasps a minute or so after what seemed like the last breath, before breathing eventually stops.
When someone dies
The moment of someone’s death is often very profound, even when you have expected it for a long time. You might want to talk to someone or call family and friends to let them know. You might prefer to be alone.
Some people feel overwhelmed with sadness, for others it can take days, weeks or months to process how they feel.
If you have been caring for the person you might feel exhausted, and the relief and finality of the moment of death can take you by surprise.
Every person’s experience of dying and bereavement is unique. However you are feeling, there are organisations and resources to help you. If you think you could benefit from bereavement support visit our page on how to find bereavement services.
It’s hard to ask your doctor what dying will be like. Death is a gut-wrenching reality for everyone. If you have an incurable illness, knowing what to expect as your body shuts down helps you prepare for as “good” of death as possible.
If you have an incurable illness, knowing what to expect as your body shuts down helps you prepare for as “good” of death as possible.
There are similarities to every death, but each dying person’s journey is unique.
Normal signs and symptoms of dying are increased fatigue and weakness, social withdrawal, increased pain, loss of appetite and thirst, and altered mental status.
Changes in the bladder, bowel movements, breathing, and vital signs are also normal.
Facing these changes alone can increase suffering. Seek help earlier in your journey from your loved ones and a palliative care specialist.
A “good” death to most people is free of avoidable suffering and aligns with their cultural, spiritual, and relational wishes as much as possible. To achieve a more peaceful death, studies and experts say preparing helps.
As a hospital nurse, I cared for many dying people during their final hours and walked their families through the process. Every last breath was sacred and unique. The patients who learned about death and talked about what they wanted to develop a realistic plan for their comfort. They were more likely to avoid unnecessary suffering for themselves and their families.
At a point in the dying process, you’ll become unconscious and no longer able to express your wishes. Talking sooner than later about your end-of-life needs empowers your family and caregivers to care well for you when that time comes.
What it’s like to die: signs and symptoms of natural dying
A “natural” death refers to someone dying of a terminal illness or old age. More sudden death due to a traumatic injury will have some of these similar signs but at a more rapid pace depending on the injury. These signs and symptoms occur during the last few months to hours of a dying patient.
1. Weakness and fatigue
As the end nears, it’s normal to feel weak and sleepy, but the timeline differs for everyone. Some become weak quickly while others – often younger or healthier at diagnosis – take longer but then decline rapidly.
It’s okay to sleep as much as you need. Try to time your daily tasks and activities for when you’re more likely to have energy.
As you get weaker, a simple activity like sitting outside, going out to eat, or being with your children can cheer you up, even if it’s exhausting. But there may be a point where you simply can’t do it anymore.
Be honest with your loved ones and caregivers about how you’re feeling. Rather than push yourself too hard, be willing to ask for help when your muscles become too weak to move on their own.
2. Social withdrawal
As you progress toward death, you may feel less social. It can be hard to tell this to your loved ones, especially if you’re from a culture or community that many people want to visit. But it’s okay to let them know if you want fewer visitors. Try your best to explain how you feel, assuring them it’s not their fault.
At the end of life, some people want to be surrounded by friends and family instead of becoming less social. Let your loved ones know if you enjoy their visits.
As you feel more withdrawn and weaker, consider the remaining important things you wish to say and try to have the courage to say them before it’s too late.
3. Pain
Your pain may increase as your disease advances or your joints stiffen, but no one should suffer needlessly. Medications, hospice care, and alternative health treatments all help ease your discomfort.
It is difficult for your loved ones to see you hurt. Be sure you talk thoroughly with them about how you want to manage your pain. You may want enough medication to ease the pain while also staying awake with loved ones. Or, you may want the medicine to help you sleep painlessly for much of the day.
Take oral pain medications 45 minutes before the pain becomes intense or before you have an activity planned. Use consistent language to describe your pain so loved ones and caregivers understand when it changes. Make a list of questions about pain management to ask your hospice nurse during their next visit, such as when to call them about increasing pain and how best to take your pain medication. Consider alternative treatments like acupuncture, massage, music therapy, or Reiki.
As you near death and can no longer talk, your loved ones and medical providers will watch for nonverbal signs of pain like grimacing, moaning, stiffening, resistance when they try to move you, calling out, restlessness, or labored and uncomfortable breathing. They can give you medications for any signs of discomfort.
You can trust that with medical help like hospice, you’ll be more comfortable and peaceful.
4. Loss of appetite and thirst
Nearly all patients lose their appetite as they near the end. Your brain will not trigger hunger and thirst sensations during the final stage of death, so you may have no desire to eat or drink.
Eating and drinking less – or not at all – is a normal part of dying as the body stops using nutrients like it did when it was healthier. As a result, your hospice nurse won’t advise trips to the hospital for intravenous (I.V.) fluids or artificial nutrition.
Your loved ones might fear you’ll “starve to death” and plead with you to eat or drink, believing it will increase your comfort and strength. Remind them with kindness that you’re not uncomfortable. When your body is dying from an incurable illness, it will continue to shut down no matter how much you eat.
Eating or drinking less may make your mouth dry and uncomfortable, however. You or your loved ones can apply lip balm and mouth moisturizer. You can also lightly moisten oral sponges with water to moisten your mouth.
5. Dreams, visions, and hallucinations
In the final days and hours, you may become less alert, drifting in and out of consciousness. Many dying patients have dreams and visions of lost loved ones, God, or other spiritual realities. You may experience hallucinations or a surge of energy just before you die. Some feel an increased awareness of death as it gets closer.
For most people, this delirium or altered state of consciousness is peaceful and not distressing.
However, if you become agitated, medications like haloperidol can restore your comfort. Caregivers can also check for other problems like pain, constipation, bladder infections, or side effects of medication.
If you experience such symptoms when you are still awake and alert, it can be helpful to talk with loved ones or care providers like end-of-life doulas and hospice nurses, counselors, and chaplains.
6. Bladder and bowel changes
At different stages during the dying journey, you may notice bowel and bladder changes.
Your urine may change color due to organ failure, and you may urinate less. Depending on your disease process, you might lose control of your bladder – also called bladder incontinence.
Incontinence can cause skin breakdown for bedridden patients. If this happens, some medical providers recommend a urinary catheter if they increase patient comfort while protecting their skin. A catheter may also be recommended if your bladder is retaining urine.
Constipation is not uncommon at the end of life. Your medical providers should counsel you on taking stool softeners and laxatives for constipation. These should be stopped or decreased, however, if you stop eating.
It may feel awkward, but it’s always best, to be honest about these symptoms with your caregivers.
7. Skin changes
In the later stages of the dying process, your skin may change in temperature and color as it stops functioning. During your final days, your body will move blood away from your arms and legs while it shunts it to the vital organs. These changes can make you feel cold and make your skin look pale, gray, or blotchy.
Some people, however, feel warm and flushed or develop a slight fever. A cool cloth on one’s forehead may ease the heat.
Keep your loved ones informed when you get too cold or hot. This helps them understand your body’s trend to care for you when you’re unconscious. Heated blankets and heating pads can be helpful but can also burn your skin if ignored.
8. Breathing changes
When people are within days to hours of dying, their breathing changes. Sometimes it’s very slow and regular with only a few breaths each minute. For others, it’s slow and irregular where they may breathe three breaths and then wait 45 seconds to take another breath.
Some patients breathe very fast, then slow down, pause, breathe fast again, and so on. This is a normal end-of-life breathing pattern called Cheyne-Stokes respiration. It can occur when the brain forgets to trigger breathing.
When you reach your final breaths, agonal breathing is common. Agonal breaths look like the patient is trying to gulp for air and can be distressing to loved ones if they’re unfamiliar with it. Nurses sometimes nickname it “guppy” breathing because the mouth opens wide and the jaw and shoulders work to pull oxygen into the lungs.
When the diaphragm and other muscles weaken, phlegm builds up in a dying patient’s airways, making a rattling sound when they breathe. This is known as the “death rattle.” If this rattle occurs to you, it will not feel uncomfortable, but the sound can be distressing to loved ones. Your caregivers may reposition your body or your neck to reduce the rattle.
If a medication like atropine is given at the beginning of your final days, it may improve the death rattle later when it occurs in your final hours.
These breathing changes – even agonal breathing and the death rattle – rarely, if ever, cause discomfort. They are a normal part of dying and occur when you are in a relaxed and unconscious sleep.
If your breathing does look painful, very labored, or very rapid, your loved ones or nurses will give you a medication like oral or I.V. morphine, because the labored breathing may be a sign of pain. Morphine is typically the end-of-life pain medication of choice because it not only dulls the pain but also eases your breathing.
You may want to continue wearing oxygen as you reach the end. In most cases, it will not lengthen your life significantly during the final days, but some people find it comforting.
9. Heartbeat and blood pressure changes
Changes in your heartbeat and blood pressure will also occur. Your heart rate may become irregular and eventually weaker as your heart fails. These are normal changes and are not treated at the end of life. To de-medicalize the dying process for the patient and their loved ones, most medical providers will stop monitoring vital signs during a patient’s final days.
Facing death takes profound courage. If you have an incurable illness and know death approaches, gather your loved ones and your medical team around you. Consult with a palliative care specialist sooner than later to help you through the journey. Be sure to talk openly with them about tough topics such as what it’s like to die and how they can help make you comfortable.
Patients want comfort and peace at the end of life, but each one defines this differently. Death is a deeply personal journey, and more than anything when facing death, patients want medical providers and loved ones to hear and value their unique needs.
By Sharleen Lucas, RN
Dying patients want comfort and peace. Each patient defines this differently, but there are 7 common requests they make.
They want dignity and open talks about their illness and their treatment.
They want to be comfortable.
They want relief from burdens, time with loved ones, and a legacy that outlives them.
They may even want to die alone.
Death is a sacred journey, unique to each person. Knowing what a dying loved one wants is what matters.Patients with advanced illnesses may have a few days or years to live. The phrase “end-of-life” refers to the final stage of an incurable disease or injury. A time frame does not define this last stage of life because it’s a unique journey for each person.
“Every death journey follows along the same path in different ways,” explains Delta Waters, a death doula, and registered nurse. Like birth, each patient has unique symptoms and desires.
Patients, end-of-life specialists, and researchers agree on these seven common requests from dying patients.
1. Dignity
Dignity refers to a person’s inherent nobility and worth. Respecting a patient’s dignity is one of the most common values held by patients, loved ones, and medical providers alike.
But dignity is not an objective, one-size-fits-all concept. It means something different to each person.
“To most end-of-life patients, dignity means, ‘Until my dying breath, I feel like you treat me as if I’m alive and cared for,'” said Beth Patterson, a certified end-of-life doula, and veteran palliative care chaplain.
To one patient, feeling alive and cared for might mean staying on a life-saving machine until they die. To another, however, removing devices is more dignified. Some patients may want a family member to care for their bodily needs, while others may hire an objective caregiver.
Either way, honoring a patient’s wishes whenever possible is the best way to honor their dignity.
2. Open talks
When you’re well, you don’t care to talk about sickness. But when you’re sick, almost everyone wants to talk.
Most patients want frank discussions, but some don’t, asking doctors to give the hard truth to their loved ones instead. Many want to know how the medical team will treat their pain and symptoms. A few want to know what the end will be like. Sometimes patients want advice on talking with family or finding meaning in their final days.
Studies confirm that when medical providers talk openly with patients and their loved ones about their dying journey, it improves the quality of life for the patients and their families. It also decreases excessive treatment – which often causes greater patient suffering.
The 2011 study in California found that a quarter of Californians faced language issues with their medical providers, drastically reducing their quality of care. To prevent this, medical providers are required to provide interpreters.
But not all talking needs to be about a patient’s end-of-life treatment, Waters told me. A simple chat over a cup of coffee about whatever comes to their mind helps dying patients feel normal.
3. Comfort and symptom relief
It’s not surprising that dying patients want to be comfortable. Most importantly, comfort means symptom relief, but it also includes how and where they want to die. Most people prefer to die a natural death at home rather than in a hospital connected to machines.
Common end-of-life symptoms include pain, shortness of breath, increasing weakness, anxiety, nausea, loss of appetite, and thirst. Some patients want these symptoms controlled to the point where they mostly sleep. Others choose to endure some discomfort to be awake with loved ones.
The goal of symptom relief is comfort – as defined by the patient. Not clearly understanding a patient’s symptoms and desires for comfort can increase their suffering.
4. Relief from burdens
End-of-life patients worry about their families, their finances, and what the end is like. Most of all, dying patients want to know their loved ones will be okay.
One of the best ways to ease these burdens is hospice care. Hospice offers holistic care and counseling for patients facing their last six months of life. With care provided by nurses, aides, medical social workers, counselors, and volunteers, hospice is typically free of charge thanks to Medicare coverage and hospice fundraising.
Sadly, however, most patients wait too long to start hospice. Instead of using hospice for their last six months of life, about 50% of patients only use it for their final 18 days or less.
Contacting hospice sooner helps relieve patients and loved ones of their worries. At a time when every day counts, hospice may even lengthen patients’ lives for up to 29 days.
5. Time with loved ones
Most dying patients want to spend as much time as possible with loved ones. Many want to strengthen relationships, resolve old hurts, and pass on love, wisdom, and stories.
In his book, Dying Well, Dr. Ira Byock says there are five necessary statements to say to your loved ones at the end of life.
Forgive me
I forgive you
Thank you
I love you
Good-bye
These statements help relieve the spiritual and relational burdens of both the dying and their loved ones.
6. A legacy
Loretta Bruening, Ph.D., founder of the Inner Mammal Institute, writes, “You are hard-wired to care about what you leave behind when you’re gone…The neurochemistry that drives animals to promote their genes is what drives you to care about your legacy. Understanding that is important to your happiness.”
Contributing to others and leaving a legacy is called generativity in psychology. It refers to the need of humans later in life to leave their mark. They want to create something that will live after they die.
End-of-life studies support this, saying dying patients show a need to contribute to their community to feel needed, significant, and remembered. Some patients create gifts, start projects, continue to work or make financial donations. Others offer time and knowledge to their community and loved ones.
After working with thousands of dying patients, Patterson knows the importance of a legacy unique to each person. She told me about one patient who left a legacy of “words and actions” by earnestly creating videos for his wife and the first responders he led as captain of the fire station. In contrast, Patterson also recalled a Buddhist coworker who felt no need to create a legacy because her “life was her legacy.”
7. Maybe to die alone
As Waters reminds us, “In the end, even though death is a universal human experience, it’s still a solitary journey for each person.” And some want it that way.
As an RN, I cared for a dying patient in the hospital who lived days longer than his family expected. At age 90, with a failing heart, we thought death would come quickly. His family sat with him each day, taking turns at night. They grew exhausted after several days but were grateful to be with him.
They wondered why he held on so long. We discussed that perhaps he wanted to die alone, so the family decided to go to dinner together, leaving the patient with our staff for an hour.
Not long after they left, his breathing changed and slowed, eventually stopping before the family returned.
Patients who want to die alone are common, according to hospice staff and death doulas. It can be hard on loved ones, but letting patients die alone if they want to is another way to honor their wishes and dignity.
There’s no “right” way to die. Death is an individual’s sacred and one-of-a-kind moment. What matters is honoring each patient’s unique dignity and desires.
— Three professionals who work with death and dying have described the one thing they all have in common.
By Bek Day
Woody Allen famously said “I’m not afraid of death, I just don’t want to be there when it happens,” and whatever you think of the scandal-plagued filmmaker’s behaviour in life, it’s a sentiment many can agree with.
“We live in a death-denying culture,” says Dr Merran Cooper, who is also trained as an end-of-life doula and physiotherapist. “By denying the possibility we might die, and having conversations about it, we deny ourselves the opportunity to have the most important conversations of our lives with the most important people.”
But just what are those all-important final moments like for people? Is death really as frightening as we think?
News.com.au spoke to three professionals who work with death and dying and their descriptions all had one major thing in common: it’s usually more peaceful than you might expect.
Camilla Rowland, CEO of Palliative Care Australia
“My experience has been that usually as the different organs start to shut down, people come in and out of a semiconscious state, and it is usually very peaceful,” Camilla explains, adding that the feeling of someone’s ‘spirit’ ‘energy’ filling the room is also common.
“I’ve had that experience, and also many other members of my palliative care team have said that as well, that they felt the spirit of the person around them. And that’s not necessarily a religious thing, it’s just a feeling that occurs. I’ve had people from all walks of life and all different belief systems say the same thing.”
Patsy Bingham, Death Doula
“Peace, calm, relief, hysteria – there could be any one of these feelings depending on who died, how they died and whether they were too young to die,” explains Patsy.
“But for everyone, it is a defined moment in time, and I have a habit of looking at the clock when someone takes their last breath, as family members don’t, and then ask later.”
Dr Merran Cooper, CEO of Touchstone Life Care
“Everyone dies differently but most commonly, when death is expected, a person begins to sleep more, and breath more shallowly until it is very hard to tell whether they are breathing or not,” Dr Cooper explains.
“It can be a peaceful thing to watch. There are noises that worry the person watching, and even bleeding which is distressing to watch, but for the person dying, they slowly move to a place of deeper and deeper unconsciousness until they do not take the next breath.”